
Abstract
Background:
The appropriate dose of enoxaparin for venous thromboembolism (VTE) prophylaxis in low body weight patients is unknown.
Objective:
The aim of this study is to evaluate the impact of enoxaparin dosing on major and minor bleeding events in low body weight patients.
Methods:
This was a retrospective cohort study of patients weighing less than 45 kg receiving subcutaneous (SC) enoxaparin for VTE prevention. The primary objective was to determine whether enoxaparin dose was associated with major and minor bleeding. The secondary objective was to determine the incidence of VTE by enoxaparin dose.
Results:
There were 173 patients included in the study, of which 37 patients received 2 different courses of enoxaparin during hospitalization, resulting in 210 enoxaparin courses. Among all enoxaparin courses, 16.2% were associated with major bleeding and 5.2% with minor bleeding. There was no difference in the incidence of major bleeding by dose (enoxaparin 30 mg SC daily, 30 mg SC twice daily, or 40 mg SC daily; P = .409). Patients who experienced major bleeding were older (54.9 ± 16.1 years) than patients who did not (48.4 ± 18.4 years) (P = .043). There was no difference in the incidence of minor bleeding by dosing schedule (P = .14). No patients experienced a VTE.
Conclusion and Relevance:
The risk of bleeding was similar by enoxaparin dose but increased with age in low body weight patients. Given the low incidence of VTE in this study, it is reasonable to consider decreasing the prophylactic enoxaparin dose in low body weight patients, especially in the elderly population.
Introduction
Venous thromboembolism (VTE) is a disease characterized by either deep venous thrombosis (DVT) or pulmonary embolism (PE). Possible consequences of VTE include leg pain, chest pain, shortness of breath, chronic post-thrombotic syndrome, and death. 1 There are approximately 150 000 to 200 000 deaths related to VTE per year in the United States. 2 Hospitalized patients have an inherently high risk of VTE. Risk factors for VTE that are commonly present in hospitalized patients include active cancer, reduced mobility, recent trauma or surgery, advanced age, heart failure, respiratory failure, acute myocardial infarction, ischemic stroke, acute infection, and obesity. Studies have demonstrated up to an 11% incidence of VTE in high-risk hospitalized medical patients and as high as 30% in surgical patients; therefore, VTE prevention is a main concern for the health care team.3–5
The most effective means of preventing VTE is by anticoagulant thromboprophylaxis. The primary agents utilized for VTE prophylaxis include unfractionated heparin (UFH) and low-molecular-weight heparin (LMWH).1,2 Recently, direct oral anticoagulants have also emerged as oral options for thromboprophylaxis in surgical and medical patients.6,7 Low-molecular-weight heparin and UFH have similar efficacy for VTE prevention in hospitalized medical patients, but LMWH has been associated with less major bleeding than UFH in several studies.8–12 In surgical patients, studies displayed a reduction in the incidence of VTE with LMWH compared with UFH.13,14 As a result, LMWH may be the preferred agent for VTE prophylaxis in the absence of contraindications. Enoxaparin is the most frequently used LMWH in the United States.
There is literature supporting enoxaparin dosing for VTE prophylaxis in the general population, obesity, and renal insufficiency.15–27 The manufacturer recommends dosing enoxaparin for VTE prophylaxis 40 mg subcutaneously (SC) once daily for the general population or 30 mg SC twice daily in orthopedic surgery patients. In patients with a creatinine clearance (CrCl) of less than 30 mL/min, the manufacturer suggests reducing the enoxaparin dose to 30 mg SC once daily. 15 Although not specifically recommended by the manufacturer, many institutions either increase the enoxaparin dose to 40 mg SC twice daily or increase the dose by 30% in patients with a body mass index (BMI) of greater than 40 kg/m2 based on the results of clinical trials.16–27 However, there is insufficient evidence to determine the appropriate dose of enoxaparin in patients with a low body weight. The manufacturer recommends individualized clinical monitoring of patients with a low body weight, defined as less than 45 kg for women and less than 57 kg for men, but does not specifically recommend a dose reduction due to a lack of evidence in this population. 15 As a result, pharmacists and physicians practice clinical judgment in selecting the enoxaparin dose for VTE prophylaxis in low body weight patients.
