
Abstract
Objectives:
To identify gaps in knowledge, attitude, and practice regarding the use of corticosteroids and nonsteroidal anti-inflammatory drugs (NSAIDs) among patients with chronic rheumatic diseases.
Methods:
A cross-sectional study was conducted using a questionnaire including 12 knowledge questions, 13 attitude assessment statements, 5 barrier assessment statements, and 7 practical scenarios. We counted the total numbers of correct answers in knowledge, positive attitudes, barriers, and appropriate practices and fitted using Poisson regression to examine factors associated with knowledge, attitudes, and practices.
Results:
A total of 182 participants were included in this study, a large proportion of them had never heard of corticosteroids (34%) and NSAIDs (54%) before. Physicians were the source of information regarding corticosteroids and NSAIDs in 83% and 84% of the cases, respectively. Gastric ulcer was the most commonly recognized adverse drug reaction (ADR) for corticosteroids (64%) and the only ADR recognized for NSAIDs (95%), while only few patients were aware of life-threatening ADRs. The primary barrier, with a 40% agreement, was health care providers’ time constraints in providing medication information to patients. Our study findings did not reveal any gaps in practice, nor did they show any correlation between patients’ knowledge and attitudes to the practice of using corticosteroids and NSAIDs.
Conclusion:
There were gaps in knowledge, attitudes, and barriers to information access regarding NSAIDs and corticosteroid use in Vietnamese patients with chronic rheumatic diseases. Potential solutions include allocating more time for information exchange between physicians and patients, creating new channels to provide reliable information for patients, and emphasizing the important ADRs.
Introduction
Chronic rheumatic diseases encompass a heterogeneous spectrum of systemic and localized conditions impacting both synovial joints and the peri-articular soft tissues, which typically characterized by inflammatory, pain, restricted joint mobility, and in long term, ultimately leading to deformities and functional limitations.1,2 Osteoarthritis represents the most prevalent condition within the noninflammatory category, whereas rheumatoid arthritis and gout stand as the most common pathologies among inflammatory joint diseases. 1 With the aim of reducing symptoms, restoring mobility function, and preventing irreversible joint damage, the use of nonsteroidal anti-inflammatory drugs (NSAIDs) and corticosteroids plays a pivotal role and are widely used in the management of patients with chronic rheumatic diseases.3,4
However, these medications are associated with potential adverse drug reactions (ADRs) in the gastrointestinal tract, cardiovascular system, kidney function, liver, blood pressure, and other systems.3,5,6 In many countries worldwide, NSAIDs and corticosteroids are classified as over-the-counter medications, and their use is still considered safe when adhering to appropriate nonprescription guidelines, including correct dosage and the absence of contraindications and drug interactions. 7 However, evidence from previous studies has revealed that approximately one-third of the cases taking over-the-counter NSAIDs have contraindications, drug interactions, or overdosage.8,9
Previous studies have highlighted gaps in knowledge, attitude and practice regarding the use of NSAIDs and corticosteroids among patients with chronic rheumatic diseases,10-13 as well as general population.14-20 In Vietnam, there is ample evidence indicating the widespread availability and accessibility of corticosteroids and NSAIDs, along with a high rate of nonprescription sales for these drug groups.21-25 However, there has been no study conducted to assess the knowledge, attitude, and practice regarding the use of these 2 medication groups within the Vietnamese population. As a widely prescribed and rapidly effective medication group, coupled with a lack of understanding regarding their adverse effects, inappropriate use and medication abuse are highly possible. Therefore, we conducted this study with the expectation to identify gaps in knowledge, attitude and practice regarding the use of corticosteroids and NSAIDs in Vietnamese population, thereby providing a basis for appropriate interventions to enhance the quality of patient care.
Methods
Study design
A cross-sectional study was conducted from October 2023 to January 2024 at the Center of Rheumatology, Bach Mai Hospital and Rheumatology Department, Hong Ngoc General Hospital in patients with chronic rheumatic disease.
Bach Mai Hospital’s Rheumatology Center, recognized as the leading referral facility for rheumatology conditions in Vietnam, treated approximately 2000 to 3000 patients each month, providing a large and diverse sample for our research. The frequent use of NSAIDs and corticosteroids among this patient population made it an appropriate setting for the study. 26 In contrast, Hong Ngoc General Hospital, a reputable private facility known for its high standards of care, saw a lower volume of patients, with about 500 to 600 rheumatology cases treated each month. This hospital addressed a wide range of rheumatology conditions and served a patient demographic with higher socioeconomic status, characterized by better education, income, and living standards, as well as less reliance on medical insurance coverage compared to the general population. As a result, the knowledge and attitudes toward medication use, including NSAIDs and corticosteroids, were expected to differ from those in the general population. 27 This diversity contributed to a richer data set and strengthened the overall findings of the study.
