
Abstract
Introduction:
Knee injuries constitute a significant proportion of sports-related injuries. Osseous oedema can present in specific patterns with certain injuries
Objective:
This study aims to analyse the patterns of bone marrow contusion in the lateral tibial condyle (LTC) post knee trauma, categorising the condyle into anterior, middle, and posterior thirds, and to evaluate the prevalence of associated ligamentous and meniscal injuries.
Materials and Methods:
A cross-sectional study was conducted on 150 patients (92 males, 58 females) with an average age of 16.9 years, who underwent MRI within one week following knee trauma. The LTC was divided into anterior, middle, and posterior thirds for analysis. The bone marrow contusion patterns, along with associated ACL, MCL, PCL, LCL, medial meniscus, and lateral meniscus injuries, were documented.
Results and Analysis:
Bone marrow oedema in the LTC was observed as follows: anterior one third in 6, middle third in 13, and posterior third in 31 cases. The analysis revealed the following injury associations: Anterior one-third osseous oedema was associated with ACL injuries in two cases, MCL injuries in 3, PCL in 1, and medial meniscus injuries in 1. Middle one-third osseous oedema was associated with ACL injuries in 11 cases, MCL injuries in 3, medial meniscus injuries in two cases, and lateral meniscus injuries in 2. Posterior third osseous oedema was associated with ACL injuries in 28 cases, MCL injuries in 9, and medial meniscus injuries in four cases.
Conclusion:
The study highlights a clear association between the location of LTC bone marrow oedema and specific patterns of ligamentous and meniscal injuries. The posterior third, with the highest incidence of oedema, showed a strong correlation with ACL and MCL injuries, while anterior and middle oedema also demonstrated significant associations with ACL and MCL, and varied involvement of meniscal injuries. These insights contribute to a more comprehensive understanding of knee injury mechanisms, advocating for precise diagnostic strategies and potentially guiding more effective treatment protocols in radiological and orthopaedic practice.
Keywords
Introduction
The knee is a highly complex joint, experiencing constant stress not only during physical activities but also in everyday life.[1] In addition to the surrounding muscles, the knee’s stability heavily depends on passive stabilisers, including ligaments, menisci, and the joint capsule. Injury to any of these structures can result in chronic pain, knee instability, and an increased risk of early arthritis.[1,2] In recent years, traumatic knee injuries have become a growing concern, constituting a significant portion of sports-related incidents, making up about 32% of all musculoskeletal injuries in sports.[3–5]
Magnetic resonance imaging (MRI) is the most effective diagnostic tool for identifying ligamentous knee injuries.[6] Moreover, MRI offers the advantage of detecting radiographically occult osseous injuries[7–9] manifesting as bone contusions, commonly known as bone bruises.[5] The term ‘bone marrow oedema’ was initially introduced by Wilson et al. in 1988 when describing a group of patients experiencing debilitating knee and hip pain.[10] This appears as an ill-defined hyperintensity on T2-weighted MR images, in contrast to standard radiographs, which typically show nonspecific osteopenia or normal findings.[7,11–13] The manifestation of these abnormalities is believed to result from factors such as oedema or hyperaemia associated with trabecular injury.[13]
Furthermore, the presence of bone marrow oedema on MRI often serves as an indicator of an underlying soft-tissue pathology.[5,7–11,13] Clinicians use these findings to diagnose and address the root cause of the oedema. By examining the distribution of the oedema, a comprehensive understanding of the injury mechanism is gained, allowing for the accurate prediction of associated soft-tissue abnormalities.
This study aims to analyse the patterns of bone marrow contusion in specific regions of the lateral tibial condyle (LTC) following knee trauma and to assess the prevalence of concomitant ligamentous and meniscal injuries.
Methods
Local ethical committee approval was obtained for the study. We conducted a retrospective study that involved the analysis of 150 knee MRI scans of patients who had experienced traumatic knee injuries over a year period were included in the study. All MRIs were performed within one week of the injury [Table 1]. As traumatic knee injuries are common in young patients, patients who were younger than 30 years were included in the study. We excluded cases with tumours, prior surgical procedures, or infections.
