
Abstract
Idiopathic granulomatous mastitis (IGM) is an inflammatory-mediated rare disease that can be linked to rare manifestations. Erythema nodosum (EN) and polyarthritis, seen in a multitude of autoinflammatory and autoimmune diseases, have been rarely linked to IGM. Despite the cause of IGM being unclear, Corynebacterium infections are thought to play a role in the pathophysiology of IGM. Unusually, IGM has a relapsing and remitting course, which also applies to its systemic manifestations. As such, we present a case of IGM in a middle-aged lady who was initially thought to have Corynebacterium-containing unilateral abscesses for which drainage was performed. However, several abscesses devoid of bacterial growth started recurring, and the disease course was complicated by EN and polyarthritis. IGM, EN, and polyarthritis eventually resolved and were managed with symptomatic treatment.
Introduction
Idiopathic granulomatous mastitis (IGM) is a rare benign inflammatory disease of the breast that can mimic other breast pathologies. 1 Despite that the cause of IGM is not well understood, multiple risk factors were described, most importantly including recent pregnancy and/or breastfeeding. 2
The presentation consists of unilateral or bilateral tender firm breast masses accompanied by erythema, pain, and drainage. 3 The diagnosis is ideally performed by breast biopsy (ideally by core biopsy) showing a noncaseating granuloma with epithelioid histiocytes and multinucleated giant cells within breast lobules, and might contain micro abscesses. 2