Previous studies indicated that a body weight of less than 55 kg was associated with an increased bleeding risk in patients receiving enoxaparin for VTE prophylaxis.28,29 Rojas et al 30 examined the anti-factor Xa activity in patients weighing less than 55 kg and receiving enoxaparin for VTE prophylaxis. Anti-factor Xa levels significantly exceeded the therapeutic range in low body weight patients, especially those weighing less than 45 kg. The results of this study suggest that low body weight patients may have an increased bleeding risk when treated with enoxaparin. However, the association between anti-factor Xa levels and bleeding risk remains controversial. Recently, Sebaaly and Covert 31 performed a literature review assessing enoxaparin dosing at extremes of body weight. No clinical trials evaluated enoxaparin for VTE prophylaxis specifically in low body weight patients. In the absence of clinical evidence, the authors concluded that it is reasonable to reduce the dose of prophylactic enoxaparin to 30 mg SC once daily in underweight patients (BMI less than 18 kg/m2 or body weight less than 55 kg). To our knowledge, there have been no studies comparing the major and minor bleeding events in low body weight patients receiving varying doses of enoxaparin for VTE prophylaxis. It is hypothesized that low body weight patients receiving enoxaparin for VTE prophylaxis have an increased bleeding risk and may require a dose reduction. The literature supporting this hypothesis is limited to studies observing anti-factor Xa levels. As a result, there is a lack of guidance for providers to decide when to reduce the dose of enoxaparin based on body weight. This study was designed to provide preliminary data regarding the rate of major and minor bleeding events in low body weight patients receiving different doses of enoxaparin for VTE prophylaxis.
Methods
Study design and participants
This was a retrospective cohort study of patients with an actual body weight of less than 45 kg who received enoxaparin for the prevention of VTE at a 650-bed community teaching hospital (with associated Level I Trauma Center) between March 1, 2015, and September 30, 2016. This study was approved by the OhioHealth Institutional Review Board (IRB). Informed consent was not required by the IRB because the study involved minimal risk to study participants.
All enoxaparin prescribing is done by physicians, but pharmacists at our institution may adjust enoxaparin dosing per the health-system dosing policy. Among patients with a BMI less than 40 kg/m2 and CrCl greater than 30 mL/min, pharmacists may adjust the enoxaparin dose to 30 mg SC twice daily in trauma patients and 40 mg SC daily in all other patients. Pharmacists may increase the dose to 40 mg SC twice daily in patients with a BMI greater than 40 kg/m2 and CrCl greater than 30 mL/min. Finally, in patients with CrCl less than 30 mL/min regardless of BMI, pharmacists may reduce the dose of enoxaparin to 30 mg SC daily. Although not specifically addressed in the dosing policy, some prescribers reduce the dose of enoxaparin in patients with a low body weight. Pharmacists are not required to adjust the dose to comply with the dosing policy if the lower dose was selected based on the prescriber’s clinical judgment.
Patients were included in the study if they were at least 18 years of age, were treated with enoxaparin for prevention of VTE (enoxaparin 30 mg SC once daily, 30 mg SC twice daily, or 40 mg SC once daily), and weighed less than 45 kg. Patients from all units of the hospital were eligible for inclusion. Patients were excluded if they had a CrCl of less than 30 mL/min upon initiation of enoxaparin or if they were taking oral anticoagulants. CrCl was calculated using ideal body weight unless it exceeded the patient’s actual body weight, in which case actual body weight was used. Demographic and clinical variables were collected retrospectively by a single reviewer from the electronic medical record via manual chart review using a standardized, electronic data collection tool.
