
Abstract
Introduction:
Tibial slope angles (TSAs) have been identified as potential risk factors of anterior cruciate ligament (ACL) injury in the literature. A higher body mass index (BMI) might increase the risk of ACL tear because of greater axial compressive force. The aim of this study was to determine the relationship of these factors and the combined effect of BMI and TSA in determination of risk potential for ACL injury.
Methods:
The preoperative magnetic resonance (MR) images of 81 ACL-injured male knees and of 68 male individuals with no ACL injuries were evaluated by 2 radiologists to measure the TSA. The Mann-Whitney U-test was performed to indicate the significant difference in height, weight, and BMI values. The independent samples t-test was used to determine the differences between ACL-injured and non-injured groups regarding TSA values. Odds ratios were calculated by logistic regression tests, and receiver operating characteristics (ROC) curves revealed the area under the receiver operating characteristics curve (AUC) values to compare the relationships of these parameters with ACL injury.
Results:
Body mass index, lateral tibial slope (LTS), and medial tibial slope (MTS) were predictive of ACL risk injury. Body mass index alone had the greatest effect among these parameters, and there were no statistically significant differences in coronal tibial slope values between the ACL-ruptured and control groups. The greatest AUC was observed for the combination of BMI, MTS, and LTS.
Conclusions:
Body mass index, LTS, and MTS angles were associated with ACL injury risk and BMI + MTS + LTS together revealed the greatest effect on ACL injury.
Introduction
There are many reports on the results, techniques, postoperative complications, and treatments of anterior cruciate ligament (ACL),1–9 but there are fewer reports on the risk factors and causes of ACL injuries.10–13 The relationship between various anatomical factors and ACL injury is still a topic of interest to researchers. Some structural variations, such as narrower femoral notch width, decreased notch width index and notch width angle, steep plateau, and shallow tibial plateau, have been reported as possible risk factors of ACL injury in previous studies.11,13–22 A steep tibial plateau is one of the important risk factors for ACL injuries, and researchers have measured the tibial slope angles (TSAs) in patients with ACL injury regarding ethnicity, age groups, sex differences, or various branches of sporting activities.23–27
Body mass index (BMI) is another parameter that is considered to be related to lower extremity injuries. 28 In a study by Evans et al, 29 elevated weight and BMI values have been found to be significantly associated with ACL injuries, especially in male individuals. BMI has also been found to be associated with other intra-articular injuries observed during ACL reconstructions.30,31
There are few studies in the literature on the combined effects of tibial slope and BMI on ACL injury. The aims of this study were to identify the effects of BMI and TSA as possible risk factors for ACL injury in male knees, to investigate the combined effect of these factors, and to determine the odd ratios for each factor and for the combined effect of BMI and TSA on ACL rupture.
Methods
Patients
This case-control study was approved by the Ethics Commitee of Kafkas University. The ethics committee waived the requirement for informed consent form because of the study design. According to the results of a power analysis, a minimum of 49 subjects was necessary to establish 90% power to determine the statistical significance of differences in this study. Five patients who had poor quality magnetic resonance (MR) images (n = 1), advanced osteoarthritis with grade > 2 Outerbridge classification (n = 1), and patients with ACL tears presenting > 3 months after injury (n = 3) were excluded from this study. For both the patient and control groups, male patients ⩾ 18 and <50 years old were included in this study to avoid the structural changes in osteoarthritis, which could possibly have affected the results of the slope angle measurements. Accidental or injurious events without any direct blow to the knee were accepted as non-contact knee injuries. All male patients with non-contact ACL injury in this age group who had undergone ACL reconstruction between January 2011 and November 2017 in our institution were assigned to the patient