Certain diseases have been associated with IGM, such as tuberculosis or sarcoidosis, and less rarely ANCA-associated vasculitis. 4 Certain manifestations, that are linked with rheumatological conditions, have been described in the context of IGM. Erythema nodosum (EN) and polyarthritis are examples of such manifestations. We present a case of a middle aged woman who had relapsing and remitting unilateral breast abscesses to be diagnosed with IGM followed by appearance of EN and polyarthritis, both of which self-resolved with resolution of mastitis lesions.
Case Presentation
A 41-year-old G5 P5 previously healthy female presented with vague pain, discharge, and erythema in her right breast. The patient’s last lactation occurred approximately 3 years before her current presentation. Despite attempting self-medication with metronidazole, the symptoms recurred after discontinuing the antibiotic.
Mammography and breast ultrasound revealed a 7-cm nodular and irregular area involving the right breast at 8 o’clock (Figure 1A and B). In addition, there was a suspicious right axillary lymph node 21 mm (Figure 1 C and D). However, no abnormalities were detected in the left breast. Biopsy of the breast mass showed widespread acute inflammation, abscess formation, and fat necrosis (Figure 2).
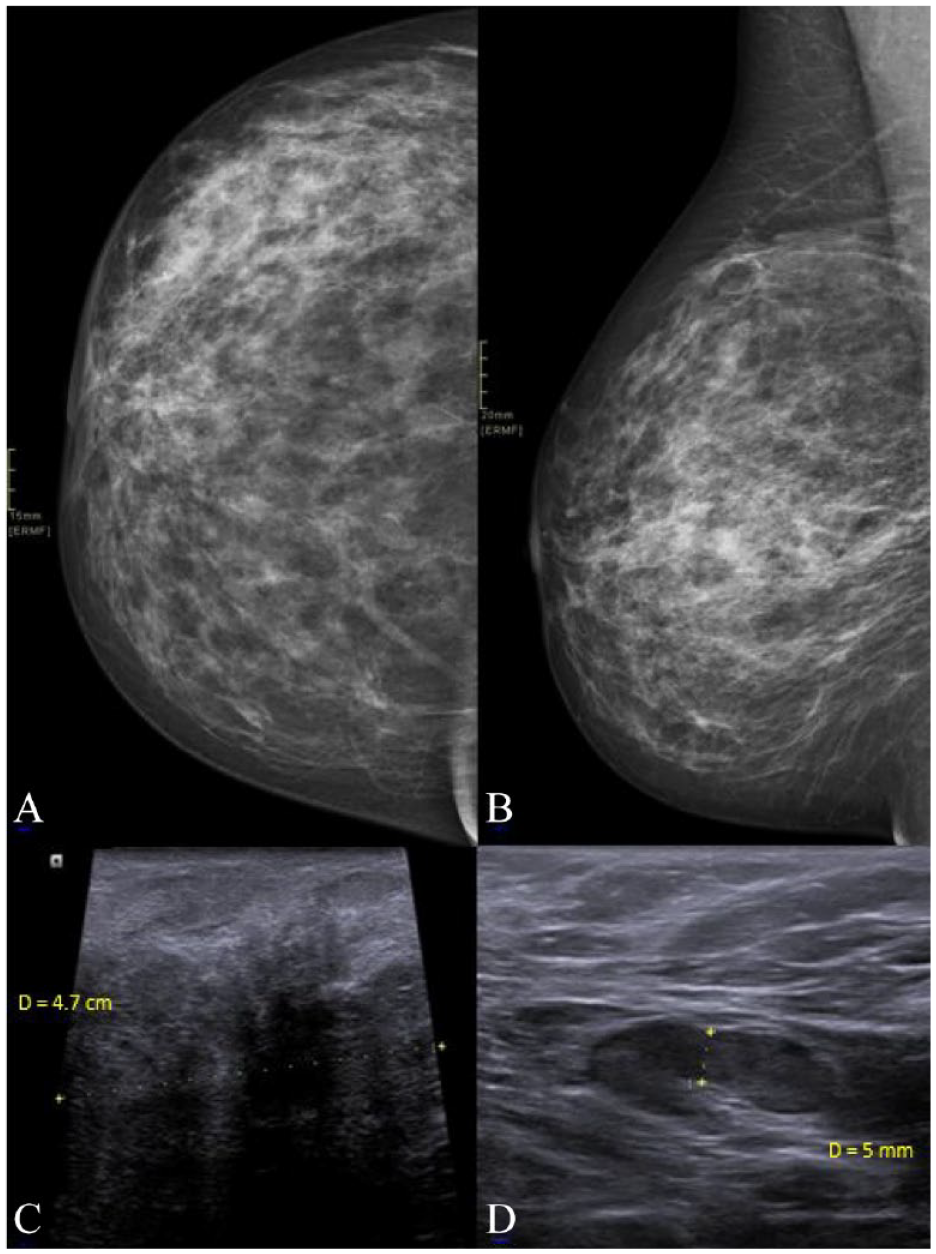
Craniocaudal (A) and mediolateral oblique views (B) of the right breast show an area of increased density along the outer slightly lower quadrant of the right breast. Ultrasound (C) of this region showed an area of decreased echogenicity with areas of low-level internal echoes. Aspiration of the areas with low-level internal echoes revealed pus, which was sent for cytology and culture. Ultrasound of the right axillary region (D) showed a borderline 2 × 1 cm lymph node with 5 mm cortical thickening.
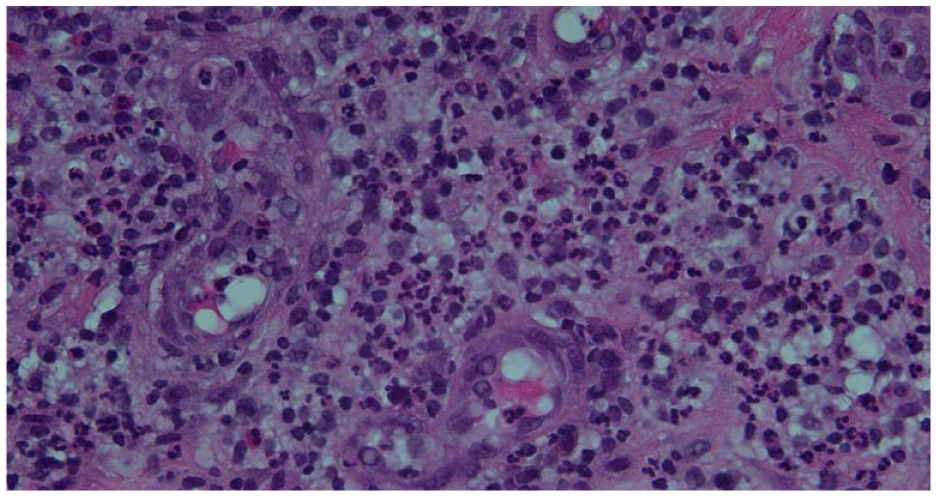
Acute inflammation consisting of neutrophils with prominent vessels. Scattered eosinophils and lymphocytes are also seen. (Hematoxylin and Eosin stain, original magnification 40×).
