
Abstract
Objective:
The present work was led by a multidisciplinary panel of experts and proposes an extensive review on the use of prescription crystalline glucosamine sulfate (pCGS) in the multimodal treatment of osteoarthritis (OA) applicable in Ukraine and other Commonwealth of Independent States (CIS) countries.
Methods:
A panel of rheumatologists, orthopedic surgeons, and field experts from Ukraine and CIS regions discussed the management of OA. Literature was systematically searched using Medline, EMBASE, CIHNAL, and Cochrane Library databases. The 2-day meeting critically reviewed the available literature, treatment algorithms, pharmacoeconomic aspects, and real-world instances to form a multimodal approach based both on real-life clinical practice and systematic literature research for the management of OA in Ukraine and CIS countries.
Expert Opinion:
pCGS plays a pivotal role in the stepwise approach to OA treatment. If it is necessary (step 1), the combined use of pCGS with paracetamol and topical nonsteroidal anti-inflammatory drugs (NSAIDs) has been recommended. If symptoms persist, oral NSAIDs and intra-articular (IA) hyaluronic acid or corticosteroids are added to the therapy (step 2) of pCGS in the patients. In case of insufficient relief and severe OA (step 3), pCGS along with oral NSAIDs, IA corticosteroids, and duloxetine have been recommended. Patient stratification with regular monitoring and careful alterations in treatment were advocated.
Conclusions:
This expert opinion article recommends a modified approach to the existing guidelines incorporating pCGS in treatment modality of OA in Ukraine and CIS countries. Extensive use of pCGS targets early symptomatic relief in OA while limiting the adverse effects due to long-term use of analgesics and NSAIDs.
Keywords
Introduction
Osteoarthritis (OA) is a progressive and chronic inflammatory joint disease that causes pain, disability, impaired quality of life (QoL), functional limitations, and increased health care burden. 1 While OA accounts for major disability in the older population, knee OA is becoming an important health care challenge accounting for 80% of total OA burden. 2 According to the Global Burden of Disease Study 2016, OA is highly prevalent affecting approximately 300 million worldwide. 3 The impact of OA on health and work productivity across the five major European countries were substantial and similar despite variations in pharmacotherapy in different countries, most likely driven by national prescribing guidelines. 4
The current goals for OA treatment are aimed at reducing the symptoms, use of rescue analgesia, and disease progression, which in turn may provide benefit in patient’s mobility, QoL, and health care resource needs by delaying joint replacement surgery. 5 Management of OA involves elimination of modifiable risk factors by nonpharmacological measures, pharmacological measures (fast- and slow-acting drugs), followed by invasive treatment in the later severe stages. 6 Among the pharmacological measures, nonsteroidal anti-inflammatory drugs (NSAIDs) are preferred over paracetamol in effectively controlling pain; however, upper gastrointestinal (GI) and cardiovascular risks are also associated with NSAIDs.7,8 Chronic Symptomatic Slow Acting Drugs for Osteoarthritis (SYSADOAs) associated with a slow onset of action along with symptom control may delay the progression of joint structural changes. Among the SYSADOAs, prescription crystalline glucosamine sulfate (pCGS) lowers the use of drugs for rescue analgesia, including NSAIDs. 9
Despite the existence of several national and international evidence-based guidelines for OA management, there is no agreement on the different treatment modalities including pharmacological and nonpharmacological therapies.10-13 Furthermore, many of the existing guidelines are country-specific and have been designed on an individualized assessment of the patient, considering patients requirements or the subjective interpretation by the physician. Thus, evidence-based recommendations following country-specific regulatory guideline is vital in providing appropriate interventions for OA management in a heterogeneous population, especially in Ukraine, Kazakhstan, Uzbekistan, and Armenia. In the current article, the members of the expert committee convened a meeting to explore a general agreement on using a reviewed stepwise approach for the management of OA. The primary objective of this work was to provide an expert opinion on the use of pCGS in the management of OA in Ukraine, Kazakhstan, Uzbekistan, and Armenia.