Outcomes
The primary outcome was to determine whether enoxaparin dose was associated with a difference in the incidence of bleeding events, with the incidence of major bleeding events and the incidence of minor bleeding events evaluated separately. Major bleeding was defined as a hemoglobin drop of at least 2 g/dL in 24 hours, a transfusion of at least 1 unit of packed red blood cells, bleeding into a critical site (eg, intracranial, intraocular, retroperitoneal, intra-articular, pericardial, or intramuscular with compartment syndrome), or fatal bleeding. Minor bleeding was defined as overt bleeding not meeting the criteria for major bleeding (eg, gastrointestinal bleeding, hematuria, hematemesis, or hematochezia). 32 Bleeding events were collected for the duration of enoxaparin therapy and were attributed to the current dose of enoxaparin at the time of the bleeding event. Secondary objectives included determining the incidence of VTE, defined as a diagnosis of DVT or PE, by enoxaparin dosing schedule and performing subgroup analyses to determine the risk of major and minor bleeding events based on service line, age, gender, BMI, and CrCl. Finally, we compared the incidence of major and minor bleeding by enoxaparin dose among fragile patients. Fragility has previously been defined as 1 or more of the following criteria: age greater than 75 years, CrCl less than 50 mL/min, or body weight less than or equal to 50 kg. 33 As low body weight was a requirement for inclusion in this study, patients were considered fragile if they met at least 1 of the remaining criteria (age greater than 75 years or CrCl less than 50 mL/min).
Statistical analysis
Demographic and clinical characteristics were described using frequencies and percentages for categorical variables and means and standard deviations and medians and ranges for continuous variables. Demographic and clinical characteristics were compared by enoxaparin dosing schedule using Fisher’s exact test for categorical variables and analysis of variance (ANOVA) and Kruskal-Wallis tests for continuous variables.
The incidence of major bleeding, minor bleeding, and VTE was calculated, overall and by dosing schedule. The incidence of major bleeding and the incidence of minor bleeding were compared by enoxaparin dosing schedule using Fisher’s exact tests. Patient characteristics were compared by dosing schedule using Fisher’s exact tests (gender, anti-platelet use, nonsteroidal anti-inflammatory drug [NSAID] use, and service line), ANOVA (age, body weight, height, BMI, and international normalized ratio [INR] on enoxaparin initiation), and Kruskal-Wallis tests (CrCl, serum creatinine, and length of stay). Characteristics of patients who did and did not experience major or minor bleeding were compared using Fisher’s exact tests (gender), 2-sample t tests (age and BMI), and Wilcoxon rank sum tests (CrCl). Statistical significance was set at P < .05 for all tests. Analyses were conducted using SAS 9.4 (Cary, NC, USA).
Results
Patient characteristics
Demographic and clinical characteristics of the 173 patients who received enoxaparin for VTE prophylaxis are presented in Table 1. There were 37 patients in the study who received 2 different courses of enoxaparin during their hospital stay. For example, a patient started on enoxaparin 40 mg daily for 3 days before a prescriber reduced the dose of enoxaparin to 30 mg daily due to a perceived bleeding risk at the higher dose. Therefore, there were 210 courses of enoxaparin included in the study.
Demographic and clinical characteristics in study population.

Abbreviations: BMI, body mass index; INR, international normalized ratio; NSAID, nonsteroidal anti-inflammatory drug.
n (%).
Mean (SD).
Data not available for 2 patients (n = 171).
Median (range).
Data not available for 86 patients (n = 87).
The majority of patients in the study were female (86.1%) with a mean age of 53.6 years, mean weight of 41.5 kg, and a mean BMI of 17.1 kg/m2. There were significant differences in enoxaparin dosing schedule by age (P < .001), body weight (P = .025), CrCl (P = .010), service line (P < .001), and length of stay (P = .002). Patients who received enoxaparin 30 mg once daily were older (Mean = 60.8 years, SD = 12.7) than patients who received 30 mg twice daily (Mean = 38.2 years, SD = 22.4) (P = .005) and patients who received 40 mg once daily (Mean = 53.1 years, SD = 15.2) (P < .001). Patients who received enoxaparin 30 mg twice daily had a higher CrCl (median = 84.8 mL/min, range = 32.2-177.4) than patients who received 30 mg once daily (median = 48.3 mL/min, range = 30-238.2) (P = .022), and patients who received 40 mg once daily had a higher CrCl (median = 69.4 mL/min, range = 30.5-222.6) than patients who received 30 mg once daily (median = 48.3 mL/min, range = 30-238.2) (P = .010). Patients who received enoxaparin 30 mg once daily had a longer length of stay (median = 6.2 days, range = 1.4-80.2) than patients who received 40 mg once daily (median = 4.3 days, range = 1.0-80.2) (Table 2).
Demographic and clinical characteristics in study population by enoxaparin dosing schedule.