Patient eligibility
Eligible participants were individuals diagnosed with a rheumatological condition at least 6 months prior to study inclusion. Patients with cognitive disorders, mental illnesses, and those requiring prolonged corticosteroid use due to specific medical conditions such as primary adrenal insufficiency or surgically treated pituitary tumors were excluded from the study.
Data collection tool and approach
The questionnaire was developed following a formal protocol. The items were first collected from the questions in the literature review. The principal investigator is an expert herself in rheumatology, and she added items that are relevant to the Vietnamese context and then discussed the content of the questionnaire with another medical doctor. The items were also reviewed by an epidemiologist who has experience in scale development before we narrowed down the list of items in the finalized questionnaire. The questionnaire was piloted in 10 patients to confirm their understanding and refine any items that require rephrasing.
The questionnaire included general patient information such as demographic and socioeconomic information, comorbidities, and characteristics of their current chronic rheumatic disease. We also measured patients’ health literacy level using the Single Item Literacy Screener (SILS). It has only 1 question: “How often do you need to have someone help you when you read instructions, pamphlets, or other written material from your doctor or pharmacy?”, with response options range from “0—never” to “4—always.” Similar to previous studies, the response was dichotomized as followed: respondents with scores of 0-1 were deemed to have adequate functional health literacy scores, while those who responded with 2 to 4 were deemed to have inadequate functional health literacy scores.20,28 The validated scale SILS was reported with good reliability in various settings.28-30
This study focused on evaluating patients’ knowledge, attitudes, and practices regarding the use of NSAIDs and corticosteroids. The questionnaire had been developed and designed by the research team based on the fundamental characteristics of NSAIDs and corticosteroids, and references from the content of previous surveys regarding knowledge, attitudes, and practices among patients with chronic rheumatic disease and general population.10-20
The knowledge section began with a question asking patients whether they had heard of NSAIDs and corticosteroids before. If they had, patients were then asked about the sources of information they had heard about these medications from. Following this were 3 questions regarding NSAIDs and 3 questions regarding corticosteroids, including brief questions asking patients to list the drug names, main effects, and potential side effects. In addition, there were 5 knowledge statements assessing dosage, usage, and drug combinations. The 13 statements in the attitude section were divided into 3 main themes: trust in the benefits of medication; concerns about medication side effects; and attitudes toward receiving information. We also provided 5 statements to assess barriers in receiving information and proper practicing regarding medication use. For each statement in the knowledge, attitude and barrier sections, patients select a response on a 5-point Likert scale ranging from 0—Strongly disagree to 4—Strongly agree. The practice section includes 7 scenarios assessing patient’s practice regarding medication use, for each statement, patients select a response on a 5-point Likert scale ranging from 0—Never to 4—Always.
Data collection
Patients visiting the study sites who met the inclusion and exclusion criteria were informed about the study and invited to participate. Patients provided informed consent before being formally interviewed for data collection. Through direct interviews based on a predesigned questionnaire, we collected demographic information; details related to chronic rheumatologic conditions; and assessed knowledge, attitudes, and practices related to NSAIDs and corticosteroids.
To assure the data reliability in our study, all investigators received formal training on data collection, including history taking, examination, and interview techniques. The principal investigator conducted careful monitoring for the first few patients recruited by each investigator. Data entered in the electronic database was verified again by a data analyst for any inconsistency.
Statistical analysis
Continuous variables were presented as mean values (standard deviations) or median (interquartile range). Categorical variables were presented as values and percentages and visualized using horizontal stacked bar charts (for attitudes, barriers, and practices). Poisson regression models were employed to determine factors associated with the primary outcome variables (total number of correct knowledge answers, total number of positive attitudes, and total number of appropriate practices). Independent variables considered for inclusion in the regression models included demographic/socioeconomic characteristics (age, gender, health insurance coverage, education level) and clinical characteristics (duration of illness, use of corticosteroids/NSAIDs and health literacy). In addition, knowledge, attitudes, and barriers were also included in regression models based on the theoretical assumption framework: Before specific patient-targeted information on a health-related issue modifies patient outcome, it first affects the patient’s knowledge, then the patient’s attitude, and eventually the patient’s behavior and practice. A P-value of .05 was considered statistically significant. R language version 4.3.2 was used for all analyses.