Table showing inclusion and exclusion criteria
To investigate the injury patterns, we examined the LTC on proton density fat-suppressed images. Images were acquired on 1.5T Siemens Espree (Erlangen, Germany) or Philips MRI Ingenia Elition 3.0T. (FOV-160, TR 2499, TE 30, slice thickness -3 mm). The LTC was further divided into anterior, middle, and posterior thirds to facilitate a detailed analysis of injury distribution. We documented the patterns of bone marrow contusions and their association with injuries to the anterior cruciate ligament (ACL), medial collateral ligament (MCL), posterior cruciate ligament (PCL), lateral collateral ligament (LCL), medial meniscus, and lateral meniscus.
Data collected from the MRI scans were recorded in Microsoft Excel, and a simple descriptive analysis performed on GraphPad was employed to present the results of our study. Images were analysed by a fellowship-trained musculoskeletal radiologist with over 10 years of experience.
Results
Of the 150 patients, 92 were male, and 58 were female, with an average age of 16.9 (range 8–30 years). Fifty patients had oedema of the LTC and were included in our study.
Distinct patterns of bone marrow oedema within the LTC were observed, with the majority of 31 cases occurring in the posterior third, followed by the middle third (n = 13), and the anterior third (n = 6) [Table 2 and Figures 1–6].
Pattern of osseous oedema of lateral tibial condyle and concomitant injuries

Anterior third LTC oedema was associated with ACL injuries in two cases and MCL injuries in three cases. PCL injuries and concurrent medial meniscus injuries were less common, each observed in one case. Middle-third LTC oedema, observed in 13 cases, was predominantly linked to ACL injuries (n = 11), with three cases experiencing MCL injuries, two sustaining medial meniscus injuries, and another two presenting with lateral meniscus injuries. Posterior third oedema, found in the majority of cases, showed strong associations with ACL injuries (n = 28), MCL injuries in nine cases, and medial meniscus injuries in approximately four patients. None of the bone marrow oedema cases were linked to LCL injuries. All the results are displayed in Table 2.
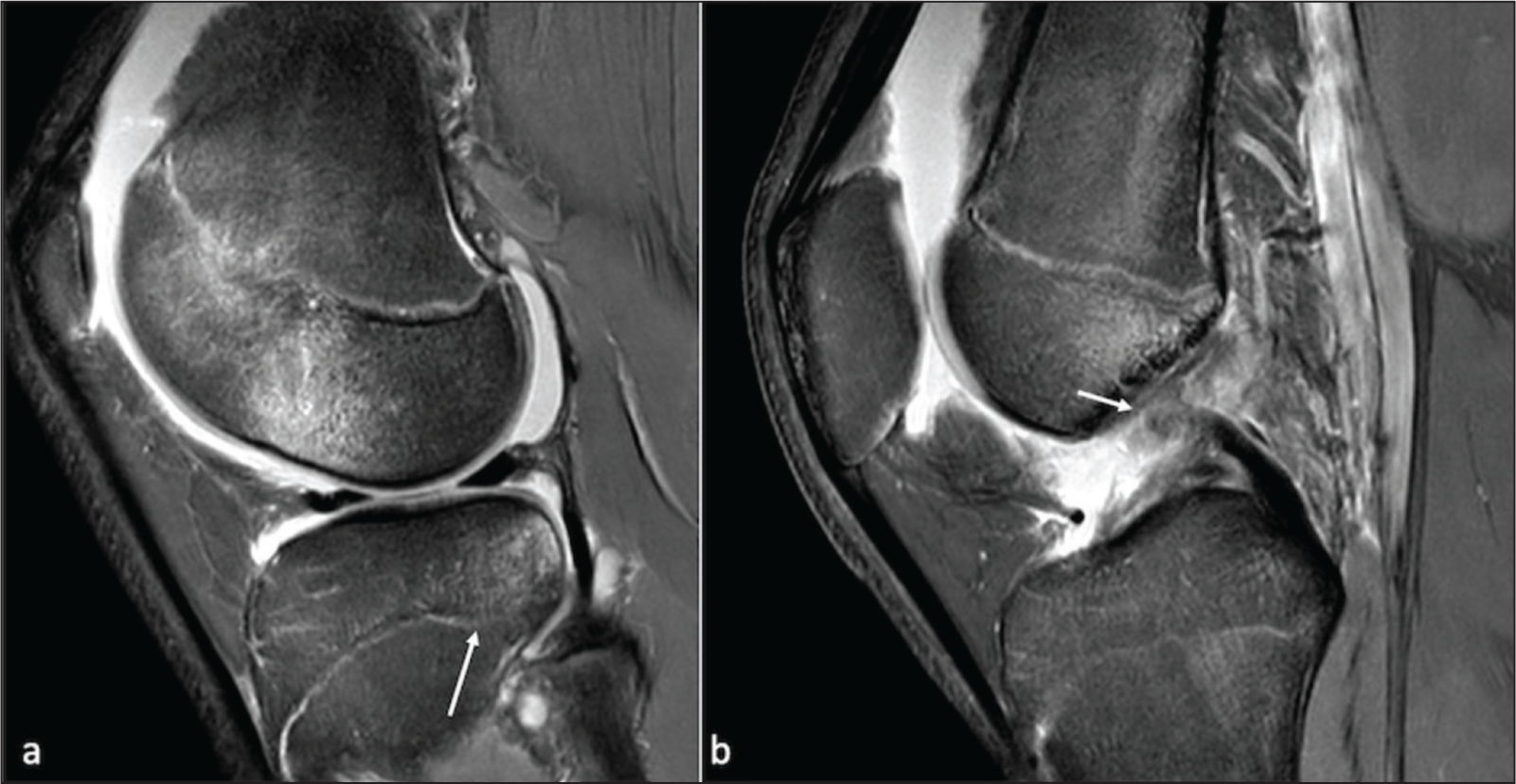
PDFS (proton density fat suppressed) sagittal (a and b) showing osseous oedema of posterior third of lateral tibial condyle (arrow, image a) with concomitant ACL tear (arrow, image b)
