
Abstract
Background:
Globally, hypertension rates are rising, particularly in low-income nations where access to healthcare and education remains limited. In the Dominican Republic, marginalized Haitian migrant communities, known as Bateyes, face disproportionate burdens. However, limited information exists on their understanding of hypertension and related health risks. This program-based evaluation aimed to explore community knowledge as part of ongoing outreach efforts.
Methods:
We conducted a descriptive analysis of responses from 379 adults across three Bateyes in the Puerto Plata region. Participants completed a 15-item hypertension knowledge questionnaire during a routine mobile medical screening program (December 2022-January 2023) coordinated by the Kerolle Initiative. Hierarchical clustering was used to identify knowledge patterns and explore associations with community differences and systolic blood pressure (SBP) levels.
Results:
Average BP values were 133/84 mmHg for males and 125/84 mmHg for females, with 27% of respondents meeting the clinical threshold for hypertension. Knowledge levels varied with 44% of participants having insufficient knowledge, and only one participant demonstrating adequate knowledge. Knowledge was associated with education level and household income. Poor awareness of basic concepts emerged as a key driver of variation across Bateyes. Cluster analysis revealed three knowledge patterns: (1) awareness shaped by lived experience of hypertension; (2) gaps due to common misconceptions; and (3) protective behaviors likely influenced by broader public messaging.
Conclusion:
Findings from our educational outreach program evaluation suggest variable hypertension awareness across Batey communities. These observations highlight key areas for tailoring future community-centered health education efforts to the local needs of Bateyes.
Introduction
Hypertension, or elevated blood pressure, is a key modifiable risk factor for cardiovascular disease that has negative impacts on patients’ physical, and mental health outcomes, as well as their overall well-being. It can lead to various conditions including congestive heart failure, cerebrovascular disease, and coronary heart disease. 1 Individuals with hypertension are reported to have a shorter life expectancy by 2 to 5 years, losing an average of 5.1 years for men and 4.9 years for women compared to those without hypertension.2 -4 Hypertension can be prevented by adopting lifestyle modifications that include quitting tobacco and alcohol, leading an active life, reducing sodium intake, and maintaining optimum body mass index and body fat percentage. 5
Over the last three decades, the global prevalence of hypertension has doubled, primarily in middle and low-income countries, largely due to inadequate patient education and substandard healthcare practices.6,7 In the Dominican Republic, a middle-income Caribbean country, around one-third of adults are estimated to have hypertension. 8 However, this proportional burden increases as socioeconomic status decreases, with a prevalence rate of approximately 57% in the poorest, most rural, and remote regions of the island.9,10 Among the 30% of Dominicans living in extreme poverty, the Bateyes or Haitian migrant communities, are among the most impoverished. Their socioeconomic challenges result from a combination of governmental neglect, anti-Haitian sentiment, and the decline of the Dominican sugarcane industry, which has been a primary source of these communities’ livelihood. 11
Despite hypertension being the second most common diagnosis in the Dominican Republic, there is a scarcity of data on its prevalence in these remote communities. 12 To our knowledge, no prior studies have documented awareness and knowledge of hypertension risk factors and symptoms within these communities. This program evaluation, conducted as part of an annual outreach campaign, aimed to assess community awareness of hypertension-related health issues in three Bateyes in the Puerto Plata region of the Dominican Republic. The primary goal was to inform and tailor local health education and outreach efforts led by the Kerolle Initiative. While not designed to produce generalizable or extrapolatable findings, we believe these observations may be informative for other programs serving similarly underserved populations in the Dominican Republic and across the Caribbean.
Materials and Methods
Program Evaluation and Classroom Experience
This project was conducted as a program evaluation of an ongoing annual community health outreach initiative and classroom-based educational experience. Data were collected by the Kerolle Initiative for Community Health, a registered non-profit, non-governmental organization in the Dominican Republic. The organization comprises licensed medical professionals and community health workers who have provided free basic healthcare and educational outreach to rural and Batey communities since 2006. Under local regulations, the Kerolle Initiative has institutional authorization to conduct non-interventional, community-based evaluations, including routine health screenings and knowledge assessments to support program development and internal staff training. Accordingly, this program evaluation was approved by the advisory and executive boards of the Kerolle Initiative. Approval from the national bioethics commission, Consejo Nacional de Bioética en Salud (CONABIOS), was not applicable, as the knowledge assessments were not interventional in nature, were not of national scope, and were not conducted by an academic entity for research purposes.