We have followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) Guidelines when conducting this study and preparing the manuscript. 31
Result
A total of 182 participants were included in this study, of which 36% were male and median age was 55 (IQR 43–65). Most participants were inpatients (62%), resided at rural area (62%), were married (86%), had medical insurance (74%), and had normal body mass index (BMI) (58%). Around half of the participants had completed high school or higher education, with an average monthly income exceeding 4 million Vietnam Dong (VND) (Table 1). Hypertension was the most prevalent comorbidity (27%), followed by gastroesophageal reflux disease (GERD) (22%), dyslipidemia (12%), and diabetes (11%). Osteoarthritis was the major rheumatological condition (25%), followed by rheumatoid arthritis (17%) and gout (14%). Approximately half of the participants reported a rheumatic disease duration exceeding 5 years. More than half of the participants reported NSAIDs and corticosteroids use, with a median medication using duration of 12 and 24 months, respectively. Among NSAIDs users, nearly half were unaware of the specific medication they had used, compared with only 17% of corticosteroid users. Gastric ulcer was the most commonly reported ADR among users of both NSAIDs (39%) and corticosteroids. Hospitalization due to ADRs occurred in 2.6% of NSAID users and 4.5% of corticosteroid users. Around half of the participants demonstrated sufficient health literacy (Table 1).
General and clinical characteristics.

Abbreviations: AE, adverse effect; BMI, Body mass index; GERD, gastroesophageal reflux disease; GI, gastrointestinal tract; IQR, interquartile range; NSAID, nonsteroidal anti-inflammatory drugs; SLE, systemic lupus erythematosus; VND, Vietnam Dong.
A majority of the participants had never heard of corticosteroids (34%) and NSAIDs (54%) before. Among those informed, doctor was the source of information regarding corticosteroids and NSAIDs in 83% and 84% of the cases, respectively. Medrol (Methylprednisolone) was the most frequently reported brand name among participants, while approximately half of them indicating no familiarity with any NSAIDs’ brand names. The majority of patients were aware of the anti-inflammatory and pain reduction effects of NSAIDs and corticosteroids; however, only 3.3% knew about the immunosuppressive effects of corticosteroids. Regarding corticosteroids, gastric ulcer was the most commonly recognized ADR (64%), followed by Cushing syndrome (30%), osteoporosis (21%), edema (16%), adrenal insufficiency (12%), cataract (6.6%), and gastrointestinal bleeding (2.5%). Regarding NSAIDs, gastric ulcer was the only ADR recognized by patients (95%); other ADRs such as hepatotoxicity, nephrotoxicity, and ADRs related to the cardiovascular system including hypertension, heart failure, or myocardial infarction were not recognized. Nearly 38% of patients disagreed with the recommendation against abrupt discontinuation of corticosteroid after long-term use (Table 2).
Knowledge regarding NSAIDs and corticosteroids among participants.

Abbreviations: ADR, adverse drug reaction; GI, gastrointestinal tract; NSAID, nonsteroidal anti-inflammatory drugs.
Most patients expressed positive attitudes toward the benefits of medication and information provision. Approximately 80% to 90% of patients were concerned about medication’s side effects and apprehensive about drug dependence (Figure 1). “Healthcare providers often lack time to provide information about these medications to patients” was the primary barrier, with a 40% agreement (Figure 2). The majority of patients reported that they frequently adhered to correct practices regarding medication adherence and consult a doctor when abnormalities occur. Meanwhile, very few patients reported engaging in incorrect practices, including self-dosing, self-medicating without prescription, and combining medications without consulting a doctor (Figure 3).

Attitudes toward NSAIDs and corticosteroids use and information receiving.

Information receiving barriers.

Practice of medication use.
Patients with prior use of NSAIDs and corticosteroids demonstrated better knowledge. No other association between knowledge, attitude, barriers and practice was observed in this study (Table 3).
Factors associated with knowledge, attitudes and practice regarding the use of corticosteroids and NSAIDs.
