
Abstract
Regional right ventricular dysfunction with akinesia of the mid-free wall with normal apical motion known as McConnell’s sign is an under-reported echocardiographic finding in the setting of pulmonary embolism. We conducted a literature review and systematic analysis, while describing 2 cases of pulmonary embolism with findings of reverse McConnell’s sign.
Introduction
Different echocardiographic features are described in the literature in the context of acute pulmonary embolism (PE). McConnell’s sign, a regional right ventricular (RV) dysfunction with akinesia of the mid-free wall with normal motion at the apex is a well-known finding in the setting of acute pulmonary embolism. 1 Reverse or paradoxical McConnell’s sign is rarely reported in the literature as a sign suggestive of pulmonary embolism. We present 2 cases of massive/submassive bilateral PE in patients who were found to have hypokinetic RV and normal to hyperdynamic RV free wall motion, indicative of paradoxical McConnell’s sign. The first patient was admitted for small bowel obstruction and subsequently worked up for PE following the development of respiratory symptoms during his treatment course. The second patient presented with symptoms of PE following a lengthy airplane flight and was found to have reverse McConnell’s sign on transthoracic echocardiography (TTE) as well. Both cases had the characteristic finding of RV dysfunction and wall motion changes in the apex and free wall. We also performed the literature review and systematically analyzed this unique pattern of RV dysfunction in the setting of PE.
Case 1
A 67-year-old man presented with abdominal pain and progressively worsening distension over the last few days. His past medical history included tobacco and marijuana use, chronic back pain status post laminectomy, provoked deep vein thrombus, and PE in 1980s, and newly diagnosed invasive squamous cell cancer of the tongue. He was subsequently admitted for small bowel obstruction. He had no fevers, chills, lightheadedness, shortness of breath, or chest pain. His vitals were 128/75 mmHg, heart rate 74/minute, 97% in room air, respiratory rate 18/minute. General Surgery was consulted and recommended conservative management as obstruction was not complete. Computed tomography chest/abdomen/pelvis with contrast revealed large acute pulmonary thromboembolic disease with evidence of right heart strain (Figure 1A and B). There was small bowel obstruction secondary to focal wall thickening within the terminal ileum. No free air was present to indicate bowel perforation.

(A and B) CT angiography of the chest of Patient 1 with arrows indicating pulmonary emboli. (C and D) CT angiography of the chest of Patient 2 with arrows indicating pulmonary emboli. (E and F) Systolic and diastolic transthoracic image of right ventricle of Patient 1 with arrows indicating akinetic apex. (G and H) Systolic and diastolic transthoracic image of right ventricle of Patient 2 showing paradoxical McConnell’s sign.
The PE was thought to be provoked in the setting of active malignancy with given previous history of venous thromboembolism. TTE showed hypokinetic RV apex and hyperkinetic RV of mid-free and basal wall suggestive of paradoxical McConnell’s sign (Figure 1E and F). There was enlargement of RV and the left ventricular ejection fraction was 54%. Intravenous heparin was started. His subacute intestinal obstruction improved with conservative management, and he was discharged home on apixaban.
Case 2
A 59-year-old man presented with pleuritic chest pain and dyspnea on exertion after recently returning to the area following a 5-hour flight. His past medical history included epilepsy and multiple deep vein thromboses. On physical exam, his respirations were mildly labored, and he was hemodynamically stable on room air. Computed tomography angiography revealed extensive non-occlusive thrombi in all major pulmonary arteries (Figure 1C and D). Transthoracic echocardiography showed a hypokinetic right ventricular apex with hyperkinesis of the RV free wall, (reverse McConnell’s sign) (Figure 1G and H). He was started on heparin drip and transitioned to lovenox bridge with warfarin. His respiratory symptoms resolved, and he was discharged with warfarin and instructions to follow up with anticoagulation clinic for INR monitoring.