Since 2016, the University of South Florida (USF) Judy Genshaft Honors College has partnered with the Kerolle Initiative through faculty-led, community-engaged study abroad programs. These collaborations have resulted in a range of applied public health education outcomes, including publication of bilingual healthcare infographics (in Spanish and Kreyol), a nutrition guide for pregnant women, community gardening initiatives, and community health program evaluations for several non-communicable diseases. These experiences are integrated into student coursework to enhance experiential learning and cross-cultural understanding of community health. For this evaluation, the hypertension knowledge questionnaire was administered during the Kerolle Initiative’s regular mobile health clinics between December 2022 and January 2023 in three Batey communities.
The primary goal was to assess prevalent misconceptions, practices, attitudes, and awareness concerning hypertension, its risk factors, and prevention. Thus, the questionnaire functioned both as a patient education tool by identifying knowledge gaps and a training resource for health workers. All participants provided both verbal and written informed consent and were informed that their anonymized responses could be used for health education, program evaluation, and classroom experience purposes. No personal identifying information (eg, names, phone numbers, ID numbers, or specific community names) was collected. Participation in the evaluation was voluntary and not a requirement to receive medical care.
The USF faculty and students participated in the digitization and analysis of de-identified questionnaire forms as part of a classroom-based educational activity. Based on the results, a community health handbook and visual flyers were created and distributed to support community and internal education efforts. Prior to manuscript preparation, the USF Institutional Review Board (IRB) was contacted for guidance. Based on the IRB’s criteria and the nature of the project, it was determined that this activity met the definition of non-human subject research, categorized as program evaluation, and classroom-based learning. As such, formal IRB submission was not required, and retrospective IRB approval was not applicable for this type of activity. Furthermore, no generalizable outcomes were intended or derived from this work; the insights presented are grounded in the specific context and observations from the evaluated communities.
Sampling Characteristics
We reviewed de-identified medical records and responses to the hypertension knowledge questionnaire collected by the Kerolle Initiative. Adults aged 18 and older who were living full-time in one of the three Dominican Bateyes in the Puerto Plata region were included in the program evaluation. To protect the privacy of these vulnerable communities, we referenced them as Batey A, Batey B, and Batey C throughout the manuscript. These Bateyes were selected by the Kerolle Initiative based on logistical feasibility, including transportation access, and the presence of established relationships with the local community health workers. These Bateyes have participated in similar outreach and evaluation activities for over a decade as part of the Initiative’s annual program cycle. Data were excluded if the participants were under the age of 18 or were not known to live in the designated communities.
Screening of Records
The following demographic information was extracted from the participants’ medical records as part of routine screening—age, gender, weight, marital status, highest level of education, occupation, socioeconomic conditions, history of smoking and alcohol consumption, and the latest blood pressure (BP) readings. Blood pressure values were recorded in the clinic records as the average of two consecutive measurements, taken approximately 15 minutes apart, following standard clinical procedures. For descriptive purposes, the BP readings were classified as hypotensive (⩽89/59 mmHg); normotensive (90/60-120/80 mmHg); prehypertensive (121/81-139/89 mmHg); Grade I hypertension (140/90-159/99 mmHg); and Grade II hypertension (⩾160/100 mmHg). 13
Hypertension Knowledge Survey
The adapted hypertension knowledge questionnaire used in this evaluation has been validated in multiple previously reported studies (Supplemental File 1).14,15 The printed, paper-based survey included 15 dichotomous (Yes/No) questions focused on common hypertension risk factors, symptoms, and prevention strategies. Participants were also given the opportunity to briefly explain their responses, allowing for additional qualitative insight during the interactions. The survey was administered in the language most comfortable to each participant, with assistance from a community health worker and an interviewer. These interactions also served as opportunities for personalized health education discussions with participants and, when appropriate, their family members. For internal evaluation purposes, participant responses were pooled into a simple cumulative score out of 15 points, reflecting the number of correct answers. Based on prior applications of the tool, scores were categorized as follows: ⩽ 8 indicated insufficient knowledge, 9 to 12 indicated average knowledge, and 13 to 15 indicated sufficient knowledge.14,15 These scores were used descriptively to understand knowledge gaps and strengths in awareness across the three Batey communities.