Methodology
Expert panel and scope
In October 2018, a panel of 10 expert physicians (7 rheumatologists and 3 orthopedic surgeons) met in Ukraine to discuss available evidence on the use of pCGS in the treatment of OA. The panelists were chosen based on their expertise in areas of rheumatology, orthopedics, and musculoskeletal diseases and experience in clinical trials on rheumatic diseases. The panel reviewed variations in treatment modalities and real-world evidence for the better management of OA. Recommendations were made to optimize (1) an integrated approach toward OA management, (2) early incorporation of SYSADOAs (pCGS) in the treatment regimen for Ukraine, and (3) modified approaches in diagnostics and evaluation including the use of volumetric magnetic resonance imaging (MRI) for enhancing the clinical outcomes.
An integrated multiple-choice survey was conducted among the expert panel including questions on evidence-based treatment of OA with the administration of SYSADOAs, combination therapy with oral analgesics, and oral anti-inflammatory drugs (eg, usefulness of SYSADOAs in clinical practice in patients with shoulder OA, coxarthrosis, gonarthrosis, OA in hand, other pathologies; the most appropriate SYSADOA for knee OA treatment, etc).
In brief, each panelist was asked to generate opinion or statement for specific questions regarding the management of OA. A serial brief discussion was led by the moderator to clarify the opinions or statements by each panel members using the available evidence from the published literature and voted privately. The statement or opinion receiving maximum votes was used to form an opinion on the use of pCGS in the stepwise management of OA.
Systematic literature analysis
The expert opinion for OA treatment using pCGS in Ukraine is based on the critical assessment of the up-to-date literature that were systematically analyzed using Medline, EMBASE, CIHNAL, and Cochrane Library databases. The general approach is concentrated on two main components (a) specifically for the management of OA using pCGS and (b) the existing references and related clinical implications (meta-analysis of randomized controlled trials [RCTs]); RCT; controlled study without randomization; expert committee reports or recommendations or clinical experience of respected authorities, or both; nonexperimental descriptive studies, such as comparative, correlation, cohort study and case-control studies). Review articles and commentaries were excluded, and only guidelines in English were considered.
Diagnosis of OA
Radiography remains a mainstay in the diagnosis of OA. Radiographs are used to evaluate joint space narrowing (JSN), Kellgren-Lawrence grading scheme, 14 and the Osteoarthritis Research Society International (OARSI) classification score establish guidelines for the diagnosis of OA progression. 15 MRI is recommended as it evaluates early OA changes in cartilage biochemical composition and provides valuable high-resolution morphological details of joint tissue along with quantitative metrics of joint soft tissue condition. 16 In this regard, positron emission tomography/magnetic resonance (PET/MR) systems permit simultaneous, sensitive, and qualitative assessments of the morphological and functional features of the whole joint. 16 Proteo-glycans are complex molecules with negatively charged glycosaminoglycan (GAG) side chains on protein core. Proteoglycans depletion is a result of enzymatic degradation in cartilage in OA. Eventually, early diagnosis and potential treatment monitoring are possible by recognizing these variations in GAG content and distribution. A new advanced method, chemical exchange saturation transfer imaging of GAG (Gag CEST) makes it possible to detect endogenous GAG content in cartilage. 17
Management OF OA
Nonpharmacological therapy
Nonpharmacological interventions, in parallel to the pharmacological treatment modalities, have been recommended for the management of OA and associated comorbidities (Table 1). The core set of nonpharmacological treatment includes information access or education, weight loss in case of overweight individuals, and an exercise program (eg, aerobic, strengthening, or resistance exercises). 18 Patients should be referred to a physical therapist/other specialist for assessing whether correction for varus/valgus malalignment is needed. Correction using knee braces appears to be preferable as compared with wedged insoles. Furthermore, throughout the treatment, assessment of whether other physical interventions (in combination with pharmacological interventions) are useful in providing additional symptom relief should be performed. 18 The emphasis on patient-oriented nonpharmacological interventions limits the usage of pharmacological drugs, thereby restricting the adverse effects (AEs) related to their chronic use.7,19 However, core therapies are usually not adequate to control postdiagnosis symptoms of OA: thus, a combination of nonpharmacological and pharmacological therapies is strongly recommended. 7
Treatment modalities for the management of OA.