Abbreviations: BMI, body mass index; INR, international normalized ratio; NSAID, nonsteroidal anti-inflammatory drug.
n (%).
Mean (SD).
Median (range).
Outcomes
Among all courses of enoxaparin received by patients with a low body weight (n = 210), 16.2% were associated with major bleeding and 5.2% with minor bleeding. There was no difference in the incidence of major bleeding by dosing schedule (P = .409). Of the major bleeding events that occurred in this study (n = 42), the majority were either a hemoglobin drop of at least 2 g/dL (n = 25) or a transfusion of at least 1 unit of packed red blood cells (n = 15). There were also 2 critical site bleeds, both of which were intracranial hemorrhages. There was no difference in the incidence of minor bleeding by dosing schedule (P = .14; Table 3).
Bleeding events and VTE in study population by enoxaparin dosing schedule.

Abbreviations: PRBCs, packed red blood cells; VTE, venous thromboembolism.
n (%).
Other minor bleeding events included bleeding esophageal ulcer (n = 1), bleeding from chest tube (n = 1), bleeding from tracheostomy (n = 1), epistaxis (n = 1), and hemoptysis (n = 1).
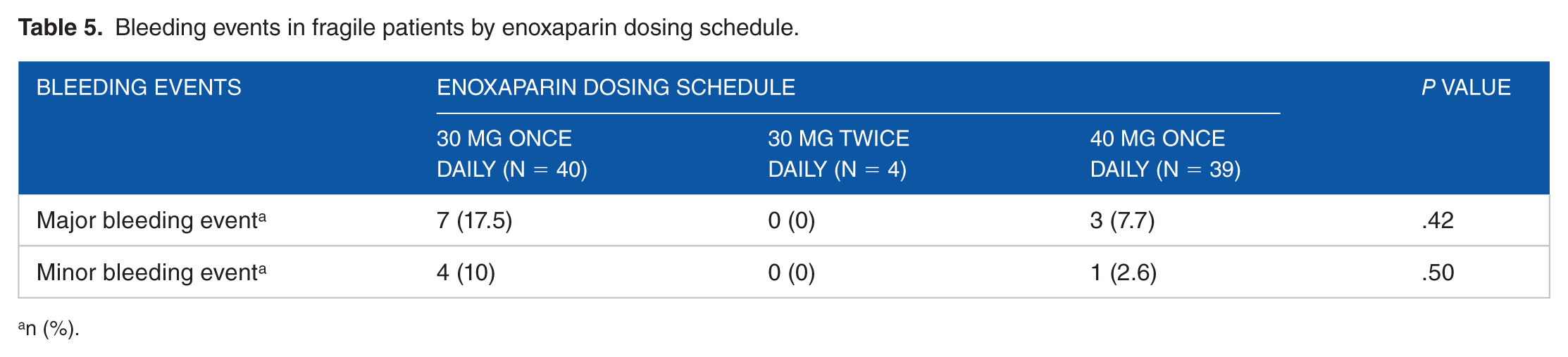
Patients who experienced major bleeding were older (Mean = 54.9 years, SD = 16.1) than patients who did not experience major bleeding (Mean = 48.4 years, SD = 18.4) (P = 0.043). No (0.0%) patients in the study experienced DVT or PE while receiving any dose of enoxaparin for VTE prophylaxis (Table 4). Among the 210 courses of enoxaparin in this study, 83 included fragile patients. The incidence of major and minor bleeding in fragile patients was 12% and 6%, respectively, and there was no statistical difference in major and minor bleeding by dosing schedule (Table 5).
Bleeding events in study population by demographic and clinical characteristics.

Abbreviation: BMI, body mass index.
One patient had a minor bleed on 2 different dosing schedules.
n (%).
Mean (SD).
Median (range).
Cell sizes were too small to perform a valid comparison test.
Bleeding events in fragile patients by enoxaparin dosing schedule.
n (%).