Statistical Analysis
Quantitative variables (age and weight) were assessed for distributional characteristics using Shapiro-Wilk test and Q-Q plots. Both variables were found to be non-normally distributed and hence non-parametric tests were used in descriptive and comparative analyses. For categorical variable with two groups, the Mann-Whiney test was used while for 3 or more groups, the Kruskal Wallis ANOVA was used. For associations between categorical variables (nominal variables), the Chi-squared test was used. Fisher-Freeman-Halton Exact was used in case of violations of the requirements for Chi-squared test. For assessing the distribution of nominal variables across ordinal variables, the Kruskal Wallis ANOVA was used. The significance level was set at P < .05. All analyses were performed using IBM SPSS Statistics for Windows 11 v29.0. 2023, IBM Corp: Armonk, NY, USA.
Additionally, we conducted Multiple Correspondence Analysis (MCA) to explore the relationships and clustering patterns among categorical variables, specifically, participants’ responses to the 15 hypertension knowledge questions. MCA allowed for dimensionality reduction and visualization of the similarity or dissimilarity in response patterns across the different Batey communities. This analysis also helped us to identify key thematic groupings of questions that contributed most to knowledge variation between communities. Following MCA, Hierarchical Clustering (HC) analysis was applied to the same set of knowledge questions along with their correlation with systolic BP readings to group them into thematic clusters. This approach allowed us to identify natural groupings of questions based on how participants answered them, revealing patterns such as questions tied to personal BP experience, widespread misconceptions, and universally understood protective behaviors. Spider (Radar) plot was generated to depict relative strengths and gaps in hypertension knowledge by community, as a tool for informing future education and outreach content development.
Results
A total of 379 participant records met the inclusion criteria—95 from Batey A; 94 from Batey B; and 190 from Batey C. This sample represented all adults who attended the Kerolle Initiative’s scheduled annual mobile health clinics between December 2022 and January 2023, and who voluntarily participated in the hypertension awareness screening and education activity. This reflects a convenience sample, as participants self-elected to attend the clinics and completed the survey during their routine health clinic visits. Among the 379 participants, 65% identified as females, and more than two-thirds of the respondents reported they were currently not involved in a relationship. There were no significant associations observed between gender, marital status, and the sampled Batey (Table 1).
Descriptive Demographic Overview of the Respondents in the Study.

Abbreviation: FFH, Fisher-Freeman-Halton Exact test.
Statistical notes—responses marked as “missing” were treated as empty data (ignored) for the Chi-squared test (Χ2) or the Kruskal Wallis H test.
Quantitative Variables
The median age of the participants was 35 years (range 18-100 years) with no significant differences in the distribution across the different Bateyes (Kruskal Wallis H = 1.274; P = .529). The median age was 38.5 and 34 years, respectively for males and females (Mann-Whitney U = 15 639; P = .456). The median weight of the participants was 64.9 kg (range 32.7-126.5 kg) with no significant difference in the distribution across the different Bateyes (Kruskal Wallis H = 1.861; P = .394). The median weight for males was 67.1 kg while for females was 64.4 kg (Mann-Whitney U = 15 504; P = .107).
Educational and Employment Status
Most of the participants reported having completed only a primary school-level education, with approximately one-fifth indicating completion of high school education. There were no notable differences in distribution of education levels across the Bateyes (Table 1). In terms of employment, two-thirds of the participants (67%) reported being currently unemployed. An association was observed between the employment status and the Batey community (P = .002), suggesting possible differences in local economic opportunities or access to employment across the communities.
Monthly Household Income
In line with patterns observed in employment status, more than half of the participants reported a monthly household income of less than 2000 pesos. Income levels varied substantially across the Bateyes (P < .001), with post-hoc analysis (with Bonferroni correction) showing significant differences in monthly household incomes between Batey B and Batey A (P < .001) and Batey B and Batey C (P < .001). However, there were no significant differences observed between Batey A and Batey C (P = .237). These differences in reported income may reflect underlying variability in socioeconomic conditions, which could have implications for health access, education, and hypertension awareness.
Smoking and Alcohol Consumption
Most participants (85%) reported that they did not currently smoke, although there were significant associations noted with the Batey community (P < .001). Regarding alcohol use, approximately three-fourths (75%) of the participants reported no current alcohol consumption. A significant association between alcohol consumption and the Batey community (P = .042) was observed. These findings suggest community-specific differences in lifestyle choices and behaviors, which may inform future health education efforts.
Blood Pressure (BP) Measurements
The average systolic blood pressure among all participants was 128 mmHg (SD 23 mmHg) while the average diastolic blood pressure measured was 84 mmHg (SD 15 mmHg). When stratified by gender, average blood pressure was 133/84 mmHg for male participants and 125/84 for female participants. Based on the BP grading scale, 45% of the participants fell within the normal BP category, while approximately 27% were classified as pre-hypertensive. An estimated 27% of the participants met the criteria for hypertension (Table 1). There were no significant differences in distribution of BP gradings and the Batey communities (P = .949), suggesting a relatively uniform pattern of blood pressure levels among communities at the time of screening.