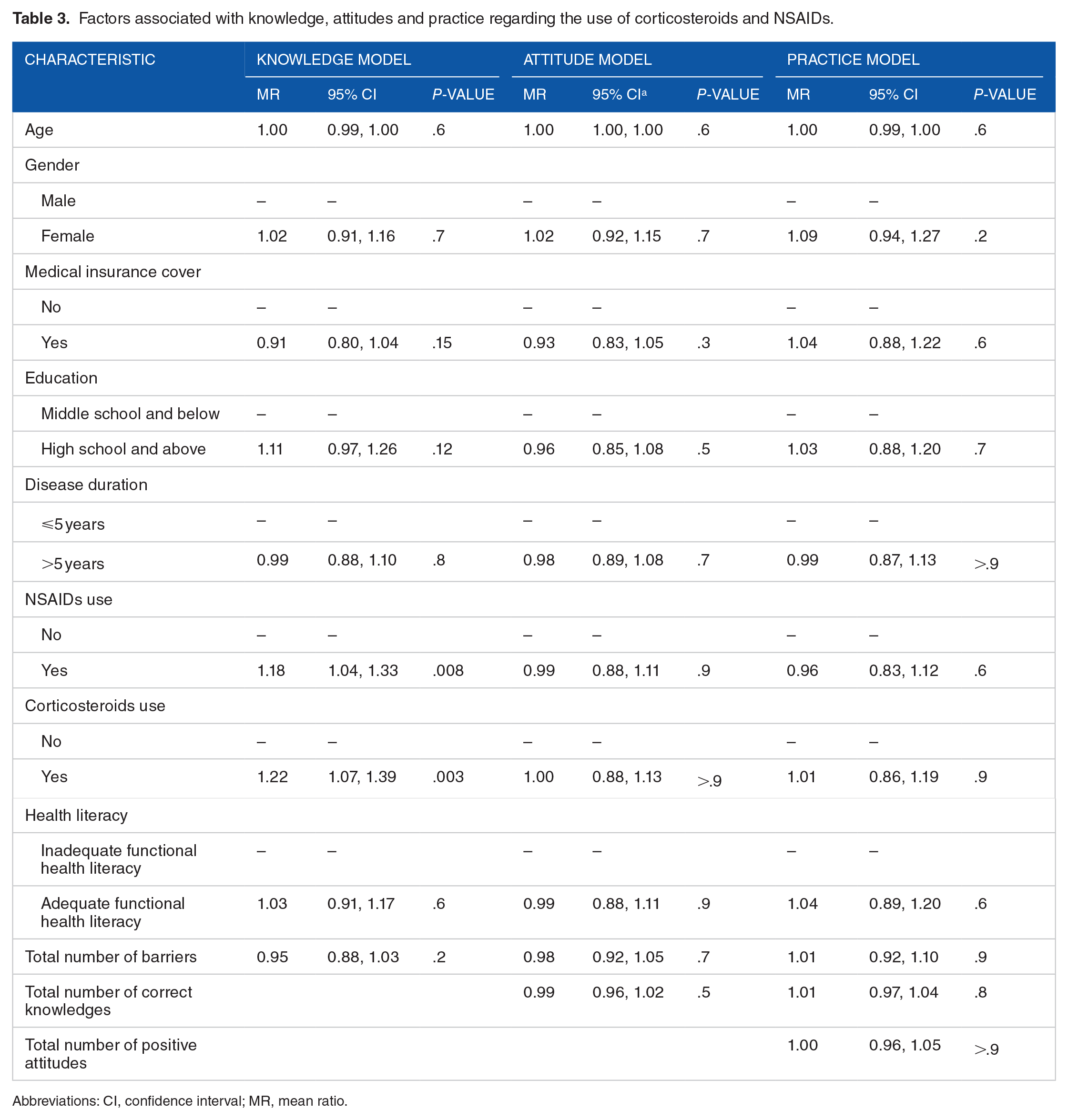
Abbreviations: CI, confidence interval; MR, mean ratio.
Discussion
Our study findings highlighted notable gaps in patient knowledge regarding the adverse effects of NSAIDs and corticosteroids. The majority of patients in the study were only aware of gastric ulceration as an adverse effect of these medications. Conversely, very few patients were knowledgeable about life-threatening adverse effects, including gastrointestinal bleeding, adrenal insufficiency, and toxicity to the liver, kidneys, and cardiovascular system. Similar knowledge gaps have been reported in previous studies among NSAIDs and corticosteroids users.10,13,15,19,20 It is important to note that while severe adverse effects occur relatively infrequently with both NSAIDs and corticosteroids, in populations with high-risk characteristics such as those in our study—including multiple comorbidities and especially the prolonged use of corticosteroids/NSAIDs—these severe ADRs are more likely to occur and pose a life-threatening risk or significantly impair the patient’s quality of life.32,33 Therefore, health care providers may need to prioritize patient education and communication regarding the potential adverse effects of NSAIDs and corticosteroids, particularly among high-risk patient populations. This could involve providing written materials or resources and engaging in proactive discussions with patients about the risks and benefits of these medications. These considerations are important for enhancing patient safety and optimizing the quality of care provided to patients with rheumatological conditions.
