
Abstract
BACKGROUND:
IGM has a diagnostic and treatment dilemma. The etiology of IGM is unknown but some conditions have been discussed as predisposing factors including Oral Contraceptive Pills, pregnancy, breast feeding, reproductive age, hyperprolactinemia, infectious and autoimmune diseases. The current study aimed to determine possible risk factors for IGM and to evaluate our experience in its management.
PATIENTS AND METHODS:
The study included forty patients with IGM and forty females with normal breasts as a control group. CST treatment was initiated for all patients; patients who responded completely were followed up without surgical intervention. Failure to respond to medical therapy or incidence of corticosteroid-related complications were considered indications for surgical treatment. All patients were followed up for 6 months to detect recurrence.
RESULTS:
IGM had a significant higher incidence rate in young females within 5 years from the last lactation, smokers, those with hypperprolactinaemia, who had a history of breast feeding and those who received OCP (P = <0.001, <0.001, 0.006, 0.001, 0.023 and 0.027 respectively). The central part of the breast was more affected (9 cases (22.5%)). Multicenteric disease affected 8 cases (20%). Breast Mass was the most common presenting sign. After CST; the mass disappeared in 5 cases (12.5%), mass size reduced in 26 cases (65%) and mass size not affected in 9 cases (22.5%). Surgery was done in whom the mass size was reduced or not affected (35 cases (87.5%)). Disease recurrence was reported in 2 cases (5.7%).
CONCLUSION:
IGM usually affects females in their childbearing period with multiple risk factors mainly parity, smoking, OCP and breast feeding with wide variation regarding the presenting manifestations. We should start with CST as there is always a chance to avoid unnecessary surgery and combination of both modalities can reduce the incidence of recurrence.
Introduction
Idiopathic granulomatous mastitis (IGM) or granulomatous lobular mastitis, is a benign chronic inflammatory breast disease that was first described by Kessler and Wolloch in 1972 [1,2]. It is characterized by sterile noncaseating lobulocentric granulomatous recurrent inflammation [3–5]. IGM has a diagnostic and treatment dilemma as it clinically and mammographically mimics breast cancer especially the inflammatory type and it lacks a definitive treatment plan [6–8]. The etiology of IGM is unknown but some conditions have been discussed as predisposing factors including Oral Contraceptive Pills (OCP), pregnancy, breast feeding, reproductive age, hyperprolactinemia, infectious diseases (such as the Gram-positive bacillus Corynebacteria especially corynebacterium kroppenstedtii) and autoimmune diseases [7–10]. The most common presenting sign is a defined hard lump in the breast [10]. As the disease progresses nipple inversion, peau d’orange, tumorous induration, ulcer and fistula can occur that can easily be mistaken for cancer [6,9,10]. Neither U/S nor mammography can differentiate IGM from malignant or other benign lesions, especially inflammatory breast cancers [8,9]. Some authors suggested magnetic resonance (MRI) in diagnosis of IGM, but studies have shown that MRI does not provide additional findings [8]. In view of the non-definitive clinical and imaging findings; histopathology is the cornerstone of definitive diagnosis by core tissue biopsy; Fine Needle Aspiration Cytology (FNAC) cannot confidently differentiate IGM from other breast lesions whether benign or malignant [9,10]. Before the 1980s; most patients with IGM were treated with wide surgical excision. However, conservative therapy with oral steroids was currently being endorsed as a first-line treatment option before surgical consideration [11]. Multiple case series have reported that treatment of IGM involves one or a combination of several treatment options including treatment-free close follow-up, drainage, excision, antibiotics, steroids, and various immunosuppressive agents [12–16]. Some studies suggested the use of methotrexate with surgery or treatment with corticosteroid and azithromycin, and administration of steroids directly in the lesions [17–21]. The current study aimed to determine possible risk factors for IGM and to evaluate our experience in its management.
Patients and methods
Patient selection
A case-control study included forty female patients with IGM defined as any female patient with histopathological diagnosis of IGM (lack of caseation within the granuloma that is centered on the lobule as proved by core tissue biopsy which is considered pathognomonic for IGM) and forty females who were attending the outpatient clinic either complaining of mastalgia and were proved normal clinically and radiologically or females who attended the outpatient clinic for checkup or having cancer phobia and also proved normal clinically and radiologically as a control group. Cases and controls were females attending the outpatient clinics in the department of surgery, Medical Research Institute, University of Alexandria, Egypt and in the main university hospital, Alexandria Faculty of Medicine, University of Alexandria, Egypt. Patients with specific granulomatous mastitis, patients who had previous malignancy and patients with any contraindications for corticosteroid therapy were excluded from the study.