group. After exclusion of 5 patients, a total of 81 patients were included (25.44 ± 1.35 years; range, 18–43 years) in this group. Patients who had undergone orthopedic surgery for other reasons, such as meniscal injury (n = 27), infected Baker cyst rupture (n = 4), patellar dislocation (n = 2), plica excision (n = 1), and unexplained joint effusion (n = 1) in the same time period (between January 2011 and November 2017), and the patients treated at the Orthopedics Department of our hospital between January 2017 and November 2017 for knee pain (n = 21), sprain (n = 10), and knee locking (n = 2) with an intact ACL (35 patients with arthroscopic surgery confirmed and 33 patients with radiologically confirmed intact ACLs) were accepted as the control group. A total of 68 males of similar age (mean age, 23.60 ± 1.03 years; range, 18–36 years) were included in the control group. The median time interval between the injury and a magnetic resonance imaging (MRI) scan was 10 days (minimum time interval was 1 day and maximum time interval was 43 days) for the patients with ACL injury and 14 days (minimum time interval was 1 day and maximum time interval was 36 days) for the control group. The data of height and weight measurements of the subjects were obtained from the medical records of these patients. These data were used to quantify BMI (weight in kg/height in m2) values.
MRI protocol
All MRI scans were performed by using a 1.5T MRI machine (Magnetom Essenza; Siemens, Erlangen, Germany) and an 8-channel knee coil. The parameters of each MRI sequence were as follows: T1-weighted (T1W; sagittal plane) images: echo time (TE): 14 ms, repetition time (TR): 515 ms, matrix: 192 × 256, field of view (FOV): 160 mm, slice thickness: 3.5 mm, interslice gap: 0.7 mm, echo train length (ETL): 55, number of excitations (NEX): 2; axial proton density weighted (PDW) images: TR: 2500 ms, TE: 28 ms, matrix: 206 × 256, FOV: 170 mm, slice thickness: 3.5 mm, interslice gap: 0.7 mm, ETL: 69, NEX: 1; coronal PDW images: TR: 2350 ms, TE: 26 ms, matrix: 205 × 256, FOV: 180 mm, slice thickness: 3.5 mm, interslice gap: 0.7 mm, ETL: 69, NEX: 1; sagittal PDW images: TR: 2670 ms, TE: 24 ms, matrix: 205 × 256, FOV: 190 mm, slice thickness: 3.5 mm, interslice gap: 0.7 mm, ETL: 70, and NEX: 1 for all knee MR examinations. Each patient included in this study was examined in the supine position, with approximately 15° of external rotation of the knee and slight knee flexion (range, 10°-15°). Magnetic resonance imaging slices started above the trochlear groove and extended below the tibial tubercle. Suprapatellar joint recess was included in each MR examination.
MRI measurements
Magnetic resonance images were re-assessed by a general radiologist with 20 years of experience and a musculoskeletal radiologist with 12 years of experience independently. These 2 radiologists measured the posterior medial tibial slope (MTS), posterior lateral tibial slope (LTS), and coronal tibial slope (CTS) angles for each patient on knee MR images. The procedure that was used to measure the TSA on MR images was based on the studies of Matsuda et al 32 and Hashemi et al. 27
Medial tibial slope and LTS were measured on sagittal T1W images. For both MTS and LTS, the sagittal plane which passed closest to the central point of the tibial plateau surface was identified with the aid of axial MR images that passed through the level of the tibial plateau. First, the longitudinal axis of the tibia (LAT) was drawn to measure these angles. It was represented by a line that passed through 2 points located in the center of the anterior-posterior width of the tibia. To indicate these midpoints, the width measurements were made as distally as possible in the sagittal image, approximately 4 to 5 cm apart in the sagittal plane. The LAT was drawn as the line that passed through these 2 midpoints of the tibial width. The most appropriate sagittal plane that showed the most centroid part of the tibial plateau was chosen to measure the posterior slope. The angle formed between the line perpendicular to the LAT and the line passed through the posterior and anterior peak points of the medial and lateral condyles of the tibia represented the medial and lateral posterior tibial slope (Figures 1 and 2). If the line perpendicular to the LAT was above the line that passed through the posterior peak point of the tibial plateau, then the slope angle was accepted as positive.