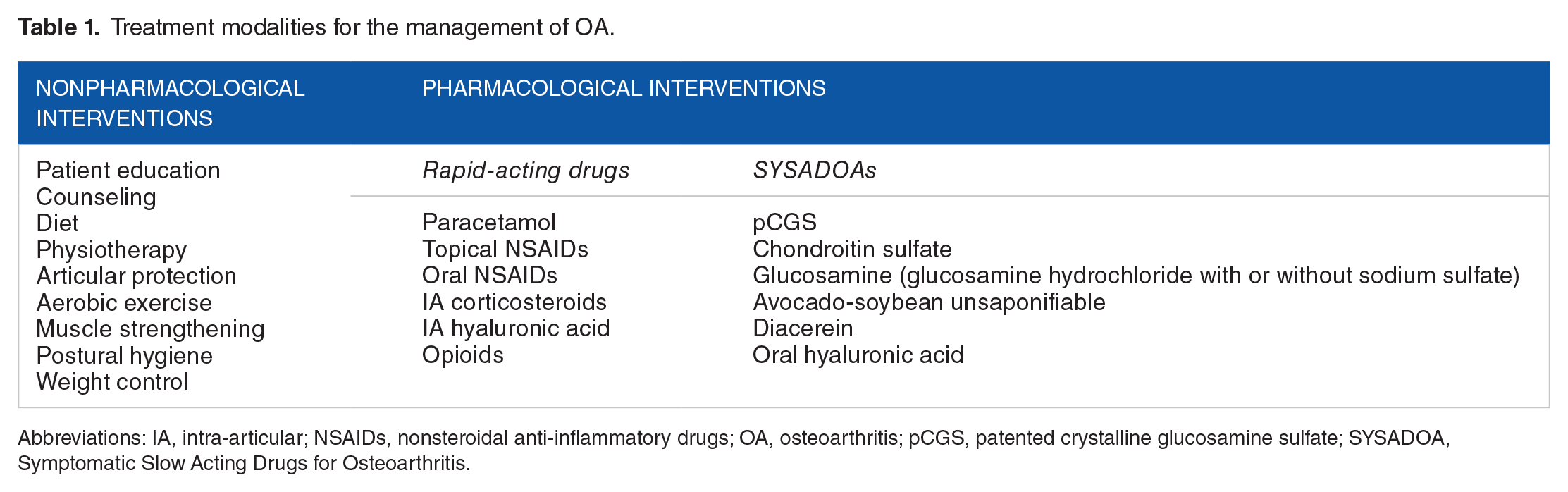
Abbreviations: IA, intra-articular; NSAIDs, nonsteroidal anti-inflammatory drugs; OA, osteoarthritis; pCGS, patented crystalline glucosamine sulfate; SYSADOA, Symptomatic Slow Acting Drugs for Osteoarthritis.
Pharmacological therapy
The pharmacological approach in symptomatic OA management mainly focuses on improvement or control of symptoms, pain, and underlying inflammation resulting in a reduced need for rescue analgesia and joint replacement surgery (Table 1).5,20 Although paracetamol has minimal effects on symptoms, it is widely recommended as a first-line oral analgesic, presumably due to its availability, low cost, and assumed safety.5,21 Recent studies raise concerns over the safety profile of paracetamol and its role in routine and chronic treatment. Uncertainty over efficacy in terms of reduction in stiffness and pain has been reported for paracetamol compared with placebo among patients with OA.5,10,21-24 Moreover, the use of paracetamol particularly for prolonged durations is associated with a greater risk of a dose-dependent increase in mortality, cardiovascular, upper gastrointestinal, and renal toxicity.5,8,10,25 Because of safety concerns and poor evidence to support the efficacy, paracetamol on a regular basis is no longer recommended for initial treatment of OA. Paracetamol may still be used in primary care to treat pain in patients with mild-moderate OA at daily doses up to 3 g/day. However, paracetamol may not be the drug of choice if it is found insufficiently effective and physicians should, therefore, consider modifications in treatment along with other therapies. 5 Recent network meta-analysis has shown NSAIDs to be associated with moderate effect compared with paracetamol or placebo for a duration of ⩽ 12 weeks and short-term use has been recommended due to safety concerns. 24 Therefore, a safer approach would be to use SYSADOAs, with as-needed paracetamol and NSAIDs for short-term, rescue analgesia.
OA drugs have been categorized as Symptom-Modifying Osteoarthritis Drugs (SMOADS) which are divided into two major subcategories: (1) rapid-acting drugs including analgesics, NSAIDs, and intra-articular (IA) glucocorticoids and opioids; (2) SYSADOAs.5-7,11
In accordance with the different existing recommendations,5,26,27 early administration of pCGS has been proposed by the expert panel for the management of OA (Figure 1).