Hypertension Knowledge Questionnaire
A detailed summary of the responses to each of the 15 questions in the survey, stratified by Batey, is presented in Table 2. The median number of correct responses was 9 out of 15 (range 4-13), suggesting moderate overall awareness of hypertension-related knowledge within the Bateyes. When classified into categories, 55% of the respondents demonstrated average knowledge, while 44% were classified as having insufficient hypertension knowledge. Notably, only one participant achieved a score to meet the threshold for sufficient knowledge (13 points; Figure 1), highlighting substantial knowledge gaps across the Bateyes and underscoring the need for strengthened, community-based health education efforts.
Results from the Hypertension Knowledge Questionnaire.
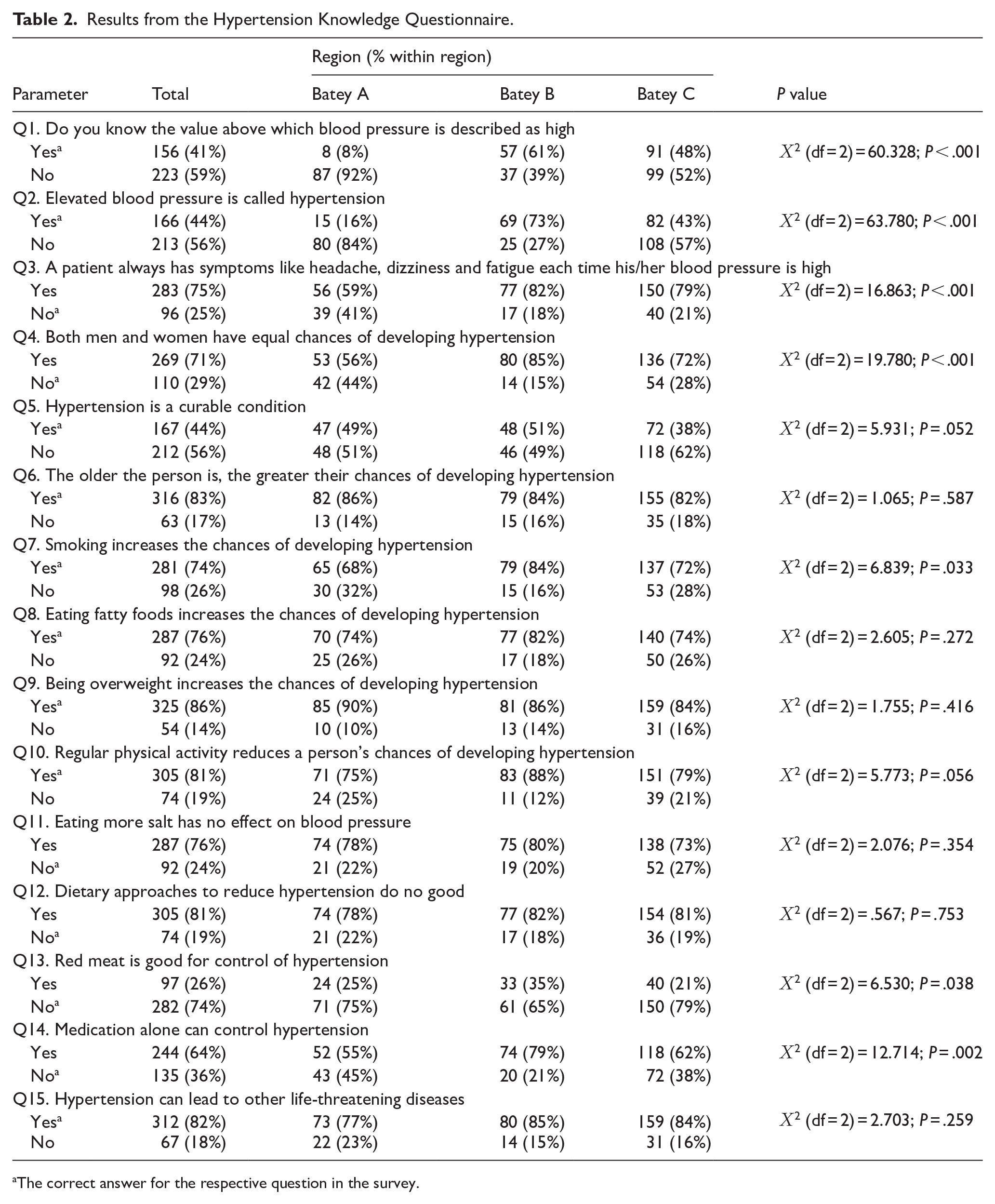
The correct answer for the respective question in the survey.