Ethical considerations
Institutional Research Committee approved the protocol before the study started (Ethics code: E/C. S/N. R4/2019). The study was explained to prospective patients and written informed consent was obtained before study entry.
Study protocol
All included females underwent Complete history taking (Age, marital status, history of oral contraceptive use, smoking, time elapsed since the last lactation, history of breastfeeding, previous breast suppuration, family or past history of breast cancer, IGM or tuberculosis, history of autoimmune diseases and history of previous drainage procedures for similar conditions, Full clinical examination (localization and size of breast lesion, size of the breast, signs of inflammation, the presenting sign (lump of the breast, nipple inversion, peau d’orange, abscess or sinus), laboratory investigations (after confirming diagnosis with core tissue biopsy; routine lab investigations, serum prolactin level, culture and sensitivity test and Ziehl–Neelsen staining for Mycobacterium tuberculosis) and Radiological investigations (U/S mammography both breasts, tuberculosis was excluded in each patient with chest X-ray films). Any collection was drained either by aspiration under U/S guidance or with open drainage. Medical treatment was initiated for all patients diagnosed with IGM with prednisolone. An initial daily dose of 0.5 mg/kg/day was used in two divided doses. In patients who responded completely to corticosteroid therapy within 8 weeks; tapering of prednisolone dose over two weeks was done till complete stoppage and subsequent follow-up was applied without surgical intervention. Failure to respond to Corticosteroid therapy (CST) regarding the decrease in size or incidence of corticosteroid-related complications were considered indications for surgical intervention. During surgery; we excised the inflammatory mass with a rim of normal non affected tissues around, in association with excision of the retro areolar duct system which is thought to be the site of disease origin [9]. The choice of the appropriate surgical technique is dependent on the breast mass ratio [22,23]. Early postoperative complications like bleeding and infection were recorded. All patients were followed up for 6 months in regular visits at the outpatient clinic at intervals of 3 and 6 months to detect recurrence. Recurrence was considered only after histopathological confirmation by core tissue biopsy. Patients with recurrence after excision underwent re-excision and oral prednisone [24,25].
Statistical analysis
Data were fed to the computer and analysed using IBM SPSS software package version 20.0 (Armonk, NY: IBM Corp). Qualitative data were described using number and percentage. Quantitative data were described using range (minimum and maximum), mean, and standard deviation, median and interquartile range (IQR). Chi-square test for categorical variables, to compare between different groups. Fisher’s Exact or Monte Carlo correction for chi-square when more than 20% of the cells have expected count less than 5. Student t-test for normally distributed quantitative variables to compare between two studied groups. F-test (ANOVA) for normally distributed quantitative variables, to compare between more than two groups. Significance of the obtained results was judged at the 5% level.
Results
The study included forty female patients with IGM and forty females with normal breasts as a control group during the period from Mars 2019 to June 2021. As stated in Table 1; IGM had a significant higher incidence rate in young females within 5 years from the last lactation, smokers, those with hyperprolactinaemia, who had a history of breast feeding and those who received OCP (P = <0.001, <0.001, 0.006, 0.001, 0.023 and 0.027 respectively). Regarding presence or absence of autoimmune diseases; there was no significant difference between both groups (P = <0.675). The studied risk factors among cases and controls were presented in Table 1. None among both cases and controls had family history or personal history of IGM, breast cancer or TB. Clinically; twenty two cases (55%) had IGM in the left side while 18 cases (45%) were affected in the right side. The central part of the breast was more affected (9 cases (22.5%)) followed by the upper outer quadrant (8 cases (20%)). Multicentric disease affected 8 cases (20%). Sixteen cases (40%) were presented with mass and acute abscess on top while 12 cases (30%) presented with Mass with sinus. Nine cases (22.5%) presented with mass only and 3 cases (7.5%) presented with mass with nipple retraction. Clinical findings in the studied patients were grouped in Table 2. Regarding the effect of preoperative oral prednisolone on mass size; mass disappeared in 5 cases (12.5%), mass size reduced in 26 cases (65%) and mass size not affected in 9 cases (22.5%). Previous abscess drainage in 6 cases (15%), lump excision in 4 cases (10%) and U/S Guided aspiration in 2 cases (5%) were done. Effect of preoperative Oral prednisolone on mass size and previous interventions were shown in Table 2. Operative techniques were used in cases in whom mass size were reduced or not affected (35 cases (87.5%)). Lateral mammoplasty was used in 9 cases (25.7%), superior pedicle mammoplasty in 8 cases (22.9%), Medial mammoplasty in 5 cases (14.3%), round block excision in 4 cases (11.4%), batwing excision mammoplasty in 6 cases (17.1%) and inferior pedicle mammoplasty in 3 cases (8.6%). Reported postoperative complications were minor wound dehiscence in 16 cases (45.7%), seroma in 3 cases (8.6%), wound infection in 7 cases (20%), disease recurrence in 2 cases (5.7%) and transient NAC ischemia in one case (2.9%). Operative techniques and reported complications were grouped in Table 2. Figure 1 shows one of our studied IGM cases.