Stepwise treatment recommendation for management of OA. CS indicates chondroitin sulfate; IA, intra-articular; IM, intra-muscular; NSAIDs, nonsteroidal anti-inflammatory drugs; OA, osteoarthritis; pCGS, patented crystalline glucosamine sulfate; PO, per oral; SYSADOA, Symptomatic Slow Acting Drugs for Osteoarthritis.
Step 1: background pharmacological management of mild OA symptoms
The aim of this intervention is to provide early relief, improving the symptoms in mild OA. In step 1 of the algorithm, the preferred approach is to initiate background therapy with SYSADOAs (pCGS or chondroitin sulfate [CS]), with the addition of paracetamol/NSAIDs as short-term rescue analgesia as needed. Combined dosing of glucosamine with CS is not recommended because of unfavorable pharmacokinetic interactions (reduced bioavailability of glucosamine). 28 Other SYSADOAs (avocado-soybean unsaponifiable, diacerein, etc) have limited preclinical evidence and no conclusive data on effectiveness in humans. However, in the case of symptomatic patients even after receiving appropriate background therapy with paracetamol, topical NSAIDs are recommended to achieve sufficient relief. 5 Furthermore, topical NSAIDs are preferred over oral ones in OA patients with comorbidities. 5 Prolonged use of oral NSAIDs among elderly people with OA is associated with considerable side-effects. 29 Oral NSAIDs may cause major GI complications in elderly, renal complications, increase blood pressure, and are also linked with development and acceleration of congestive heart failure. 29 Oral pCGS of 1500 mg per day or intramuscular (IM) pCGS at least 400 mg thrice a week for 4 to 6 weeks has been recommended. 30 IM pCGS is indicated for flare or acute attacks of OA depending on the patient’s preference. The combination of pCGS with paracetamol or NSAIDs should be considered up to 15 days, further continuing with SYSADOAs alone.
Step 2: advanced pharmacological management of moderate OA symptoms
In the case of inadequate relief, persistent pain, and restricted function even after receiving background therapy, advanced pharmacological intervention is recommended. This has also been recommended for treating patients suffering from moderate-severe OA. SYSADOA (pCGS alone or with supplements) along with oral NSAIDs up to 15 days has been recommended. Oral NSAIDs are preferred if first-line therapy including SYSADOAs and topical NSAIDs provide inadequate efficacy. They provide a greater improvement in the disease-specific QoL with significantly decreased levels of pro-inflammatory cytokines (interleukin [IL]-6, vascular endothelial growth factor, tumor necrosis factor-alpha) in the synovial fluid. 31 The effect size for relief of NSAIDs is small to moderate (0.27-0.44), but twofold greater than the effect size of paracetamol (0.18) and similar to SYSADOAs (0.27).10,32 NSAIDs may be more appropriate in combination with SYSADOA in OA patients with persistent pain and receiving SYSADOA alone. Selective, partially selective, and cyclooxygenase-2 (COX-2) inhibitors and nonselective NSAIDs have similar efficacy. 5 Intermittent or continuous use of NSAIDs in longer cycles is preferred over chronic use, for symptoms control, due to safety concerns and scarcity of long-term trials. 5 Therefore, modification in the treatment regimen and drug selection should be based primarily on the patient’s condition and related risk factors along with the physician’s preference.
Viscosupplementation with intra-articular hyaluronic acid (IA HA) injections, or corticosteroids for management of OA as a second-line option has been recommended for symptomatic patients receiving NSAIDs. IA injections with platelet-rich plasma (PRP) have been recently used to promote soft tissue healing and reduce inflammation. A recent RCT evaluating the effects of PRP or IA HA injections in patients with knee OA documented that PRP is an effective treatment that reduced pain and improved functional status. 33 However, to date, no guidelines suggest its use in patients with knee OA; therefore, further research is needed to reach more conclusive results, although this method has been used for a long time in the treatment of patients with sports injuries of the knee joint, in the rehabilitation complex after arthroscopic manipulations, including those for the prevention of OA progression.