Distribution of total score on hypertension knowledge questionnaire—red indicates insufficient knowledge (⩽ 8 points); yellow indicates average knowledge (9-12 points); and green indicates sufficient knowledge (13-15 points).
There were observable differences in distribution of respondents based on their hypertension knowledge levels and Batey community, income levels, and highest education level (Table 3), highlighting the possible role of key social determinants such as education and economic status in influencing hypertension knowledge. In contrast, no notable differences in distribution were noted between hypertension knowledge levels and gender (P = .131), marital status (P = .644), occupation (P = .183), smoking preferences (P = .396), and alcohol consumption (P = .656). Similarly, no significant variations in distributions of age (P = .532) or weight (P = .599) across different levels of hypertension knowledge were observed.
Differences in Distribution of Respondents Based on Hypertension Knowledge Classes and Select Demographic Parameters Which Were Found to Have Significant Results.

Survey Items Driving Response Differences Across Bateyes
To explore patterns in hypertension knowledge across communities, we conducted Multiple Correspondence Analysis (MCA) for dimension reduction and to identify possible associations between individual survey responses and Batey community. The goal of this analysis was to detect response patterns and question items that may help inform future, Batey-specific educational interventions. MCA results revealed that Dimension 2 captured the most notable contrast between Batey A and B (v.test = −6.71 and 4.84, respectively). This contrast was primarily influenced by participants’ responses to
On the other hand, dimension 3 revealed the greatest difference between Batey A and C (v.test = 2.43 and −2.33, respectively), particularly in responses to

Multiple correspondence analysis (MCA) of individual survey responses by Batey. The left panel shows the distribution of individual responses from participants in Batey A (purple), B (teal), and C (yellow) projected onto the first 2 MCA dimensions, which together explain 32.9% of the total variance. Each point represents an individual, and shaded ellipses represent 95% confidence intervals for the Batey groupings. The right panel displays the contribution of individual survey item responses (correct or incorrect) to the MCA dimensions. The placement reflects the response pattern relative to the Batey distributions.
Patterns in Bateyes’ Knowledge and Mean Systolic Blood Pressure (SBP) Sensitivity
Next, to explore how knowledge themes varied across Batey communities and correlated to mean systolic blood pressure (SBP), we applied hierarchical clustering to group the 15 survey questions into three clusters. The clusters were organized based on their similarity in SBP correlation and correct response rates by Batey and revealed distinct patterns in participant understanding (Figure 3). Cluster 1 included

Hierarchical clustering of survey questions and knowledge patterns by cluster. The left panel displays a hierarchical clustering dendrogram of the 15 survey questions based on four variables: the correlation between correctness and systolic blood pressure (Corr_SBP), and the proportion of correct responses in Batey A, B, and C (Prop_A, Prop_B, Prop_C). Questions with similar patterns across these variables were grouped using Ward’s method on a scaled distance matrix. The resulting dendrogram identified three distinct clusters of questions with shared behavioral profiles. The right panel is a radar (spider) plot comparing the average knowledge pattern across the three question clusters. Each axis represents one of the input variables used for clustering—Cluster 1 (red), Cluster 2 (blue), and Cluster 3 (green).
Cluster 2 consisted of
Cluster 3 comprised a broader mix of questions, including lifestyle-related (
Discussion
Hypertension is a significant contributor to long-term cardiovascular damage and increased morbidity and mortality rates. The patterns observed in our program evaluation demonstrate the urgent requirement for comprehensive educational programs designed to address the knowledge gap pertaining to hypertension in Dominican Republic Bateyes. Our findings suggest that participants had inadequate knowledge about hypertension, which could have played a significant role in participants’ elevated blood pressure levels. These results are in line with previous studies that have shown that individuals living in regions with higher burden of hypertension generally exhibit poorer hypertension knowledge,16 -18 implying that education plays a decisive part in a community’s susceptibility to hypertension.
The population surveyed had a median age of 35 years. As the age of the public increases, data suggests that the likelihood of developing hypertension also rises. 13 The average blood pressure among males, which was measured at 133/84 mmHg, indicated that men may be more susceptible to pre-hypertension, and hypertension development than females in the Batey population, in line with global trends.19 -21 Potential causes of elevated blood pressure among Batey community members may arise from the increasing consumption of processed food products in the Dominican Republic that contain high levels of salt and saturated fats. 22 Interestingly, when surveyed, a quarter of the respondents claimed that consuming fatty foods did not lead to an increased risk of hypertension, while three-quarters believed that high salt intake did not have adverse effects on blood pressure.