The studied risk factors in both cases and controls
The studied risk factors in both cases and controls
Clinical findings, effect of preoperative oral prednisolone on mass size, operative technique and complications
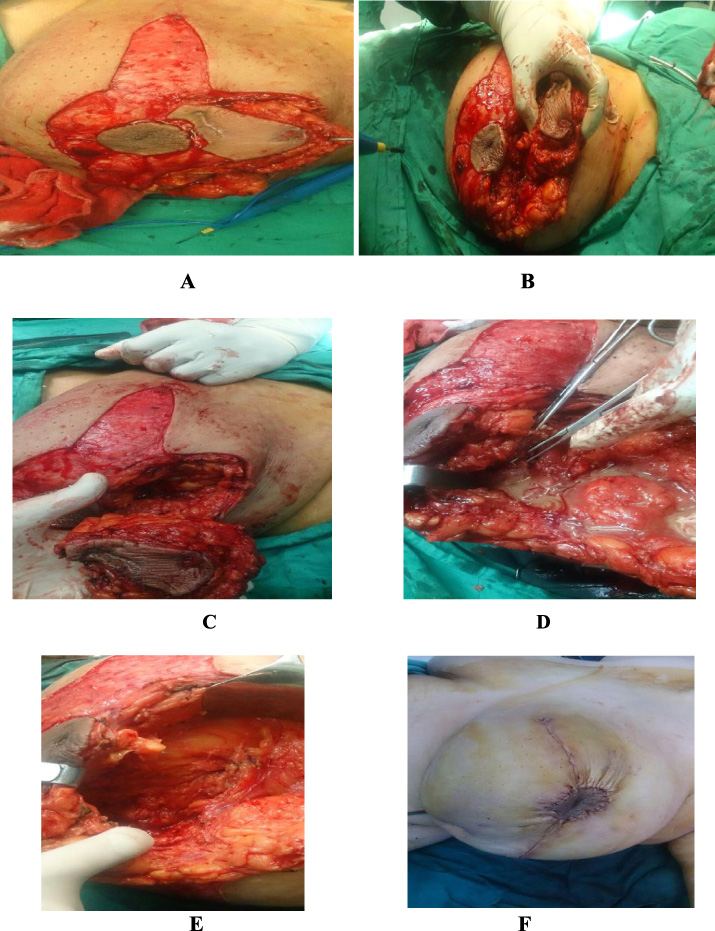
(A–F) 43 years old female patient diagnosed as IGM presented with breast mass and sinus in the upper half of the left breast; wide local excision was done using Batwing excision mammoplasty technique.
As IGM is a disease that involves the breast in an isolated manner, its mechanism of development is believed to involve the following sequence: ductal epithelial damage, transition of luminal secretions to the lobular connective tissue, local inflammation in connective tissue, macrophage and lymphocyte migration to the region, and local granulomatosis inflammatory response [26]. However, the trigger factor in the development of epithelial damage has not been clarified. Autoimmunity, pregnancy, lactation, hyperprolactinemia, oral contraceptive use, local trauma to the breast, rarely observed infectious factors, smoking, and diabetes mellitus are believed to be trigger factors in IGM etiology [27–29]. The current study concluded that IGM had a significant higher incidence rate in young females within 5 years from the last lactation, smokers, those with hyperprolactinemia, who had a history of breast feeding and those who received OCP (P = <0.001, <0.001, 0.006, 0.001, 0.023 and 0.027 respectively). In our work; the mean age among the patients with IGM was significantly younger (35.95 ± 6.58) in comparison to the control group (44.55 ± 8.27) which is similar to the results of many studies [26–29]. Among the forty patients with IGM; 34 patients (85%) were married; all of them except 4 cases had a history of breast feeding and IGM occurred in 70.6% of them within 5 years of the previous lactation. These findings were supported by the findings of Kadivar et al. [30] who concluded that childbirth and breastfeeding are the main risk factors for developing IGM especially within two years of the previous lactation. But the presence of unmarried females and females without a history of breast feeding among the patients indicate the presence of other main risk factors; this finding was the same observed by Pak et al. [31]. This observation supported the multifactorial nature triggering the development of IGM. About two thirds (65.5%) of the cases had OCP with a significant difference between cases and controls. This finding was supported by many studies [26–29] and conflicted with others [28–31]. Parasad et al. [32] conducted a study on 73 patients with IGM, only 2 of them (2.7%) were smokers but in our study; eleven cases (27.5%) were smokers with a significant difference between cases and controls; some studies [29–31] supported this finding and even considered smoking is most significant predisposing factor even in passive smokers. Some studies reported that rheumatoid factor (RF), ANA, and anti-dsDNA antibodies were positive in all patients with IGM without other clinical manifestations suggestive of autoimmune etiology [33,34]. But in our work we depended on presence or absence of a history of autoimmune diseases and concluded no significant difference between cases and controls but we recommend further studies to consider lab investigations to clarify this relation. Clinically; the central part of the breast was more affected (9 cases (22.5%)) and this support the hypothesis accusing the retro areolar duct system as being the site of disease origin [9]. Multicentric disease affected 8 cases (20%). All studied patients presented with a mass with or without inflammatory signs; these finding was similar to the results of Pak et al. [31] who concluded that the breast mass was the most common presenting symptom. In the current study; up to 40% of patients develop symptoms of acute abscess which is near to the findings of Freeman et al. [35] who concluded that around 37% presented with signs of