On the other side, the effectiveness of hyaluronic acid (HA) from RCTs has been reported, with a high effect size of 0.63 compared with oral placebo. 5 IA HA injections have long-lasting benefits of reducing pain and increased function in knee OA, as compared with IA corticosteroids. 34 Although a slightly higher incidence of local reactions and flares have been reported with IA HA injections, they are mostly considered to be safe, with only mild-moderate transient local AEs reported. 34 This step also involves reevaluation after 15 days of treatment to assess the severity and modification in case needed.
Step 3: last pharmacological management of severe OA symptoms
The advisory expert panel recommends the last pharmacological step for the treatment of severely symptomatic OA patients. In addition, OA patients receiving previous treatments and still undergoing functionality problems and persistent pain are recommended for this treatment. SYSADOA (pCGS alone or with other supplements) along with oral NSAIDs up to 15 days with IA injection of steroid and short-term duloxetine have been recommended if apparent synovitis is present. Although IA corticosteroids are effective in reducing pain, the benefits are short lasting, usually not more than 6 to 8 weeks. 35 The depleting efficacy over time may lead to pain in few patients, and frequent injections (or injections without exudative synovitis) lead to degradation of articular cartilage matrix and the rapid progression of OA. 35 Therefore, the selection of combination should be critically monitored. Opioids are associated with significant morbidity, respiratory depression, and may result in dependence and drug abuse. 36 Generally, opioids utilization depends on safety, consent, and cost-effectiveness and their availability in the markets of certain countries.5,29
Duloxetine, a selective inhibitor of serotonin and norepinephrine reuptake increasing the inhibitory descendent pathway reduces the neuronal pain transmission. 37 The combination of duloxetine with NSAIDs has also been found to significantly reduce the pain. 38
Reevaluation after 15 days of combination therapy should be conducted to assess the progression of the disease and effectiveness of the treatment regimen. NSAIDs, opioid analgesics, and duloxetine possess a similar toxicity profile in long-term use to that of joint replacement surgery. 11 Categorization of patients and careful selection should be considered before deciding the appropriate treatment. This stepwise approach depending on the severity and complexity of the disease may help to minimize the risks factors involved.
Inferences From the Integrated Survey
The panel reached an agreement for pCGS as the drug of choice in the treatment of OA particularly in patients with poly-therapy. It also reviewed and agreed on the limiting effect of pCGS on the usage of oral analgesics and oral anti-inflammatory drugs (NSAIDs, selective COX-2 inhibitors, corticosteroids, opioids). On the basis of personal clinical experiences, the advisory panel suggested that the only reason for not prescribing SYSADOA treatment is the patient’s putative allergic response to ingredients and/or patient’s choice. The common side-effects associated with the SYSADOAs treatment are constipation, gastritis, diarrhea, nausea, and flatulence. 39 The expert opinion from the multiple-choice survey conducted during the expert opinion meeting is summarized in Table 2.
Recommendations based on real-world data from panel survey for the management of OA.

Abbreviations: AE, adverse effects; COX-2, cyclooxygenase-2; CS, chondroitin sulfate; ESCEO, Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases; IA HA, intra-articular hyaluronic acid; NSAIDs, nonsteroidal anti-inflammatory drugs; OA, osteoarthritis; pCGS, patented crystalline glucosamine sulfate; SYSADOA, Symptomatic Slow Acting Drugs for Osteoarthritis.