Upon first observation, these responses may be attributed to the local cuisine, which is rich in deep-fried foods such as plantains and meats. Such diets could lead to excessive caloric intake and trans-fats consumption, thereby contributing to hypertension and cardiovascular complications. 23 Cheap, processed, heavily salted, fried, and low-quality foods are ubiquitous in the Batey communities due to structural conditions limiting access to quality food. Noticeably despite their dietary practices, the participants had a median weight of only 64.9 kg, a result of poverty and minimal access to balanced nutritional meals. To minimize the risk of developing hypertension, respondents had been advised to avoid consuming foods high in trans- and saturated fats. However, such advice often has implementational challenges since a healthy diet may be out of reach for most of the participants.
The link between dietary sodium intake and hypertension is strongly supported by multiple research studies and is known to be a significant contributor to the elevated blood pressure levels in Batey communities. 24 On average, Dominicans consume 7.3 g per day (g/d) of sodium, which exceeds the World Health Organization’s recommended daily intake level of 5 g/d. Compared to other Caribbean countries, the average Dominican consumes slightly more sodium (Caribbean average = 7.27 g/d). Our on-ground observations have shown that the Batey communities may consume even more salt than other communities in the Dominican Republic due to the absence of other seasoning options and condiments.
The Dominican Republic was rated as Level 1 on the Sodium Country Score Card, which is the lowest of the 4 levels used to assess a country’s implementation of policies and measures to decrease sodium consumption among citizens. This rating is lower than most other regional Caribbean countries. 25 Such findings emphasize the significant amount of effort the government of the Dominican Republic can dedicate toward reducing salt intake among their population, further bolstered by the results of our program evaluation that showed a significant knowledge gap regarding the link between salt consumption and hypertension.
There are multiple evidence-based diets that aim to prevent hypertension, such as the Dietary Approaches to Stop Hypertension (DASH) diet.26 -29 The DASH diet highlights the intake of fruits, low-fat dairy, and vegetables while reducing the intake of saturated and total fats. The DASH diet led to a noteworthy reduction in systolic blood pressure at each sodium level and in diastolic blood pressure at both intermediate and high sodium levels. 30 Study participants who followed the Mediterranean diet (rich in plant-based food and healthy fats) while consuming nuts had their systolic and diastolic blood pressure levels significantly reduced by 7.1 and 2.6 mmHg, respectively, compared to those on a low-fat diet. 31 Such a diet would benefit the Batey communities if it is made available to them. However, fresh fruits, vegetables, and other quality foods are currently out of reach for most Bateyes. The implementation of community gardens alongside dietary education would increase access to healthy eating practices.
Most respondents correctly identified that an unhealthy accumulation of body fat increases the risk of developing hypertension. The Body Mass Index (BMI), which measures obesity, was 27.56 kg/m2 for women and lower for men at 25.69 kg/m2 in the Dominican Republic.32,33 However, the same is not true for the Batey communities. The Batey communities exist without many of the benefits of Dominican citizens, including access to education, healthcare, and employment. 34 These factors also impact access to food, resulting in greater instances of malnutrition as opposed to increased BMI. For this reason, health campaigns for Batey communities must consider the social determinants of health that lead to a particular health condition. Increased BMI and malnutrition may both lead to hypertension, so differentiating the causes is crucial to developing future tailored interventions.
Many participants in our program correctly identified smoking as a risk factor for developing hypertension. This highlights the widespread awareness within this population regarding the negative impact smoking has on hypertension. Smoking causes abrupt increases in heart rate and blood pressure, eventually leading to malignant hypertension. 35 Additionally, smoking has harmful effects on the cardiovascular system, which can contribute to cardiovascular morbidity, mortality, and coronary heart disease. 36 Given its negative health impacts, participants may have felt pressure to deny smoking due to the associated societal stigma. Studies have shown that smokers often face discrimination, which may cause them to misreport their smoking status.37,38
This response bias can lead to under-reporting of smoking prevalence. Notably, only 15% of participants admitted to smoking in our program. While accurate responses regarding awareness of smoking and hypertension were potentially underreported, it is important to avoid overgeneralization that this awareness entirely deters smoking behavior. Some individuals may continue to smoke due to various underlying factors. Similarly, alcohol abuse presents a comparable scenario among the participants. While alcohol is known to increase the risk of high blood pressure, especially in heavy drinkers,39,40 there may be response bias leading to under-reporting of alcohol use. Even though 76% denied consuming alcohol currently, this number may be lower due to participants inaccurately reflecting their actual alcohol intake.
