
Abstract
Idiopathic granulomatous mastitis (IGM) is a rare, benign inflammatory disorder of the breast. Clinical features may include painful breasts, erythema, subcutaneous nodules, and ulcerative lesions. It can mimic various other breast pathologies, and it is a diagnosis of exclusion after infection, malignancy, and other inflammatory conditions have been ruled out. In this article, we present a case of IGM developing in a 40-year-old female 3 months after hospitalization for myxedema coma. A contrast-enhanced magnetic resonance imaging of the breasts showed bilateral edema, and a biopsy was negative for malignancy or infection. She was started on prednisone and had noticeable improvement of ulcerations within several weeks. IGM is a rare condition that requires a multimodal treatment approach. Often recalcitrant disease is encountered and requires surgical intervention, immunosuppression, and antimicrobial therapy. The diagnosis should be entertained in patients with bilateral breast inflammation to avoid unnecessary surgical resection early on.
Introduction
Idiopathic granulomatous mastitis (IGM) is a rare, benign inflammatory condition affecting breast tissue. It is typically characterized by marked inflammation with erythematous skin changes and pain and may progress to include skin ulcerations and superimposed infections. Chronic inflammatory changes and scarring may also be seen. The disease is often confused with more common conditions such as bacterial abscesses and malignancies, and as such, successful diagnosis relies on a high index of suspicion and clinical gestalt.1,2 Oftentimes patients receive multiple courses of antibiotics, biopsies, and unnecessary surgical procedures due to the challenge in diagnosis. Clinical features, inflammatory markers, negative wound cultures, and tissue analysis are used together to make the diagnosis. The disease is often seen in women of child-bearing age and a higher incidence has been seen among Hispanic women. 2 The pathogenesis of IGM remains unclear, although there is increasing evidence in support of an autoimmune mechanism that has been attributed to environmental triggers, infection, and trauma.3,4 High prolactin levels have also been associated with the disease.4-6 The diagnosis is challenging due to lack of pathognomonic features on clinical examination and imaging studies. The gold standard for diagnosis is histopathologic examination from a core needle biopsy (CNB) demonstrating noncaseating granulomas that have a sensitivity exceeding 90%.7,8
In this article, we present a unique case of IGM occurring 3 months after hospitalization for myxedema coma in a patient with a history of papillary thyroid carcinoma and iatrogenic hypothyroidism. We highlight diagnostic and treatment challenges that are often encountered in this condition.
Case Presentation
A 40-year-old primiparous female presented to a primary care clinic to establish care with a chief complaint of bilateral breast ulcers. Her symptoms started 2 months previously, as bilateral breast pain and progressive peri-areolar erythema extending laterally. At the time she was evaluated with a bilateral breast ultrasound in an emergency department, which was negative for abscess or fluid collections. She was given a 5-day course of cephalexin for presumed mastitis and provided a referral for follow-up with a breast surgeon. She was referred back to the hospital by surgery 1 week later due to persistent symptoms at which time she was started on intravenous vancomycin and was discharged 2 days later on a 14-day course of oral linezolid. Her symptoms continued to progress and included severe breast pain, bilateral subcutaneous lumps, and interval development of bilateral ulcerations, which resulted in a second hospitalization 6 weeks later. At the time, laboratory studies showed mild anemia, elevated erythrocyte sedimentation rate, and markedly elevated thyroid stimulating hormone at 74.90 µIU/mL. The left breast ulcer was selected for CNB as this lesion was open at the time. Pathology revealed dense fibrotic breast tissue with no features of malignancy (Figure 1). A breast magnetic resonance imaging showed bilateral inflammatory changes and band-like focal edema at the 12 o’clock position of the right breast (Figure 2). Wound cultures returned negative. The patient was monitored off antibiotics and treated with local wound care and pain control. Her levothyroxine dose was adjusted, and she was discharged with follow-up arranged for surgery and primary care. The patient established in the outpatient internal medicine clinic 2 weeks after discharge resulting in the current evaluation.

Hematoxylin and eosin–stained breast specimen showing normal-appearing tissue with predominant fibrous interlobular stroma and a paucity of adipose tissue (A). Higher magnification showing several acini and ductules with intralobular connective tissue within the breast lobule (B).