Sysadoas: Glucosamine Hydrochloride and Glucosamine Sulfate
Use of SYSADOAs regimen in OA includes prescription glucosamine sulfate (pGS), glucosamine hydrochloride (GH) (with or without sodium sulfate), CS, avocado-soybean unsaponifiable (ASU), diacerein, and HA.5,11 The SYSADOAs are orally administered for prolonged treatment courses and have the potential to decrease the use of NSAIDs and other rescue analgesic drugs. 9 The pGS and CS have been shown to be most effective among all the SYSADOAs. 5
Glucosamine formulations: Glucosamine (2-amino-2-deoxy-D-glucose), is a naturally occurring amino monosaccharide, essential for cartilage matrix and synovial fluid. Chemically, it is a base having a low molecular weight of 179.17 g/mol. The formulations of glucosamine for managing OA include GH and glucosamine sulfate (GS).6,40
GH is the most readily available glucosamine salt (MW = 215.56 g/mol), commonly used in dietary supplements and generic glucosamine products in a daily dose of 1250 mg.9,40
GS is a highly unstable hygroscopic compound (MW = 456.43 g/mol). However, it might be stabilized by a patented process with sodium chloride to obtain a prescription-grade patented crystalline glucosamine sulfate (pCGS) (MW = 573.31 g/mol) (Figure 2) and administered in a daily dose of 1500 mg.40,41
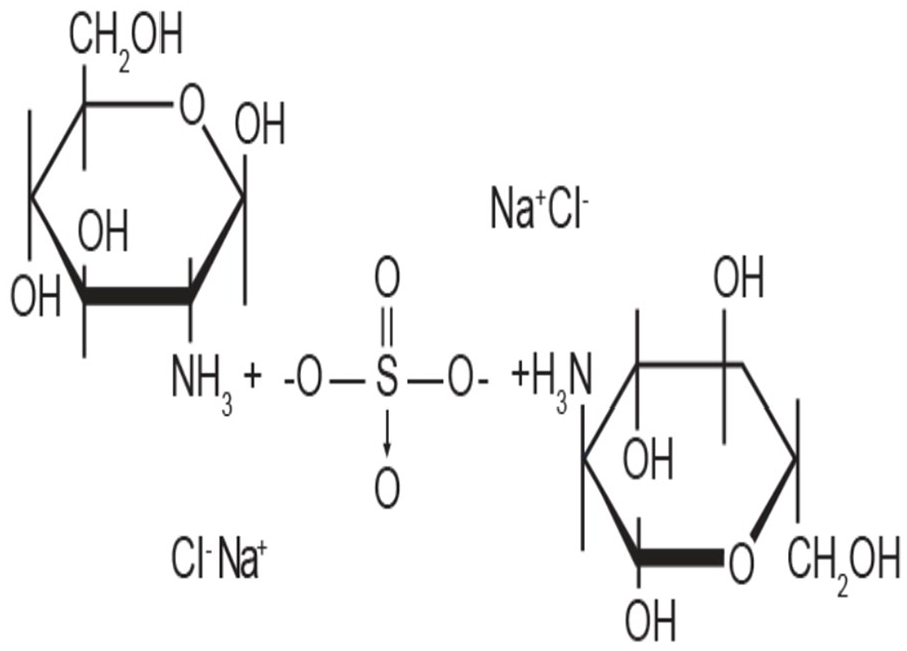
Molecular structure of stable crystalline glucosamine sulfate.
In addition to the prescription-grade, undocumented nonpharmaceutical grade GS, administered as 500 mg 3 times daily and differing in bioequivalence from the crystalline variant, is also commercially available. 40 Detailed structural analysis has revealed the nonpharmaceutical grade as a mixed salt of GH and alkali sulfate. 42
Prescription Glucosamine Sulfate Downregulates Key Genes Involved in Inflammation
The anti-inflammatory properties of pCGS are attributed to the reversal of the pivotal pro-inflammatory role of IL-1 involved in cartilage degradation. 5 GS also controls the stimuli for inflammatory cascade by reducing a host of inflammatory responses including cyclooxygenase-2 (COX-2), inducible form of nitric oxide synthase (iNOS), and prostaglandin E2 (PGE2) activity.43,44
The prescription-grade pCGS exhibits a stronger inhibitory effect than GH on joint degeneration mediators including IL-1β, matrix degradation factors (MMP-3), and ADAM-TS5 (aggrecanase 2) at a cellular concentration in the range of 10 µM which is similar to its concentration in synovial fluid after 1500 mg dose of pCGS.43,45
Glucosamine induces tissue regeneration by enhancing stem cell proliferation, and chondrogenic and osteoblastic differentiation. 46 Furthermore, it increases the levels of anti-inflammatory cytokines (IL-2, IL-10), lowers p38 MAPK and c-JNK expression, increases extracellular-signal-regulated kinase (ERK1/2) expression, inhibits nuclear factor-kB (NF-kB) and nod-like receptor protein 3 (NLRP3) inflammasome and caspase-1 activation. Glucosamine also possesses antioxidant properties. It reduces oxidative stress (intracellular reactive oxygen species levels) in chondrocytes, scavenges reactive oxygen species radicals, and upregulates the levels of antioxidant proteins/enzyme (eg, glutathione, superoxide dismutase, catalase), and inhibits endogenous reactive oxygen species production. In addition, glucosamine induces autophagy. 46
Clinical Benefits of pCGS
The efficacy and safety of glucosamine sulfate have been explored extensively in multiple RCTs. A pooled analysis from 25 RCTs (n = 4963) generally favored pCGS over any non-pCGS formulation (other GS and GH) in pain reduction based on the evaluation of the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores. 47 Furthermore, the effect size of GH for pain reduction was insignificant compared with pCGS due to the complications related to formulations, doses, and pharmacokinetics.9,40 In another large meta-analysis of 25 trials (n = 3458), pCGS formulation resulted in superior outcome compared with other formulation (P = 0.0032). 48 This finding is consistent with the recent larger network meta-analysis of 47 RCTs (n = 22,037) involving 31 pharmacological interventions where pCGS was found to be associated with a decrease in pain even with a follow-up of 1 year or longer. 24 In two large 3-year double-blind, randomized, placebo-controlled trials in knee OA, no significant loss of joint space was observed in pCGS group compared with the placebo group.49,50 The knee OA patients from these two RCTs upon 5-year follow-up after pCGS discontinuation showed a 57% decrease in the incidence of Total Joint Replacement (TJR). 51 The pivotal Glucosamine Unum In Die (once a day) Efficacy (GUIDE) trial reported pCGS to be more effective than placebo (P = 0.032) following its administration for a 6-month treatment course. 52