As there was no clinical improvement with pharmacological therapy, mastotomy with exploration and abscess drainage was performed, and tissue culture revealed the growth of pan susceptible Corynebacterium species. Amoxicillin-clavulanic acid was administered for a 7-day course.
For approximately 1 year after the operation, the patient experienced no symptoms. However, she later developed similar symptoms in the same breast, with new areas being involved on clinical examination. Incision and drainage were performed, but no growth of bacteria was observed.
A few months later, new abscesses began to appear at distinct intervals, all of which resolved completely with short courses of non-steroidal anti-inflammatory drugs (NSAIDs). The patient experienced relief from severe pain when the abscesses self-drained. Notably, the appearance of abscesses was accompanied by flares of fever, myalgias, and polyarthritis, involving the right ankle, hands, and feet, and erythematous and tender bumps were noticed symmetrically on the shins (Figure 3), diagnosed as erythema nodosum. However, the polyarthritis and erythema nodosum resolved with the resolution of abscesses.

Raised erythematous spots on the anterior shins bilaterally.
Discussion
Idiopathic granulomatous mastitis (IGM) is a benign rare condition which involves women of childbearing age. 5 The true prevalence of IGM is unknown. The course of the disease is characterized by a chronic relapsing and remitting inflammation, resulting in scarring and discharging sinuses. 6 Multiple causes were suggested for IGM, although the disease pathophysiology remains unclear. Examples of causes include autoimmune diseases, hormone irregularities, and local immune response to trauma. 1 Nevertheless, sarcoidosis, tuberculosis, foreign substances and bacterial infections are considered to be causes. 1 Specifically, Corynebacterium has been described as a significant contributor to the development of IGM and a cause for IGM recurrence. 7
Polyarthritis has been reported as a rare complication of IGM. Polyarthritis can occur alone or might be associated with other complications such as erythema nodosum (EN). 8 Corynebacterium has been rarely linked to erythema nodosum. 9 Interestingly, this association has happened in the context of IGM. Furthermore, Corynebacterium has been linked to arthritis, specifically septic arthritis. 10
Table 1 lists literature cases that linked IGM with EN and polyarthritis. Interestingly, most cases were treated with corticosteroids. Only 2 previous cases’ manifestations resolved spontaneously 26 similar to our case, and only 1 case where IGM, polyarthritis, and EN coexist in the setting of a Corynebacterium infection. 25
Previous literature cases linking idiopathic granulomatous mastitis to erythema nodosum and polyarthritis.