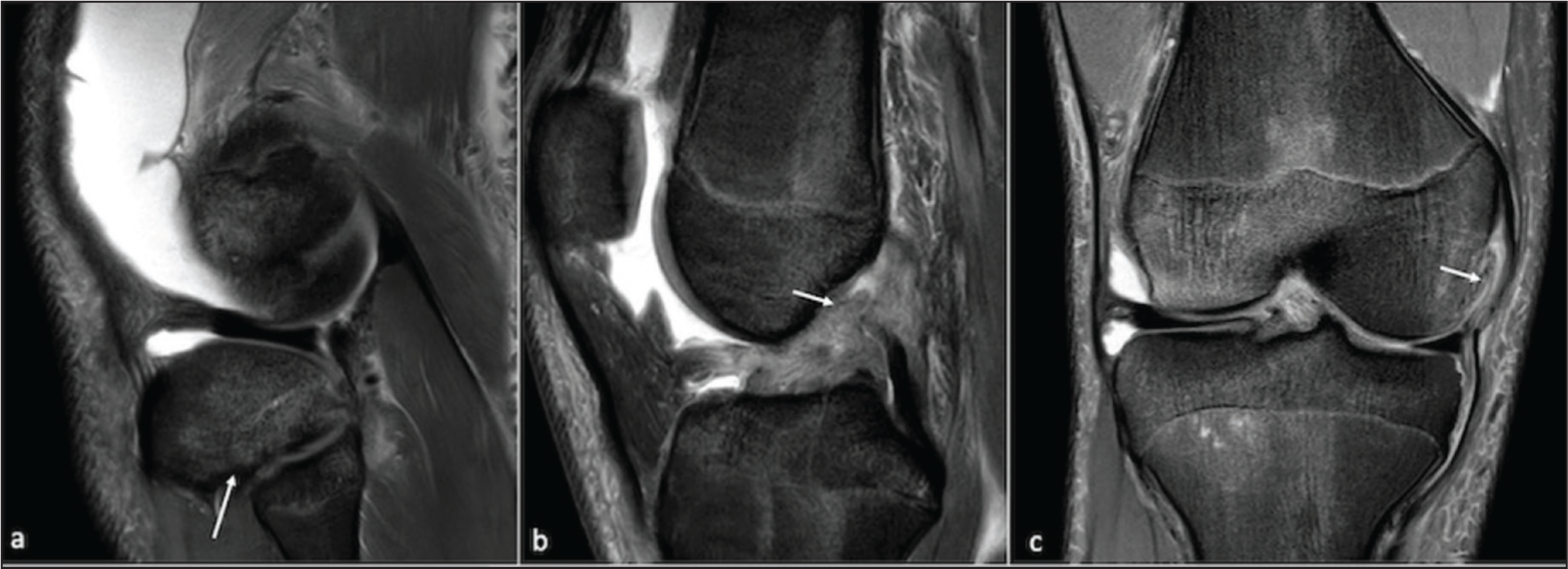
PDFS (proton density fat suppressed) sagittal (a and b) and coronal © showing osseous oedema of middle and posterior third of lateral tibial condyle (arrow, image a, b) with concomitant ACL tear (arrow, image b) and lax MCL with full-thickness tear of meniscofemoral ligament (arrow, image c)
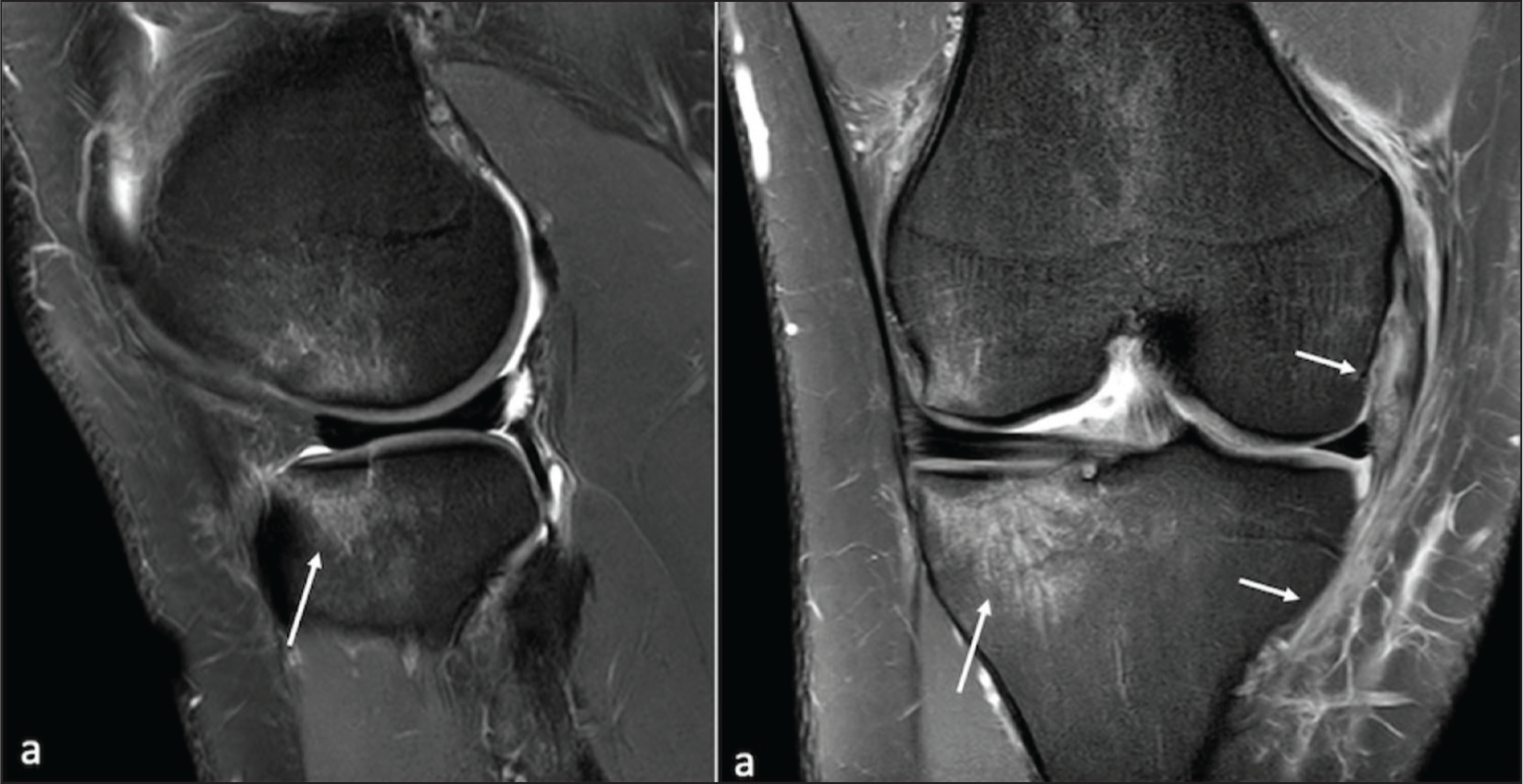
PDFS (proton density fat suppressed) sagittal (a) and coronal (b) showing osseous oedema of the anterior third of lateral tibial condyle (arrow, image a) with concomitant MCL tear (arrow, image b)
PDFS (proton density fat suppressed) sagittal (a and b) showing osseous oedema of the posterior third of the tibial condyle (arrow, image a) with concomitant ACL tear (arrow, image b)
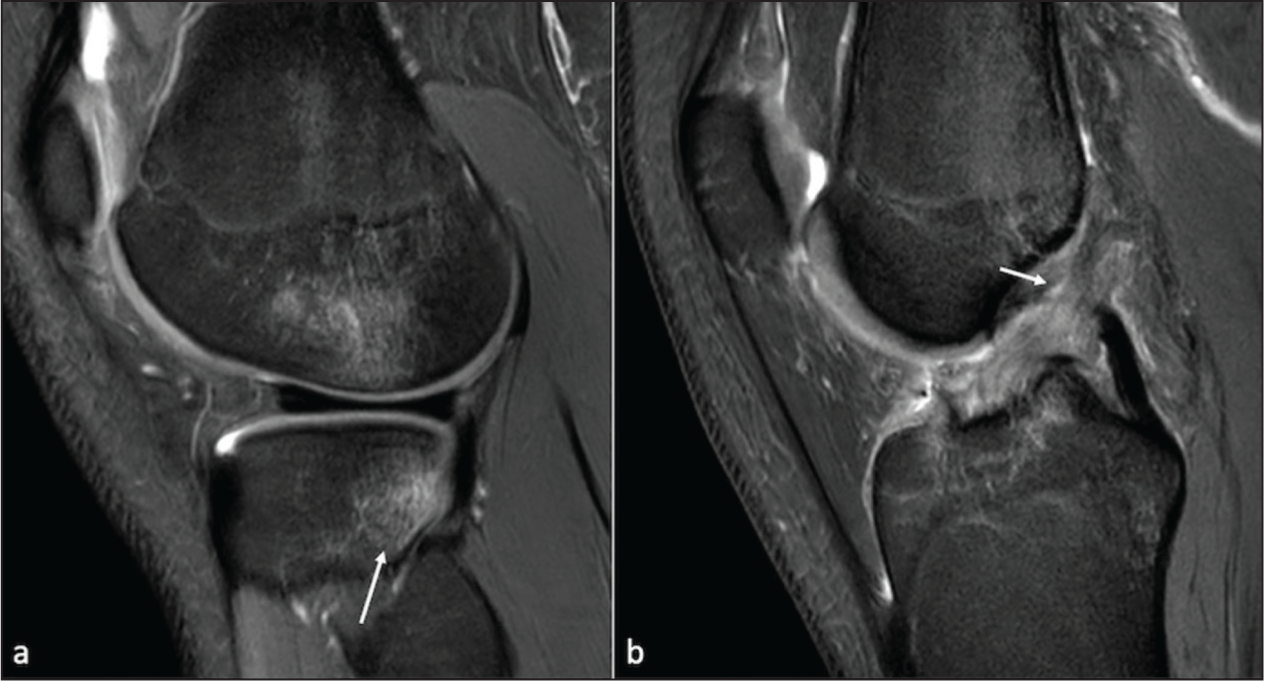
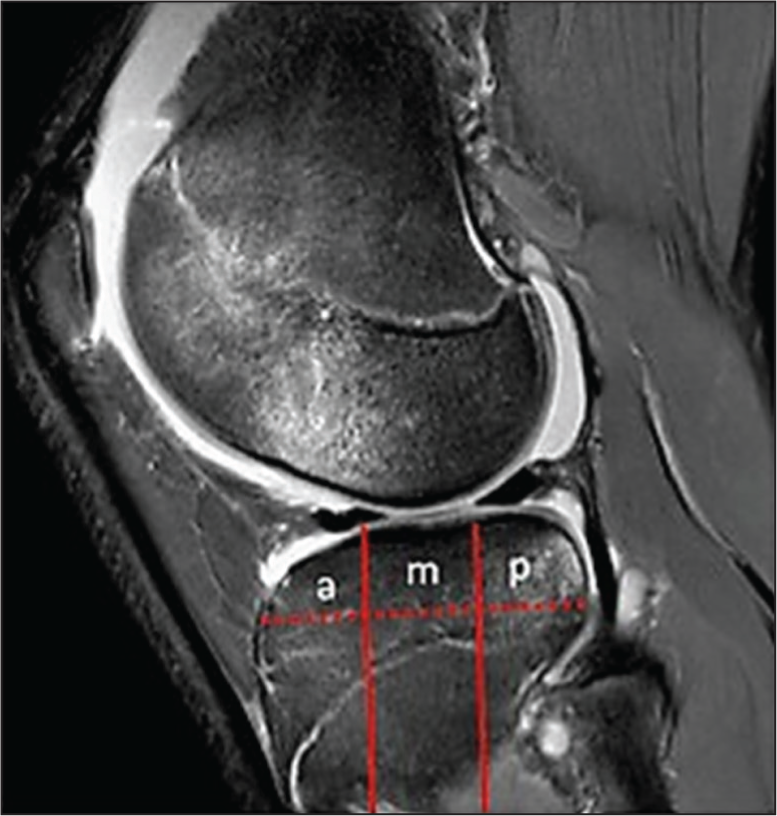
Image showing division of condyle into anterior (a), middle (m), and posterior (p) thirds
Middle one-third lateral tibial condylar oedema with lateral meniscal tear (arrow)

Discussion
Our study has provided valuable insights into the clinical significance of MRI-detected bone bruising patterns among patients with traumatic knee injuries. Our analysis of the distribution of bone