Discussion
We presented 2 cases of acute PE whose echocardiography revealed paradoxical McConnell’s sign. Different echocardiographic features are designated in literature in the setting of acute PE. The well-known pattern of right ventricular (RV) strain on TTE is McConnell’s sign, which is characterized by regional RV dysfunction with preserved motion of apex with corresponding hypokinesia of the mid and basal free wall, usually described in the setting of acute pulmonary embolism. In a cohort study analyzing 126 patients, this sign was first described by McConnell et al 2 in 1996 that has been used to assist in making the diagnosis of acute PE. It indicates considerable pulmonary perfusion defect and significant hemodynamic instability leading to death; therefore, it contributes to early decision-making with regard to use of thrombolysis. 3 However, reverse or paradoxical McConnell’s sign is rarely reported, and its clinical significance is not known. An analysis of 15 patients diagnosed with McConnell’s sign with echocardiography showed an association with massive thrombus burden. 4 In this specific pattern, akinesia of the apex and hyperkinetic or normal right ventricular mid and basal free wall occurs.
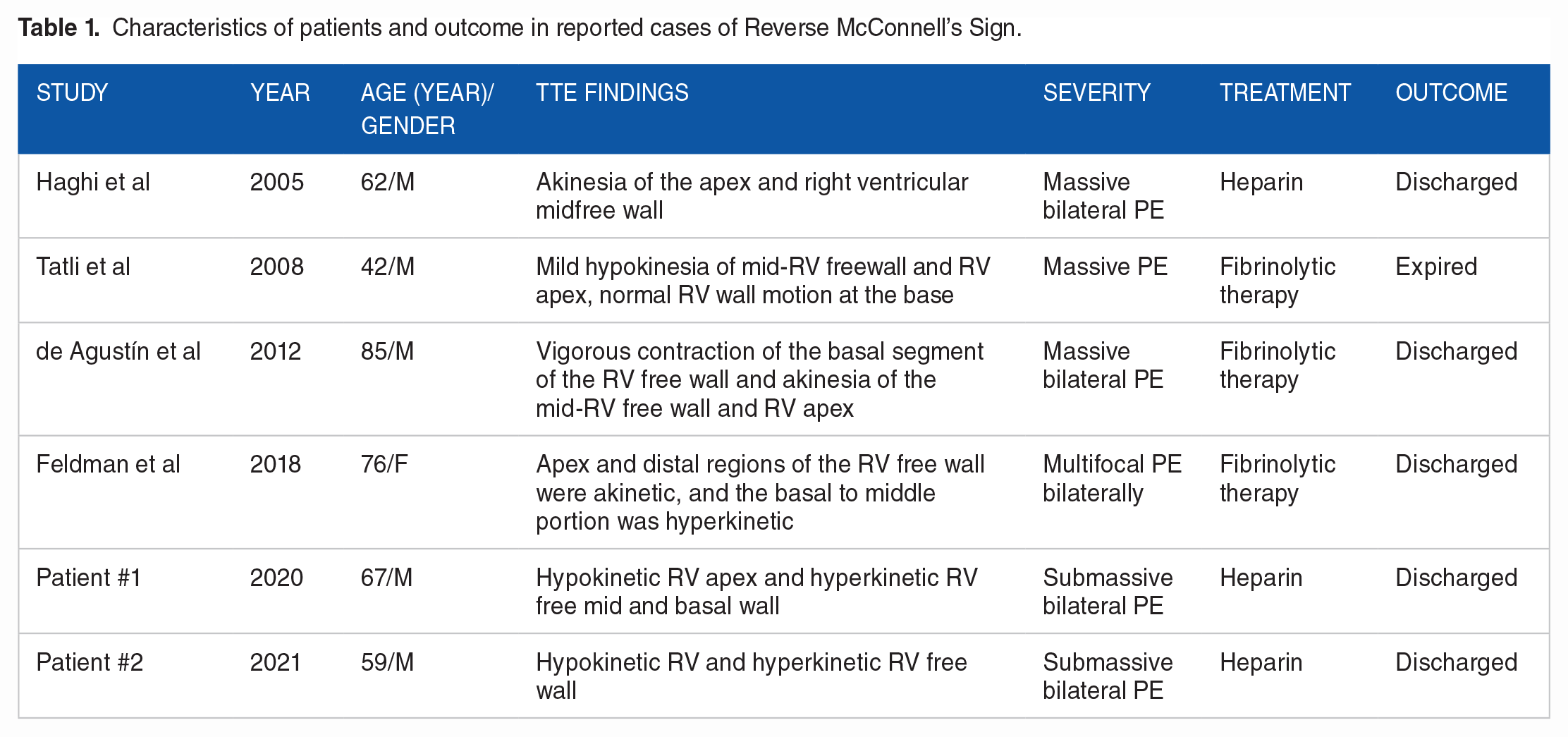
We searched PubMed, Web of Science, Google Scholar, and Cochrane database to identify all potential studies for inclusion from January 2000 to August 2020, while aiming to understand its clinical significance. Keyword and medical subject heading search (MeSH) terms used included “reverse McConnell’s or McConnell sign,” “reverse or paradoxical or inverted McConnell sign and pulmonary embolism,” “McConnell’s sign and pulmonary embolism.” All authors contributed to sort out the disagreement to select final eligible studies. We only included the study which has confirmed PE with CT angiogram. To the best of our knowledge there have been only 4 cases describing this unique pattern of RV dysfunction in the setting of pulmonary embolism (Table 1).5-8 Haghi et al 7 described a case of acute PE in 65-year-old man who developed akinesia of the apex and right ventricular midfree wall which was termed as “reverse McConnell’s sign.” Feldman et al 6 described it in an akinetic apical RV along with a hyperkinetic basal to the middle portion of the RV free wall. Similarly, de Agustín et al 5 and others including ours described the different regional pattern of abnormal RV wall motion abnormalities as reverse McConnell’s sign but had the