Caudocranial view of contrast-enhanced magnetic resonance imaging of breasts with T2-weighted sequences showing edema of skin, subcutaneous, and glandular tissue markedly pronounced right breast greater than left.
Her past medical history was significant for papillary thyroid carcinoma status post subtotal thyroidectomy with postoperative radioiodine ablation performed in the United Kingdom 2 years prior to presentation, iatrogenic hypothyroidism, secondary amenorrhea, prior alcohol abuse with cirrhosis, and medical nonadherence. She had a prolonged hospital stay for myxedema coma occurring 3 months prior to the onset of her breast symptoms. She required intensive care unit admission for acute respiratory failure, hypothermia, metabolic acidosis, and acute renal failure. At the time her thyroid stimulating hormone was 136.00 µIU/mL and free T4 0.027 ng/dL. She required intubation and mechanical ventilation due to high metabolic demand and respiratory rate, and she was started on intravenous thyroid hormone replacement. Fortunately, the patient had a full recovery. The patient is adopted and was not aware of her family history. Her medications included levothyroxine 100 µg daily, ibuprofen 400 mg every 8 hours as needed, and lactulose 15 mL twice daily.
In the clinic, she complained of worsening breast pain, progressive lesions that have scabbed over, and scant discharge (Figure 3). She denied any fever, chills, or trauma to the breasts. No nipple inversion or nipple discharge. She also complained of amenorrhea with her last menstrual period 8 months prior to presentation. On physical examination, the patient was afebrile and well-appearing. There was a 5 × 3 cm nonpurulent, peri-areolar ulcerative lesion of the right breast at the 9 o’clock position and a 3 × 3 cm nonpurulent, peri-areolar ulcerative lesion of the left breast at the 4 o’clock position. There was an eschar formation with macerated tissue underneath. No crepitus, erythema, or other surrounding skin changes were appreciated. Incidentally, there were 3 enlarged right posterior cervical lymph nodes found. The rest of the physical examination was unremarkable. Laboratory studies were as shown in Tables 1 and 2.

Pictured is the right breast (top row) and left breast (bottom row) at 2 weeks (A), 4 weeks (B), 6 weeks (C), and 7 weeks (D) after initiation of prednisone. Sloughing of the right eschar can be seen at 7 weeks with fatty, stromal tissue appearing underneath.
Routine Laboratory Panel.

Abbreviations: WBC, white blood cells; Hb, hemoglobin; BUN, blood urea nitrogen; AST, aspartate transaminase; ALT, alanine transaminase; ALP, alkaline phosphatase.
Special Tests.
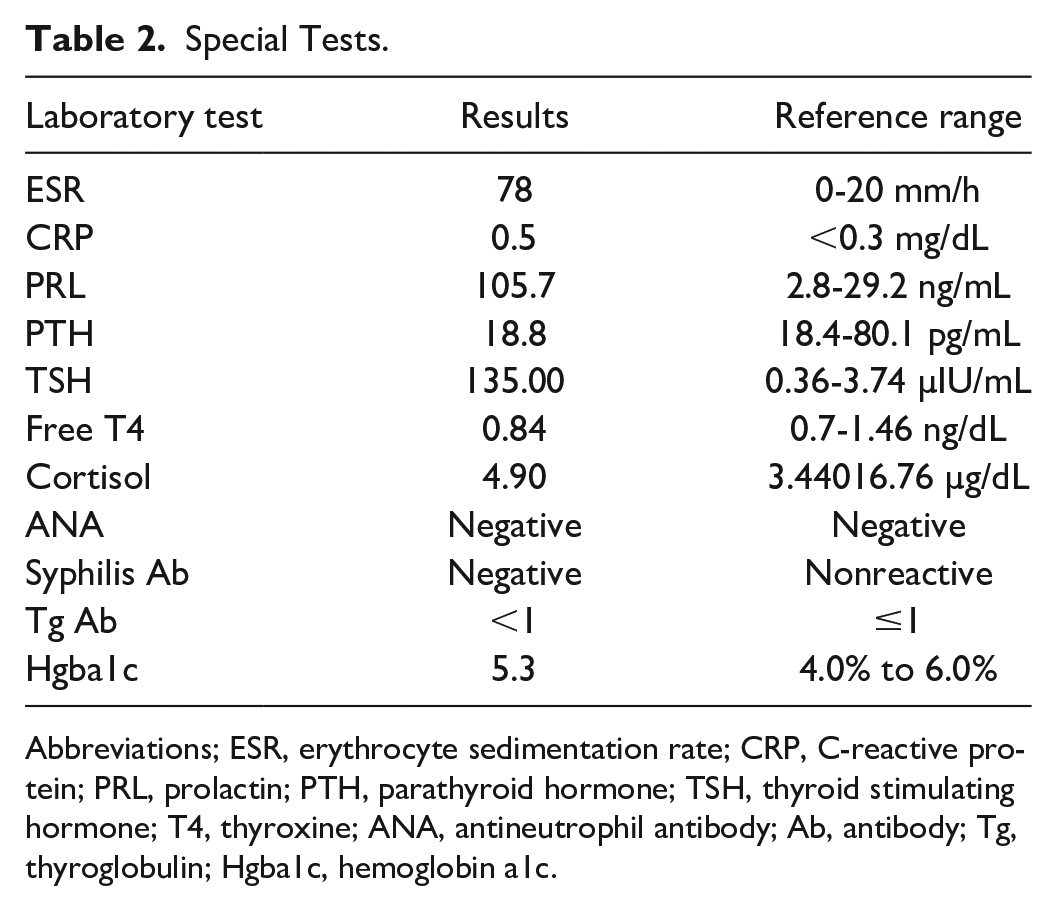
Abbreviations; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; PRL, prolactin; PTH, parathyroid hormone; TSH, thyroid stimulating hormone; T4, thyroxine; ANA, antineutrophil antibody; Ab, antibody; Tg, thyroglobulin; Hgba1c, hemoglobin a1c.
After review of her disease course, bilateral involvement, negative biopsies and cultures, and lack of improvement with empiric antibiotics, she was diagnosed with presumed idiopathic granulomatous mastitis. She was started on a prolonged course of prednisone 20 mg daily in addition to wound care with zinc oxide bandages daily. Pantoprazole 40 mg daily was added for gastrointestinal protection. She was later prescribed a 10-day course of doxycycline due to worsening green-yellow discharge of the right breast and referred to rheumatology for consideration for escalation of immunosuppressive therapy. Her levothyroxine dose was increased, and thyroid function tests and elevated prolactin levels were continuously monitored to normalization (Figures 4 and 5).