marrow oedema within the LTC has revealed distinctive patterns that hold significant clinical implications. Notably, we found that anterior oedema often coexists with ACL and MCL injuries, while a minority of cases exhibit PCL or medial meniscus injuries. In contrast, middle oedema, which is more prevalent than anterior oedema, is predominantly linked to ACL injuries, with a lower incidence of MCL and meniscus injuries. Posterior oedema, on the other hand, demonstrates a strong association with ACL injuries (95%) and MCL injuries (38%). None of the cases of bone marrow oedema were found to be linked with LCL injuries.
Magnetic resonance (MR) imaging serves as an invaluable tool for evaluating soft-tissue injuries in the knee in the context of trauma.[4,6,14,15] However, the intricate nature of ligamentous knee injuries can lead to their frequent oversight in routine evaluations.[16,17] Among these injuries, bone marrow contusions are often detected.[5,11–13] The increased utilisation of MRI technology for acute knee injury assessments has heightened awareness of bone bruising as a unique clinical entity. The distribution of bone marrow oedema offers vital insights into concurrent soft-tissue injuries. These injuries may arise from various mechanisms, with five distinct contusion patterns described in the literature, including the pivot shift injury, dashboard injury, hyperextension injury, clip injury, and lateral patellar dislocation.[11]
Multiple studies have shown that over 80% of complete ACL ruptures are present with bone contusions evident on MRI.[16–19] ACL injuries are common injuries, often occurring following a pivot shift type mechanism with decelerational-rotational-valgus stresses applied to the knee in various states of flexion.[12,14] Subsequently, antero-tibial subluxation occurs in relation to the femur, leading to the impaction of the lateral femoral condyle against the posterolateral tibial plateau. The crosshatching indicates areas of bone contusion, with the degree of knee flexion at the time of injury influencing the precise location of the lateral femoral condyle contusion.[9,12,14] Similar to our study, McCauley et al. also found that 97% of bone bruises secondary to ACL ruptures were identified on the posterolateral tibial plateau,[14] suggesting that the visualisation of bone bruises on the posterolateral tibial plateau can effectively predict ACL tears with high specificity.