The sagittal LAT (longitudinal axis of the tibia) is drawn as the line that passes through the center points of the tibial width (left). The (blue) angle formed between the line perpendicular to the sagittal LAT (green line) and the line passing through the anterior and posterior peak points of the medial tibial plateau (yellow line) represents the medial posterior tibial slope (right).

The sagittal LAT (longitudinal axis of the tibia) is drawn as the line that passes through the midpoints of the tibial width (left). The line perpendicular to the sagittal LAT (green line) is drawn. The (blue) angle formed between this perpendicular line and the line that passes through the anterior and posterior edges of the lateral tibial plateau (yellow line) forms the lateral posterior tibial slope (right).
To measure the CTS, axial planes were used to determine the central image of the tibial plateau. Two width measurements were needed to draw the LAT. Tibial width measurements were made approximately 4 to 5 cm apart and as distally as possible in the coronal MR images. The coronal LAT was accepted as the line that passed through the 2 center points of these tibial width measurements. The angle formed by line perpendicular to the LAT and the line passing through the center points of the lateral and medial aspects of the tibial plateau indicated the CTS (Figure 3). If the perpendicular line was above the line that passed through the lateral peak point of the plateau, the angle was accepted as positive.

The coronal LAT (longitudinal axis of the tibia) is drawn as the line that passes through the 2 center points of the tibial width. The line perpendicular to the coronal LAT is drawn (green line). A line that passes through the medial and lateral edges of the tibial plateau surface (yellow line) and the line perpendicular to the coronal LAT forms the CTS (right). CTS indicates coronal tibial slope.
Statistical analysis
All statistical calculations were performed by using commercially available software MedCalc Software bvba. Acacialaan 22 8400 Oostende Belgium. According to the results of a power analysis, if the type 1 error was accepted as “0.05” and the power of the test was taken as “90%,” ⩾49 individuals for both the patient group and control group were needed to perform an analysis to determine the statistical significance of differences. The Kolmogorov-Smirnov test was performed to reveal the homogeneity of the data distribution. Box-Whisker and dot-plot methods were used together to show data distributions in a plot analysis. For the interobserver agreements, the results of each reviewer were compared by using interclass correlation coefficients (ICCs). The level of the interobserver agreements regarding the ICC values was classified as shown in Table 1. The significance of the differences in height, weight, and BMI was calculated by performing the Mann-Whitney U-test. The independent sample t-test was used to analyze the differences in the MTS, LTS, and CTS values between the patient and control groups. Receiver operating characteristic (ROC) curve analysis was performed for the BMI, MTS, and LTS values and combinations of these factors. The area under the receiver operating characteristics curve (AUC) was calculated for each of these parameters (BMI, MTS, LTS, MTS + LTS, BMI + MTS, and BMI + MTS + LTS) and used to compare these measurement results with each other. A Youden plot was used to compare the data distribution for MTS versus LTS values and BMI versus MTS values. Odds ratios were calculated by logistic regression tests. A P value of <.05 was accepted as indicative of statistically significant differences.
Interpretation of intraclass correlation coefficients for interobserver agreement.

Results
A total of 149 individuals (79 right and 70 left knees) were included in this study. Age, height, weight, BMI, MTS, LTS, and CTS were investigated to understand their possible relationships with ACL injury.
The data distribution of age values was homogeneous, and the results were presented as mean ± 2 standard errors (SEs). The mean age ± 2 SEs was 25.44 ± 1.35 for the patient group and 23.60 ± 1.03 for the control group. Height, weight, and BMI values showed a non-homogeneous data distribution (P = .034 for height, P = .044 for weight, and P = .035 for BMI). Therefore, the Mann-Whitney U-test was applied, and the median values of the parameters were used to show the differences, if any, between the patient and control groups (Table 2).
The age, height, weight, BMI, MTS, LTS, and CTS values of the ACL-ruptured and non-ruptured groups.

Abbreviations: BMI, body mass index; CTS, coronal tibial slope; ICC, intraclass correlation coefficient; LTS, lateral tibial slope; max, maximum value; min, minimum value; MTS, medial tibial slope; SE, standard error.
There were statistically significant differences in height, weight, and BMI values between the patient and control groups. The median height was higher in the control group than in the patient group, and the median weight was significantly greater in the patient group than in the control group according to the Mann-Whitney U-test (Table 2). The data distribution of the patient and control groups and ROC analysis of BMI values are shown in Figures 4 and 5. If the cutoff value was accepted as 23.99 for BMI, the sensitivity was 85.2% and the specificity was 52.9% for indicating ACL injury.