In the cohort study of Pharmaco-Epidemiology of GonArthrosis (PEGASus), pCGS was the only SYSADOA that significantly decreased the use of NSAIDs by 36% in patients with knee OA. 9 Moreover, pCGS has been reported to be safe for long-term usage considering AE rate comparable with that of placebo.20,48,50 Often, the pre-fixed combination of SYSADOAs are available in the market. Therefore, it is important to highlight that combination of GH and CS reduces GH plasma levels and has been reported to lack any additional benefits. 28 The effect of combined dosing of GH and CS has not been explained by their synergism on intestinal absorption requiring further research. 28 Altogether, these evidence support the safety and efficacy of pCGS in its recommendation for the treatment of OA.
On this backdrop, prescription-grade formulations of complex molecules, namely pCGS, harnessing the biological activity are considered for maximization of the clinical benefits. Interestingly, European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO) recommends that complex molecules with biological activity such as pCGS may be treated as “biosimilars” akin to the European Medicines Agency guidance on biological medicinal products. 53
Discussion
An expert panel provided an agreement on stepwise treatment modality for better management of OA. The main purpose of this meeting was to publish a framework for the early management of OA to respective specialists, patients, associated organizations, and regulatory bodies. The current approach is in accordance with the perspective of the recently published ESCEO algorithm, 18 focusing on early symptomatic relief in OA but with a modified evidence-based recommendation for advanced management in Ukraine, Kazakhstan, Uzbekistan, and Armenia. Nonpharmacological interventions have an important role in OA management. A comprehensive approach concentrating on the associated risk factors and comorbidities has also been recommended for the treatment of OA.
Due to disparities in available treatment modalities in OA, especially regarding the use of specific glucosamine salt, the current work proposed an expert opinion on the best-available step-by-step treatment approach for OA, focusing on early intervention by pCGS. It also provides parallel recommendation of other treatment regimens depending on the severity of OA and the patient’s condition. The real-life evidence of the disease-modifying effects of pCGS supports early incorporation into the treatment regimen. The multimodal approach and combination of pCGS with short-term analgesic aids in pain relief and inhibits disease progression. Following the treatment of OA with pCGS, paracetamol, and topical NSAIDs, the treatment recommendation deviates from ESCEO consensus algorithm 2019. 18 In this review, the panel proposes chronic use of pCGS in the advanced pharmacological interventions, whereas the existing ESCEO algorithms recommend intermittent or continuous use of oral NSAIDs in longer cycles in step 2 along with the IA HA or IA corticosteroids and short-term weak opioids alone in step 3.7,18 The current multimodal therapy concentrates on combination of pCGS with oral NSAIDs and IA HA or IA corticosteroids, and IA steroid with duloxetine in step 2 and 3, respectively. Viscosupplementation with IA HA for the long-term management of OA has been recommended because of the efficiency and high effect size. 18 Long-lasting benefits of IA HA in reducing pain and increased function are superior to IA corticosteroids. 54 From baseline to week 4, intra-articular corticosteroids appear to be relatively more effective for pain than intra-articular HA. By week 4, the two approaches have equal efficacy, but beyond week 8, HA has greater efficacy. 49
However, limited usage of IA HA and glucocorticoids has been proposed to restrain the related hazardous effects. At last, for chronic OA, duloxetine in a combination of NSAIDs with pCGS has been proposed for a reduction in pain. 38 Although existing algorithms ESCEO 2014 and 20195,7 and the European League Against Rheumatism (EULAR) recommendations published in 2003, 11 highlight the symptomatic efficacy and structure-modifying effect of SYSADOAs, chronic use of pCGS in combination has not been discussed.