Lastly, hypertension, also referred to as the “silent killer,” in itself presents a diagnostic challenge as it typically exhibits no symptoms. 41 Only 8.44% of participants responded accurately when queried about the symptoms experienced by individuals with hypertension, signaling limited understanding of pre-hypertensive or hypertensive individuals’ perspectives on their condition. The potential consequences of such ignorance can be unfavorable as the quality of life of patients declines, even when no physical pain symptoms confirm their condition. An additional explanation for this trend may be related to potential confusion caused in the way the question was formulated, leading to unintentional bias in responses or interpretations. Including adverbs that indicate indefinite frequency, such as “always” or “never,” could have created ambiguity for the participants.
The study participants predominantly reported a monthly household income of less than 2000 Dominican Pesos, or 75 US Dollars when adjusted based on purchasing power parity (PPP). It is noteworthy that the average monthly wage in the Dominican Republic is 19 908 DOP or approximately 755 USD (adjusted based on PPP). 42 This stark difference between the study participants and the average population in the Dominican Republic highlights the grave income disparity that exists between the 2 groups. The participants significantly deviated from the typical monthly income of the wider population of the Dominican Republic, highlighting a contributing factor to the increased occurrence of high blood pressure within this demographic. Analogous studies have highlighted a noticeable trend toward increased blood pressure levels in low and middle-income countries, mainly due to limited awareness and limited access to corresponding medical treatments, particularly when compared to high-income countries. 43 Further evaluations should look specifically at subaltern groups that exist within low and middle-income countries, such as Bateyes, as they experience extreme poverty, dangerous conditions, and little to no access to medical care.
Limitations
The observations drawn from this program evaluation should be interpreted within the context of certain limitations. The use of convenience sampling by the Kerolle Initiative may have introduced sampling bias, resulting in a partial representation of the broader Batey populations. Individuals who did not attend the mobile clinics or who declined participation may differ in their hypertension knowledge or risk factors, potentially influencing the overall knowledge distribution observed in this evaluation. For example, the proportion of participants classified with hypertension in our sample was not notably higher—and in some cases appeared lower—than national estimates for the Dominican Republic, despite the known socioeconomic disparities affecting Batey communities.10,11 This pattern may be partially explained by the relatively young age of the sample, as well as the possible under-representation of older adults, who may have been less likely to participate due to mobility challenges, limited clinic attendance, or reluctance to engage in survey-based activities. Furthermore, we didn’t undertake any sample size or power analysis calculations as convenience sampling was used and due to the retrospective nature of our analysis.
Nonetheless, it is important to note that the Kerolle Initiative serves as the primary source of health education and services for these communities. As such, individuals sampled through this outreach may have relatively greater health exposure than those not engaged with the program. Nevertheless, the inclusion of data from 379 individuals provides a substantial sample for descriptive community-level insights. An additional challenge may arise from variations in participants’ educational levels, as most reported attaining only primary school education which may have influenced their ability to understand certain survey questions. This pattern was expected among residents of the Bateyes, where access to formal education beyond the primary level is often limited, especially for non-citizens of the Dominican Republic. Finally, while the program evaluation focused on knowledge and behavior, it did not assess psychosocial factors such as chronic stress, which is known to influence both hypertension risk and health decision-making. Broader systemic challenges such as poverty, food insecurity, and institutional surveillance may contribute to underlying health disparities in these communities. 44 Such factors should be considered in future evaluations and program planning.
Implications for Public Health Education
There is an urgent need for programs that are carefully tailored to align with the unique characteristics of the local Batey populations. It is crucial for future initiatives to prioritize the creation of health campaigns that account for the social factors contributing to health concerns and utilize local experts to shape programs effectively. Additionally, health campaigns should use a diverse range of communication strategies, including available media channels, community organizations, workshops, and community leaders such as community health agents. Given the lack of knowledge about modifiable risk factors, campaigns ought to concentrate on educating the public about the modifiable risk factors that are linked to hypertension and offer feasible changes given the available resources.