Data distribution of patient and control groups regarding BMI values. BMI indicates body mass index.

ROC analysis for BMI values. BMI indicates body mass index; ROC, receiver operating characteristic.
Statistical analysis revealed that there were significant differences in the MTS and LTS values but not in the CTS values between the patient and control groups. The plot analyses and ROC analyses of MTS and LTS are shown in Figures 6 to 9. For MTS, a sensitivity of 67.9% and a specificity of 61.8% for indicating ACL injuries were calculated for a cutoff value of 2.8. Receiver operating characteristic analysis of LTS revealed that LTS values > 3 were indicative of ACL rupture, with a sensitivity of 50.6% and a specificity of 73.5%.

Data distribution of patient and control groups regarding MTS values. MTS indicates medial tibial slope.

ROC analysis for MTS values. MTS indicates medial tibial slope; ROC, receiver operating characteristic.

Data distribution of patient and control groups regarding LTS values. LTS indicates lateral tibial slope.

ROC analysis for LTS values. LTS indicates lateral tibial slope; ROC, receiver operating characteristic.
The odds ratios of BMI, MTS, and LTS were 1.34, 1.46, and 1.26, respectively (Table 3), and ROC analysis revealed that BMI had the greatest AUC value among these parameters. Medial tibial slope + LTS had a lower AUC value than that of BMI alone, and the effect of BMI + MTS + LTS combination had the greatest AUC value among all the individual parameters and combinations (Table 4). Youden plot analyses were performed to determine the data distributions for MTS versus LTS and BMI versus MTS values (Figures 10 and 11).
Associations between BMI, MTS, LTS values, and the risk of ACL injury.
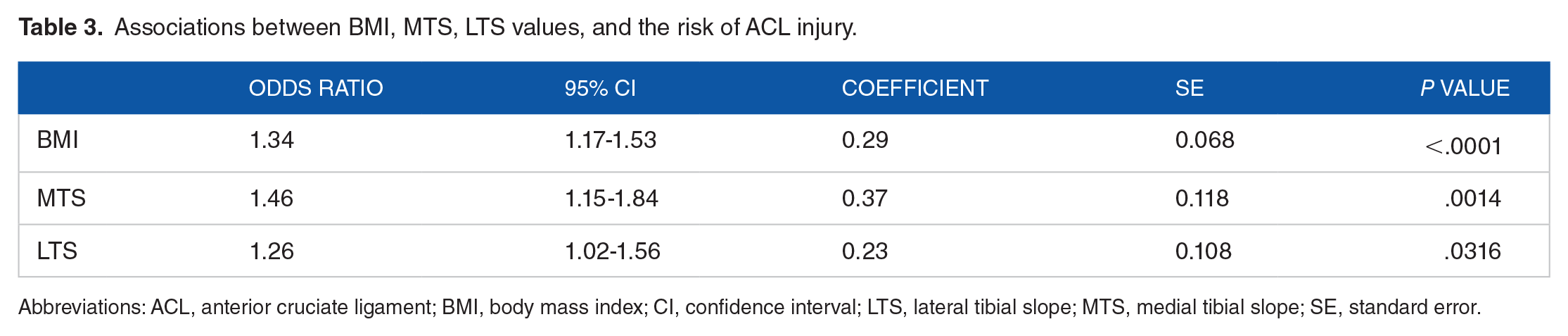
Abbreviations: ACL, anterior cruciate ligament; BMI, body mass index; CI, confidence interval; LTS, lateral tibial slope; MTS, medial tibial slope; SE, standard error.
ROC curve analysis of BMI, MTS, LTS values, MTS + LTS combination, BMI + MTS combination, and BMI + MTS + LTS together to determine the risk of ACL injury.

Abbreviations: ACL, anterior cruciate ligament; AUC, area under the receiver operating characteristics curve; BMI, body mass index; CI, confidence interval; LTS, lateral tibial slope; MTS, medial tibial slope; ROC, receiver operating characteristics; SE, standard error.