PCL injuries more commonly occur secondary to dashboard or hyperextension injuries to the knee.[20–22] Both injury mechanisms differ in their impacts on the knee joint. Dashboard injuries occur when external force is applied to the anterior aspect of the tibia while the knee is flexed, commonly happening in car accidents when the knee strikes the dashboard. They are associated with anterior tibial and patellar oedema and frequently lead to PCL disruption. In contrast, hyperextension injuries result from forcibly extending the knee beyond its normal range of motion.[21,22] This can occur through various activities, including direct anterior tibial force or forceful kicking motions. Hyperextension may cause a ‘kissing’ contusion pattern on the tibial plateau and femoral condyle, potentially leading to ACL and/or PCL injuries, as well as meniscal damage.[23] The distinction lies in the mechanisms, forces, and resultant injuries associated with these two types of knee trauma.
The MCL is the most frequently injured knee ligament in cases of knee trauma.[24,25] MCL injuries often co-occur with other ligamentous injuries, typically resulting from a valgus stress applied to the flexed knee within a range of 10–30 degrees. This type of injury leads to bone marrow oedema, most prominently in the lateral femoral condyle due to a direct impact, and a smaller area of oedema in the medial femoral condyle due to avulsive stress on the MCL.[26] To the best of our knowledge, no prior study has precisely determined the location of lateral tibial bone oedema occurrence in MCL injuries, which our study identifies as predominantly situated in the posterior third aspect of the LTC.
Bone contusions are distinguishable on T1-weighted images by displaying subchondral areas with ill-defined, decreased signal intensity compared to unaffected bone marrow. Conversely, on T2-weighted, proton density-weighted, and fat-suppressed images, these lesions appear as regions with increased signal intensity.[6,7,11,12] Presently, the pathophysiology of bone marrow oedema lacks specificity, posing challenges in distinguishing between various causes. However, bone contusions bear clinical significance, as they have been utilised to estimate the lifelong risk of osteoarthritis and are linked to knee pain subsequent to knee ligamentous injuries.[7,9] Despite this, a consensus regarding the natural progression of occult bone injuries sustained during knee trauma remains elusive.[9] Furthermore, recent literature emphasises the imperative need for additional research focused on improving the management and treatment of traumatic bone bruising, particularly in cases associated with concurrent soft-tissue injuries.[2,4,6–9,11,12]
Sanjay Yadav et al. conducted a study in 2022, out of 33 patients, 23 had bone bruises with predominant involvement of the lateral tibia (12 patients) and ACL injury.[27]
Our study had a few limitations. The number of lateral condyle oedema cases was relatively small and was retrospective. The location of osseous oedema of LTC (anterior, middle and posterior third) was relatively subjective, and no grading or scoring system was used.
Conclusion
Our study has provided valuable insights into the patterns of bone bruising associated with ligamentous injuries of the knee. By meticulously analysing the distribution of bone marrow oedema within the LTC, we have identified distinct patterns that offer clinicians a valuable diagnostic tool for identifying suspected knee injuries. These findings shed light on the clinical significance of MRI-detected bone bruising patterns in patients with traumatic knee injuries, emphasising the intricate relationships between different bone marrow oedema patterns and specific knee injuries. Our research has illuminated the differing mechanisms and injury associations among anterior, middle, and posterior oedema patterns, providing a comprehensive understanding of knee trauma and its associated pathologies. By recognising these patterns and their associations, clinicians can make more precise diagnoses and tailored treatment plans, ultimately improving the management and prognosis of patients with ligamentous knee injuries.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Local ethical committee approval was obtained.
Credit author statement
Conception and design, or acquisition of data, or analysis and interpretation of data: K J S S Raghu Teja, Botchu R.
Design, or acquisition of data, or analysis and interpretation of data: K J S S Raghu Teja, Papineni V R K, Botchu R.
Drafting the article or revising it critically for important intellectual content: K J S S Raghu Teja, Saad A, Botchu R.
Final approval of the version to be published: K J S S Raghu Teja, Saad A, Panchal H, Velicheti S, Iyengar K P, Beale D, Papineni V R K, Botchu R.
Data availability
Data available on request from the authors.
Use of artificial intelligence
No AI tools were used in the preparation of this manuscript.