akinetic RV apex was the common finding. The age of patients in these case reports including ours ranged from 42 to 85 years old, and the male to female ratio was 5:1. Reviewing all the cases, this sign was found to be associated with large PE, mostly requiring fibrinolytic treatment. Only 2 cases were successfully treated with IV heparin. Unfortunately, one case expired during hospitalization despite aggressive treatment (Table 1). 8
Characteristics of patients and outcome in reported cases of Reverse McConnell’s Sign.
Several hypotheses have been proposed to describe the etiology of reverse McConnell’s sign. Although this imaging finding is associated with submassive/massive PE, this sign is likely under-recognized and underreported since it is not yet viewed as an indicator of PE. The momentary increase in right ventricular pressure resulting in ischemia, with variation in the magnitude of it in different myocardial region is thought to be most likely mechanism. 8 Stress response of RV with acute increased in pulmonary vascular resistance and pulmonary perfusion defect may result in variation in regional wall motion abnormalities. The reverse McConnell’s Sign represents the unique presentation of RV dysfunction.
Conclusion
We presented 2 rare cases of reverse McConnell’s sign as unique presentations of RV dysfunction associated with acute PE. This rare, but distinct pattern of RV strain may also be indicative of large PE likely due to regional difference in RV myocardial ischemia. Reverse McConnell’s sign should be recognized as an indicator of PE for timely diagnosis and management.
Footnotes
Acknowledgements
None
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Abbreviations and Acronyms
F female
M male
MeSH Medical Subject Headings
PE pulmonary embolism
RV right ventricle
TTE transthoracic echocardiography
Author Contributions
AS: Wrote and edited all drafts of the manuscript and assisted in literature review. MB: Involved in care of the patient, interpreting echocardiography, literature review, and editing manuscript. AE: Assisted in editing the manuscript and literature review. SH: Involved in care of the patient, interpreting echocardiography, literature review, and editing manuscript.
Informed Consent
With exception of age and sex, no identifying information was used in the manuscript. Informed consent was obtained from each patient for the use of their hospital course and imaging in the creation of a manuscript to be published in an academic journal.