Youden plot analysis for MTS versus LTS. LTS indicates lateral tibial slope; MTS, indicates medial tibial slope.
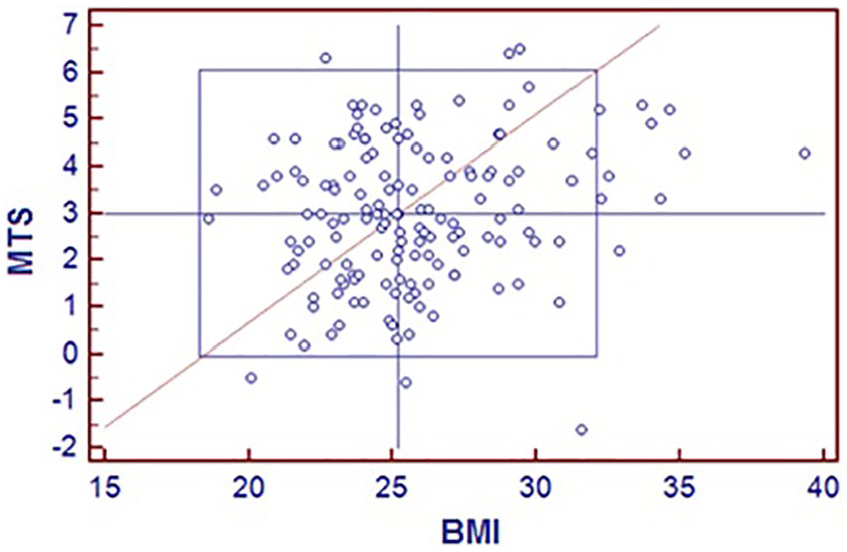
Youden plot analysis for MTS versus LTS. LTS indicates lateral tibial slope; MTS, indicates medial tibial slope.
Discussion
This study showed that BMI, MTS, and LTS had individual and combined effects on ACL rupture risk in men. In the literature, some studies have indicated that structural features and variances of the tibial plateau had a direct influence on the arthrokinematics of the tibiofemoral joint of the knee for translation, the screw-home mechanism, the location of instantaneous center of rotation, and the biomechanics of strain in the knee, which includes the ACL functions.33–35 The posterior tibial slope (with the elevation of the anterior edge of the plateau being higher than that of the posterior edge) is one of the important characteristic properties of the tibial plateau, and some authors have claimed that this property is associated with a large compressive joint reaction force produced during weight-bearing activities. This force might have an anteriorly directed shear force component that causes a corresponding anteriorly directed translation of the tibia.35,36 This slope has been measured in various studies, and the role of this structural property in anterior tibial translation has been stated by various authors in both animal 37,38 and human models.35,36 As the tibial plateau becomes steeper (the slope angle increases), the magnitude of the anteriorly directed shear force increases because of the increased compressive joint force on the tibial plateau during weight bearing.35,38,39
A study by Simon et al 40 (n = 54, with 27 ACL-injured cases) showed that an increased posterior tibial slope was associated with ACL injury, and Todd et al 21 (n = 319, with 140 ACL-injured cases) found that increased posterior tibial plateau slope was a significant risk factor of ACL rupture in women. Stijak et al 22 (n = 66, with 33 injured cases) claimed that increased LTS and Vyas et al 41 (case-control study, n = 39, with 16 injured cases) found that increased MTS was a significant risk factor of ACL injury. The results of Bisson et al 42 (case-control study, n = 80, with 40 injured cases) indicated that increased LTS was a risk factor of ACL rupture in men. A case-control study by Hashemi et al 11 (n = 104, 49 patients with ACL injury) found that increased LTS in women and both increased MTS and LTS in men were associated with ACL injury. More recent studies have also shown a relationship between tibial plateau slope and ACL injuries determined from measurements on MR images. In 2015, Dare et al 43 reported a statistically significant LTS difference between skeletally immature ACL-injured and non-injured individuals (mean age of the population, 14.8 ± 1.3, and n = 152 with 76 ACL-ruptured participants). In the same year, a study by Ghandour et al 44 also found a significant difference between ACL-ruptured and non-injured patients regarding LTS. Two important studies that included men revealed that both LTS and MTS were significantly different in the patient and control groups, and the ACL-injured individuals had a steeper tibial plateau than that of the non-injured ones.45,46
The effect of CTS on biomechanics of the tibiofemoral joint is not entirely understood.
Shultz and Schmitz 47 revealed that CTS measurements were associated with altered biomechanics of the knee joint. They suggested that greater CTS and LTS predicted greater internal rotation of the hip at initial contact and greater CTS predicted greater internal knee rotation excursions. Other studies have shown that greater internal knee rotation excursions and greater knee valgus angles had a role in ACL rupture, and these conditions were thought to be risk factors of ACL injury.48,49 Hashemi et al 27 claimed that CTS had an influence on the biomechanics of ACL injury and on the ligament balancing associated with unicompartmental reconstruction of the knee in which only one aspect of the knee joint is reconstructed. In this study, there was no relationship between CTS and ACL injury risk, a finding that was similar to the results of recent studies in the literature.23,45,50