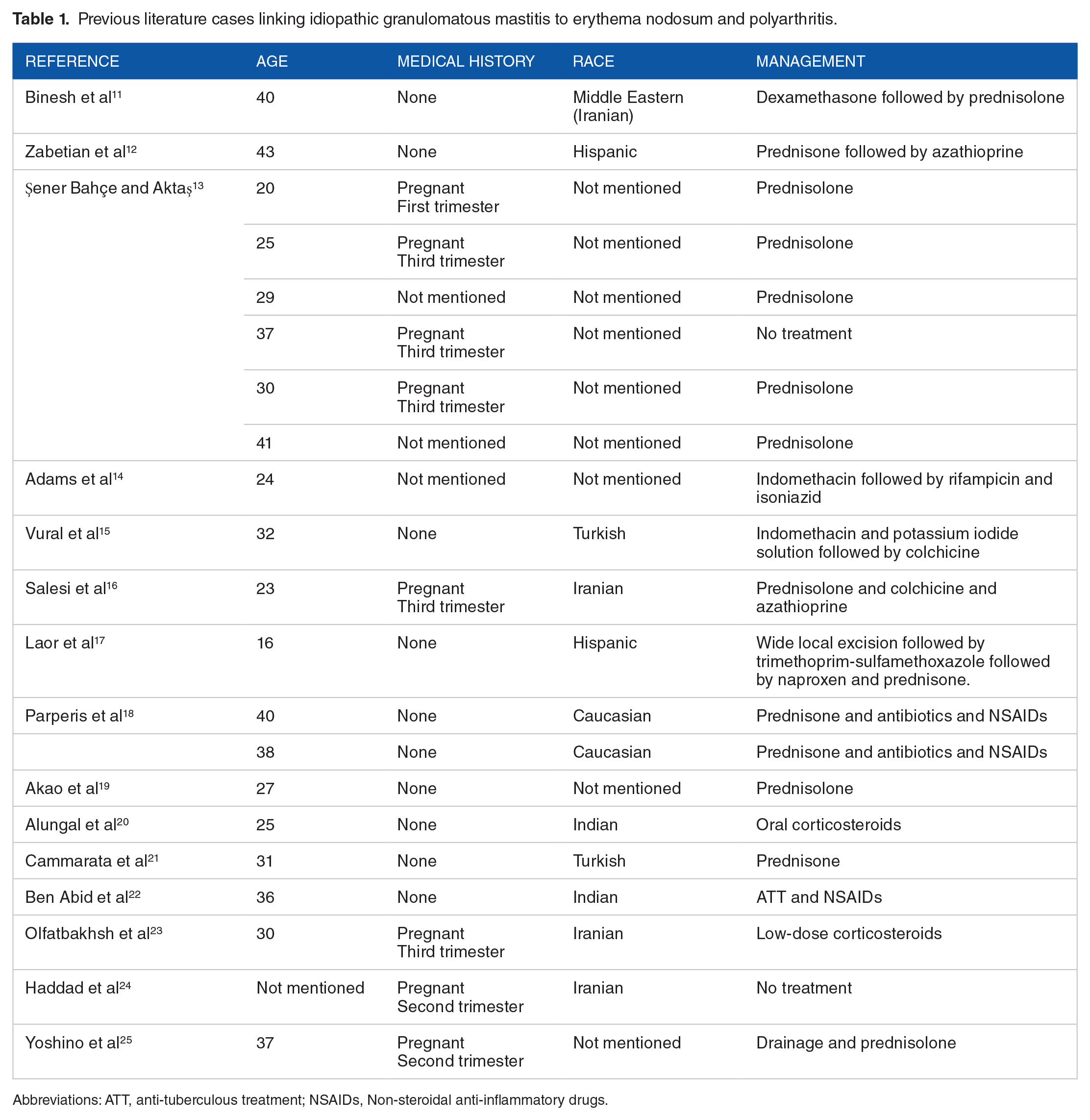
Abbreviations: ATT, anti-tuberculous treatment; NSAIDs, Non-steroidal anti-inflammatory drugs.
Conclusion
Idiopathic granulomatous mastitis can be preceded by a Corynebacterium breast abscess resulting in relapsing and remitting unilateral breast involvement. Erythema nodosum and polyarthritis are 2 complications that can follow the same disease course of IGM. Although glucocorticoids and methotrexate have been described in the literature, our experience shows that conservative and symptomatic management can be sufficient for resolution of symptoms, although a close follow-up is needed to assess for recurrence. The choice of therapy depends on the frequency, duration, and severity of the episodes, response to symptomatic management, and the symptoms overall effect on patients’ quality of life.
Footnotes
Acknowledgements
The authors acknowledge the help of all colleagues at the American University of Beirut Medical Center.
Ethics approval
Ethical permission was not required since this is a case report.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Competing interests
The authors declare that there is no conflict of interest.
Availability of data and materials
None.