Thyroid function tests as a response to adjustments in levothyroxine.

Serum prolactin level as a response to adjustments in levothyroxine.
Discussion
Idiopathic granulomatous mastitis is important to consider in patients with chronic mastitis, and in particular, if there is bilateral involvement. The histopathology from the CNB in this patient showed densely fibrotic breast tissue with microcalcifications. The biopsy was not performed under image-guidance, which may have resulted in a nondiagnostic specimen. Furthermore, magnetic resonance imaging after the biopsy revealed more disease activity in the right breast compared with the left, which may have provided a higher diagnostic yield if this site was selected for biopsy.
Treatment approaches are not well established for IGM. However, immunosuppression by virtue of systemic corticosteroids is considered by many to be the initial treatment of choice. Corticosteroid courses in previous studies were in extended 6- to 12-month courses. Treatment with doxycycline, 100 mg twice daily, was successful also as a first-line therapy, with complete response in 50% of patients in a previously published study. Methotrexate appeared to be a successful second-line therapy in patients with doxycycline-refractory disease (complete response in 50%). 2 Additional immunosuppressant therapies remain under investigation and may offer promising results in the future. 6 Oftentimes multiple surgical debridement procedures are performed and are usually unsuccessful due to disease recurrence. Vanovcanova et al have demonstrated success with use of colchicine, vitamin E, and topical ribwort plantain extract. 9
Successful treatment usually relies on a multimodal approach, which may include immunosuppressive therapies, surgical debridement in refractory cases, antibiotics, and endocrine-directed therapies. 10 There is a paucity of information in terms of therapeutic options and a definitive treatment remains to be established. However, the general census favors avoiding surgical excision as disease often recurs and cosmetic outcomes are often suboptimal and potentially severely disfiguring.11,12 Although systemic corticosteroids are often the initial treatment of choice, response rates are highly variable, and often more effective when initiated early on in the acute stages. 12 This patient was started on prednisone at a dose of 20 mg daily, which is significantly lower than the typical starting dose of prednisone for this condition (0.5 mg/kg/day). She was referred to rheumatology for management of corticosteroids and consideration for escalation of immunosuppressive therapy; however, there was significant delay in referral due to the patient being an impoverished undocumented resident and without medical insurance.
Uncontrolled hypothyroidism with concomitant thyroid releasing hormone–mediated hyperprolactinemia may have placed this patient at risk for the development of this disease. However, a direct cause-and-effect relationship cannot be established. It is also possible hyperprolactinemia may have contributed to the patient’s secondary amenorrhea as well.
In summary, IGM is a rare inflammatory condition that is poorly understood. Treatments are highly variable with varying success rates. This case highlights the challenges of both diagnosis and management of this rare condition. Future studies are necessary to determine optimal treatment strategies for this disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval to report this case was obtained from the Sarasota Memorial Health Care System.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.