Regarding attitudes toward corticosteroids and NSAIDs, our findings indicated the fear regarding the medications’ adverse effects and dependency on them. This could have acted as a barrier to patient treatment adherence. In a 2019 survey of 200 orthopedic patients in Saudi Arabia, over half of the respondents agreed that awareness of NSAIDs’ adverse effects could induce anxiety and lead them to discontinue medication use. 18 Another study in 2008 involving 170 patients with chronic rheumatic diseases found that 56% reported frequent anxiety about NSAIDs’ side effects, and 25% hesitated to take the medication due to these concerns. 11 In another study conducted on 2054 individuals from the general population during the COVID-19 pandemic, corticophobia levels were notably high across various aspects, including corticosteroid-related side effects, changes in dosage forms, or the use of corticosteroids as a drug of choice. 34 To address these concerns and improve patient adherence to treatment, health care providers should prioritize patient education and communication. This includes discussing potential side effects of medications, addressing patient fears and anxieties, and providing clear and comprehensive information about the benefits and risks of treatment options.
Furthermore, our study findings emphasized the role of physicians in providing information, as they were the primary source of information for both corticosteroid and NSAIDs users. However, the major barrier to accessing information in this study arose from physicians not having enough time to provide comprehensive information to patients. Evidence regarding barriers of communication between physicians and patients has been reported in previous studies. In a 2019 qualitative study conducted on 18 type 2 diabetes mellitus patients in Sydney, Australia, the findings revealed that the primary barrier to diabetes self-management was inadequate and inconsistent information received from health care providers. 35 In another study evaluating the care processes of primary care physicians on a simulated model of the United States disease burden in 2017-2018, involving 2500 simulated patients, the findings showed that an average physician would need to work up to 26.7 hours per day to provide standard care for patients, which included comprehensive discussions with patients about the risks and benefits of the medications they use. 36 The lack of connection between physicians and patients, especially in discussing the benefits and risks of medications, is presumed to be even more pronounced in Vietnam, due to the ongoing challenges related to health care workforce shortages and the uneven distribution of health care personnel.21,37,38 This could potentially lead to negative consequences in patient management, as incomplete communication may result in inadequate and inconsistent information being conveyed from the physician, leading to confusion and mistrust. When not fully explained and transparent, patients may resort to seeking information from unreliable sources and are more likely to self-manage their condition according to their own interpretation. This could result in improper practices and significantly impact the quality of treatment. Due to the ongoing issue of health care workforce shortages and the immediate inability to alleviate the burden on physicians, alternative measures to diversify the delivery of accurate information to patients should be considered.
Our study findings did not reveal any gaps in practice, nor did they show any correlation between patients’ knowledge and attitudes to the practice regarding the use of corticosteroids and NSAIDs. This was inconsistent with previous evidence indicating a relatively high rate of nonprescription drug purchasing and the abuse of nonopioid analgesics in Vietnam.21-24 In addition, it did not align with theoretical frameworks assuming a correlation between knowledge, attitudes, and patient practices. The main reason for this discrepancy likely lies in the fact that the practices in our study were self-reported by patients. This resulted in a knowledge-practice gap, masking the actual practice gaps and skewing the relationship between knowledge, attitudes, and practices. This was the major limitation of this study, and this emphasizes the necessity for future study using structured interviews to encompass dosing frequency, adherence to instructions, and any deviations from prescribed usage, thus ensuring an accurate measurement of patients’ practice levels. Beside, since the participants were not randomly sampled, there may be threats to generalizability, particularly if individuals with severe rheumatologic conditions or those with poor knowledge, attitudes, and practices might decline to participate. However, the findings of this study are already very concerning, and our key messages are unlikely to change. Finally, power calculation was not performed. The sample size was what we reached after screening and recruiting all eligible patients during the study period.
Conclusions
Our study findings have highlighted gaps in knowledge, attitudes, and barriers to information access regarding NSAIDs and corticosteroids. It is noteworthy that the study population was expected to have better awareness of these medications due to their prolonged disease duration and a large proportion having used the medications for a long time. This suggests that the actual gaps in knowledge, attitudes, and practices among the corticosteroid and NSAIDs users may be even wider than reported in this study. The findings suggest several policy implications, including increased communication time between physicians and patients, diversification of reliable information sources for patients, and focusing information resources on ADRs. It is recommended that future studies use structured interviews to cover dosing frequency, adherence to instructions, and any deviations from prescribed usage. This approach ensures a precise measurement of patients’ practice levels.
Footnotes
Acknowledgements
Not applicable.