Our recommendation focuses on the joint structure-modifying effect of pCGS while reducing the AEs by limiting the use of oral NSAIDs, IA HA, and corticosteroids. The combination modality may minimize risks while maintaining the clinical benefits of treatment, resulting in a decline of rescue analgesia, joint replacement, and thus a subsequent reduction in health care requirements and improving QoL.20,55 Withdrawal of pCGS at later stages is not recommended since OA is a systemic disease and it is necessary to protect the other joints that are not affected. Among SYSADOAs, high WOMAC total score decrease has been associated with glucosamine over placebo. 47 While pCGS remains the only SYSADOA that restricts the usage of NSAIDs in knee OA, 9 it is considered safe in long-term with low AE rate.20,48,50 pCGS can be safely prescribed in combination with other drugs, to patients with comorbidities and elderly. Moreover, pCGS has no AE on glucose metabolism and is considered safe in liver diseases. 56
Restricted usage of paracetamol has been proposed due to the augmented risk of GI complications and multiorgan failure. 57 In comparison with OARSI 2008 19 and EULAR 2003 11 recommendations, current treatment modality differs notably in limiting the usage of NSAIDs, opioids, and narcotic analgesics. The pCGS-based multimodal combination therapy may contribute to reducing consumption of oral analgesics and oral anti-inflammatory drugs for degenerative OA. The early combination therapy of SYSADOAs with paracetamol or NSAIDs has been suggested, but prolong usage has been discouraged too. In accordance with the existing ESCEO algorithm and recommendation,5,7 topical NSAIDs have been recommended due to the indicative efficacy and promising safety profile as compared with oral NSAIDs. The prescription of topical or oral NSAIDs is dependent on the patients’ preference and severity of the disease. But the lowest effective dose of NSAIDs for shorter durations has been recommended. 5
The present evidence-based review incorporates pCGS as an extensive arm of the combination therapy in each step accounting for its effectiveness, affordability, and low economic burden. Cost-effectiveness of GS makes it a drug of interest compared with paracetamol. 58 pCGS provides an improved affordable treatment, for an extensive time range of 3 months to 3 years. 59 Moreover, early administration of pCGS assists in better pharmaco-economical outcome by controlling the usage of analgesics, NSAIDs, and other health resources. 51
Recurrent revision of evidence and implications based on real-world data are important for the periodic modifications in the recommendations. However, it provides a representation of a modified framework for the development of future global recommendations, and this opinion from the experts may be adapted for use in different countries.
Conclusion
In conclusion, the proposed expert view from the panel targets the early pharmacological disease control while limiting the AEs due to chronic use of suggested NSAIDs and analgesic drugs. The main reason for diverse findings is the varied range of available glucosamine formulations, but pCGS has a disease-modifying effect and provides consistent relief from OA, without the development of adverse drug reactions or drug-drug interactions suggesting that this form of glucosamine may influence the outcomes. The incorporation of pCGS into the treatment regimen at every step may provide active control over disease progression and early symptomatic relief in OA. To maximize benefit, early administration of pCGS in treatment regimen after diagnosis and its long-term continuation has been recommended. The pCGS-based multimodal treatment is also cost-effective and positively impacts the cost of the overall chronic treatment of OA. The current evidence-based stepwise approach for management of OA may aid in effective management and adherence, thus providing a framework for specialists to manage OA efficiently in Ukraine and other countries.
Footnotes
Acknowledgements
The authors acknowledge Swati Krishnan, PhD and Ramu Periyasamy, PhD (Indegene Pvt. Ltd.) for providing medical writing support and technical assistance in developing the consensus manuscript.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Mylan Inc.
Author Contributions
All authors have equally contributed in the development of the manuscript.