Discussion
Enoxaparin dosing guidelines for VTE prevention have been established for the general population as well as for specific groups such as patients who are obese or who have renal impairment. However, there are no formal, recognized guidelines for dose adjusting enoxaparin in low body weight patients. Rather, dose adjustments are made on a patient-by-patient basis at the clinical discretion of providers and pharmacists. The purpose of this retrospective cohort study was therefore to determine whether the incidence of bleeding events in hospitalized low body weight patients varied according to enoxaparin dosing schedule (30 mg once daily, 30 mg twice daily, or 40 mg once daily).
This study demonstrated an overall 16.2% incidence of major bleeding events in patients receiving enoxaparin for VTE prophylaxis, which is considerably higher than the 1% to 4% incidence displayed in previous studies. 15 It is unclear why this study reported such a high rate of major bleeding events. One potential explanation is that the study institution was a Level 1 Trauma Center, so the patients included in the study may have been higher acuity than the general population. Alternatively, it is possible that low body weight patients have an increased risk of bleeding, particularly major bleeding, relative to the general population at similar doses of enoxaparin. This is supported by a previous study that included low body weight patients who predominantly received UFH for VTE prophylaxis, which demonstrated a 10.5% incidence of clinically relevant bleeding. 34
This study did not demonstrate a difference in the primary outcome between enoxaparin dosing regimens, which was contrary to our hypothesis that patients receiving a lower dose of enoxaparin would have fewer major bleeding events (Table 3). This finding may be due to the differences in baseline characteristics between the 2 groups. Patients who received enoxaparin 30 mg once daily were older, lower body weight, had a lower CrCl, and had a longer length of stay than patients who received enoxaparin 40 mg once daily. Furthermore, this study indicated that the bleeding risk associated with enoxaparin in low body weight patients increases with age. Finally, patients may have received the lower dose of enoxaparin because the prescriber felt they had a higher risk of bleeding. This is supported by the finding that 51% of the patients who received enoxaparin 30 mg once daily were categorized as fragile, compared with 34% of the patients who received enoxaparin 40 mg once daily.
There were several limitations to the study. First, this was a retrospective study. As a result, the investigators were not able to control all potential sources of error. For example, hemoglobin levels were not available daily for every patient, so we were not always able to determine whether there was a hemoglobin drop of at least 2 g/dL. In addition, minor bleeding events likely were not always recorded in the electronic medical record. Second, there was a relatively small sample size given the rare nature of the study outcomes. With this sample size, it is unlikely that we could detect a difference between major and minor bleeding events or VTEs by enoxaparin dosing schedule. Therefore, power was not calculated as the results of the study were intended to be hypothesis generating. Third, a hemoglobin drop of at least 2 g/dL was not always clinically significant. Providers were unable to identify a source of bleeding in some patients who experienced a hemoglobin drop of at least 2 g/dL. However, the International Society on Thrombosis and Hemostasis uses this marker to define major bleeding events. 32 Fourth, patients in this study had variable lengths of stay. Many patients were not in the hospital long enough to experience a major or minor bleeding event or a VTE. We did not adjust the rate of major and minor bleeding events for the length of enoxaparin therapy, which led to an overrepresentation of an individual’s length of stay and enoxaparin exposure. Finally, 37 patients received 2 courses of enoxaparin during their hospital stay. In these patients, the major or minor bleeding events were attributed to the current enoxaparin course regardless of the amount of time the patient was receiving that course.
Conclusion and Relevance
To our knowledge, this was the first study to evaluate bleeding and thrombosis associated with different doses of enoxaparin for VTE prophylaxis in low body weight patients. The risk of bleeding was similar by dose of enoxaparin but increased with age in low body weight patients. Given the low risk of VTE demonstrated in this study, it is reasonable to consider decreasing the prophylactic enoxaparin dose in low body weight patients, especially in patients over the age of 55.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
DD: contributed to project conception and design, collected and interpreted the data, and drafted the manuscript. GW, MP, and DR: supervised the study, contributed to project design and interpretation of the data , and revised the manuscript. CC: analyzed the data and revised the manuscript. All authors: reviewed and approved the final manuscript.
Podium Presentation
Great Lakes Pharmacy Resident Conference; West Lafayette, IN, USA, April 28, 2017.
Poster Presentation
American Society of Health-System Pharmacists Midyear Clinical Meeting & Exhibition; Las Vegas, NV, USA, December 2016.
OhioHealth Research Symposium, Columbus, OH, USA, May 24, 2017.