Such a program would grant individuals the ability to make informed decisions pertaining to their cardiovascular wellbeing. Furthermore, collaborations with healthcare providers, community leaders, and educators can significantly enhance the reach and impact of these campaigns. Partnerships with local organizations, schools, and religious institutions present opportunities to leverage trusted community networks and amplify the reach of hypertension awareness messages. Educational programs hold promise as immersive learning experiences that can deepen understanding and promote practical skills.
In addition to proactive educational efforts, facilitating regular blood pressure testing and monitoring is essential. Ensuring convenient access to testing, especially in underserved areas, can contribute to early detection, and intervention, ultimately reducing the prevalence and impact of hypertension. For example, the Kerolle Initiative’s community health agents have blood pressure monitors in each local community. Community members know their local health agent, and they go to them for blood pressure checks. In addition to facilitating educational programs, community stakeholders may identify ways to address some of the social determinants of health that lead to hypertension. For example, some local organizations have implemented community gardens to introduce healthy alternatives to salty, fried foods.
Embracing a family-centered approach, which extends education to households, acknowledges the influence of familial ties on health behaviors. Collaborations with community leaders can aid in organizing events and workshops that engage families in open discussions about adopting healthy lifestyles. Collectively, through prioritizing education, fostering partnerships, and tailoring interventions to the unique context of Batey communities in the Dominican Republic, significant improvements in hypertension awareness, prevention, and management are possible. These initiatives have the potential to positively impact the well-being of the population and lay the groundwork for healthier future generations.
Conclusions
Our program evaluation highlights the urgent need for enhanced community-based educational programs to address hypertension knowledge in the studied Batey communities. Observations from this outreach activity suggest a pattern of limited knowledge of hypertension being associated with elevated blood pressure, with male participants showing higher average BP, aligning with broader global trends. Several knowledge gaps were identified. While participants widely recognized the link between obesity and hypertension, misconceptions surrounding the role of unhealthy fats and salt—both prevalent in the local diet—remained common. Physical activity was generally understood to be beneficial with participants acknowledging the negative health impacts of smoking and alcohol, though under-reporting is possible. Future educational efforts should aim to address these knowledge gaps while also considering the broader social determinants of health that shape health behaviors in these Bateyes. A family-centered approach, supported by partnerships with local leaders and community health workers, may be effective in reinforcing positive health behaviors, and improving hypertension awareness through culturally tailored outreach.
Supplemental Material
sj-docx-1-cic-10.1177_11795468251350224 – Supplemental material for Community-Based Evaluation of Hypertension Awareness and Knowledge Among Underserved Bateyes in the Dominican Republic
Supplemental material, sj-docx-1-cic-10.1177_11795468251350224 for Community-Based Evaluation of Hypertension Awareness and Knowledge Among Underserved Bateyes in the Dominican Republic by Dang Nguyen, Ryan Shargo, Nityanand Jain, Yusuf Qureshi, Lovepriya Suthaharan, Ramez M. Odat, Cameron Sabet, Miyaz Ansari, Hamzah Khuddus, Phat K. Huynh, Michael J. Diaz, Reginald Kerolle, Ernest Kissi Kontor and Lindy G. Davidson in Clinical Medicine Insights: Cardiology
Footnotes
Acknowledgements
The authors would like to acknowledge the invaluable contributions of the community health workers and medical professionals affiliated with the Kerolle Initiative in the Dominican Republic. We are also deeply grateful to the residents of the 3 Bateyes who voluntarily participated in the hypertension knowledge survey and generously shared their time and experiences as part of this community health program evaluation.
Ethical Considerations
This project was conducted as a program evaluation and classroom-based educational activity. In the Dominican Republic, the program was conducted under the authorization of the Kerolle Initiative, a registered NGO permitted to carry out non-interventional community health evaluations. This program evaluation was approved by the advisory and executive boards of the Kerolle Initiative. According to the University of South Florida (USF) IRB guidelines, the program evaluation met the criteria for non-human subject research and was therefore not subject to formal IRB review.
Consent to Participate
We used secondary data, and all personal data of the participants was anonymized. Participation was voluntary, and participants provided both written and verbal informed consent prior to completing the hypertension program evaluation survey.
Author Contributions
DN, RK, LGD conceptualized the present study while DN, RS, YQ, LS, and CS were involved in data collection, investigation, data curation, and validation. NJ and EKK were responsible for data analysis and visual representations. RK and LGD were responsible for methodology, validation, resources, supervision, funding, and project administration. Original draft was written by RS, YQ, LS, RMO, and NJ while MA, HK, PKH, MJD, RJ, NJ, RMO, EKK, and LGD were responsible for revising the manuscript. All authors have read the manuscript and agreed to publication.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.