an abscess. There is no definitive therapeutic strategy for IGM; treatment methods include mastectomy, excision, drainage, antibiotic therapy, corticosteroid treatment, and observation [17–21]. Surgical treatment was the mainstream of treatment before 1980, and is still preferred by many experts nowadays [36]. As suggested by Neel et al. [37], the first-line surgical therapy did not reduce the incidence of relapse in a long-term follow-up; 80% of IGM patients relapsed after surgical treatment, and unsightly scars tended to be more frequent among women who had undergone surgery as the first line of treatment [12–15]. In our study; we started with CST therapy as the first line and according to the degree of response; we proceeded to surgery or not. In 1980; some studies [38,39] recommended CST as an effective option for the treatment of IGM. In recent years, low doses of corticosteroid were considered effective for IGM patients however there are some researches showing different results [40–42]. Azlina et al. [43] found that about half of the cases relapsed after discontinuation or decreasing the steroid dose. The proceeded results were validated by Neel et al. [37], whose research implied that corticosteroids were often effective (85%), but relapse was frequent (46%) when the dose was tapered. Zhou et al. [44] performed a meta-analysis to make a comparison between two different therapeutic methods comprising the surgical approach, and a special pharmaceutical regimen, which includes corticosteroids and antibiotics and immunosuppressive therapy without surgical approach and demonstrated that there is no significant difference in the recurrence of IGM between the surgical and conservative approaches, whereas the implementation of numerous surgeries is associated with a higher probability of wound infection, sinus formation, and other cosmetic problems. Hence, the pharmaceutical approach (without surgery) is strongly recommended; nonetheless, surgery could be suggested in case of recurrent patients or lack of pharmaceutical efficacy. Because of this literature debate; we concluded that no single treatment modality is perfect as both commonly used two methods namely surgery and CST have evident recurrence rates if a single modality is used alone. The combination between both modalities is highly recommended as even in patients in whom the lesion did not resolved completely; 65% of cases got benefit from starting with CST in reducing the size of the mass and subsequently in reducing the magnitude of surgery. Antibiotic therapy is not widely analyzed in IGM, but in the case of abscess or sinus formation, empiric antibiotic treatment is recommended due to the high probability of Corynebacterium infection [43]. In our wok; we have prescribed antibiotics empirically (as all cultures were sterile) during the first week of CST to guard against 2ry infection. Because of all of these different views either regarding etiology, risk factors and the best modality of treatment; we recommend further studies with bigger number of studied patients in different centers and wide spectrum of more risk factors and comparative modalities of treatment starting from just observation up to mastectomy as a surgical approach and different types of medications as a medical approach or combined protocols with longer periods of follow up.
Conclusion
IGM is a chronic inflammatory condition affecting women mostly in their childbearing period with multiple risk factors mainly parity, smoking and breast feeding with wide variation regarding the presenting manifestations. Exclusion of other inflammatory and malignant conditions of the breast is mandatory before initiation of therapy. We shouldn’t rush to start with surgical therapy before starting steroids as there is always a chance to avoid unnecessary surgery or decrease the magnitude of surgery in addition to decreasing the recurrence rate.
Footnotes
Conflict of interest
The authors declare no conflict of interest.