Some authors have suggested that BMI is significantly associated with intra-articular injuries at the time of ACL reconstruction. 30 The effect of BMI on ACL injury risk remains a topic of interest in research. Some researchers claim that obesity interacts more than additively with knee injury as a risk factor of degenerative joint disease. 51 It is known that internal tibial rotation and anterior tibial translation increase ACL strain and ACL injury risk.52,53 Some authors have suggested that greater axial knee compressive force combined with greater body weight and/or greater BMI with a greater lateral posterior tibial slope would probably increase ACL strain and injury risk. 54 Evans et al 29 studied the predisposing risk factors for non-contact ACL injuries in military subjects. They concluded that weight and BMI were associated with ACL injury, and this correlation was more significant in men than in women. This study found a statistically significant relationship between BMI and non-contact ACL injuries.
For BMI, MTS, and LTS alone, the odds ratio of MTS was greater than that of the other parameters in this study. In addition, the greatest AUC value was observed for the combination of BMI, MTS, and LTS. However, there are some opposite results in the literature that show no relationship between BMI and ACL injury risk in men. Uhorchak et al 55 followed 895 cadets and found that higher than normal BMI in women was one of the risk factors for non-contact ACL injuries. This finding was not observed among male cadets. Moreover, Blanke et al 50 claimed that MTS and LTS were not associated with the risk of ACL rupture during non-contact injuries among recreational alpine skiers.
In the literature, there are valuable biomechanical and clinical studies indicating the importance of slope angles and BMI as they might play a role in ACL injuries; however, there are not much studies about the “combined effect of these parameters” on ACL rupture. The results of this study might be important to underline the “combined effect” of these parameters on ACL injuries. In addition to the contributions of this study to the literature, this study had several limitations that should be considered. First, the measurements were made by 2 experienced radiologists, but human error could have influenced the angle measurements, especially in a study with such small number of subjects; the ICC values between the observers were very high. On the contrary, the data distributions for height, weight, and BMI values were non-homogeneous, and parametric tests could not be applied to these parameters. Therefore, median values were used, which is another limitation of this study that should be taken into account when interpreting the study results. According to the power analysis, there were not enough female patients (meet our inclusion criteria) in our patient archives to perform suitable statistics. Therefore, the results of male individuals have been reported in this study. Moreover, the data were acquired retrospectively from image archives of the PACS system of our hospital and prospective studies with identical age, sex, and other demographic conditions probably provide more accurate results. Finally, the lifestyles of the study population were not evaluated. The daily lifestyles and sports activities of these individuals might have affected the results of this study.
In conclusion, BMI, MTS, and LTS were found to be associated with ACL injuries. Medial tibial slope had the highest odds ratio for ACL rupture, and the greatest AUC value was observed for the combination of BMI, MTS, and LTS.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
VK was the guarantor of integrity of the entire study. Study concepts were contributed by VK, HA, and AKS. Study design was carried out by VK, AKS, HA, GRU, and KT. Data acquisition was performed by VK, GRU, and TÇ. Data analysis and statistical analysis were carried out by AKS, VK, GRU, TÇ, and KT. Interpretation was done by VK, GRU, and TÇ. Literature research was done by VK, HA, and KT. Manuscript drafting was carried out by VK. Manuscript editing was done by VK, AKS, HA, GRU, TÇ, and KT.
Ethical Approval
This study has been approved by the Ethics Commitee of Kafkas University.