
Abstract
Introduction
Considering the scarcity of specialist cessation service providers in resource-constrained Low- & middle-income countries (LMICs), the dental healthcare system can be used as an alternate source of cessation support. This study assessed dental healthcare providers’ current practices and perceptions about cessation support in teaching dental hospitals.
Methods
We assessed the cessation-related practices and perceptions of 348 dentists working in 10 teaching dental hospitals, using a cross-sectional design in the Khyber Pakhtunkhwa province of Pakistan. Participants were selected using simple random sampling technique and data were collected using a modified version of a previously used structured questionnaire, through face-to-face interviews by trained dentists. The Chi-squared test and logistic regression were used to determine associations between cessation support practices, cessation support perceptions, and their potential predictors.
Results
Overall, 13% of dentists provided cessation support, while 36% of participants practiced routine screening for tobacco use. 95% of dentists opined that cessation support should be provided in dental settings, with minimal counselling (5 As) being the preferred method. There was a strong association between dentists having formal training in cessation support and providing cessation support (aOR 6.58, 95% CI 1.95-22.11).
Conclusion
There is a lack of cessation training for DHCPs and a dearth of cessation services in the dental settings of Khyber Pakhtunkhwa, Pakistan. However, most DHCPs were willing to provide cessation services.
Implications
Cessation support falls behind compared to other MPOWER measures in Pakistan. As a resource-constrained LMIC, Pakistan can consider dental settings as a cost-efficient avenue for delivering cessation support-related services. Cessation services can be integrated into routine dental health care using a dental health workforce trained in cessation support. This untapped resource can help in curbing tobacco use in Pakistan and other similar contexts.
Introduction
Tobacco use is a significant cause of premature deaths and disability across the globe, with an estimated 7 million deaths annually attributed to its consumption. 1 Tobacco use is an established risk factor for different types of cancers, cardiovascular diseases, oral diseases, and has also been associated with adverse pregnancy outcomes. 2 The projected global prevalence for adult tobacco use is 19.8% by the year 2025, which compares to a 25% less prevalence than that in 2010. 3 This reduction can be attributed to the activities of the World Health Organization’s (WHO) Framework Convention for Tobacco Control (FCTC), a global treaty on tobacco control. 4 There is evidence of a lower prevalence of tobacco use in high-income countries (HICs) compared to low-& middle-income countries, 5 signifying more robust tobacco control measures like; tobacco quit lines, behavior counselling, online cessation programs, pharmacotherapy and other evidence based interventions, in HICs. 6 In Pakistan, an estimated 19.1% of adults use tobacco in some form, where the prevalence of smoked tobacco is 12.4%, while 7.7% of adults use smokeless tobacco products. Moreover, the prevalence of tobacco use is higher in males, and 45% of tobacco users smoke within 30 minutes of waking up, suggesting clear signs of severe addiction to nicotine. 7 Being a signatory, Pakistan has an obligation to abide by the tobacco control guidelines of WHOs FCTC including provision of cessation support services to tobacco users.
The WHO FCTC comprises 38 articles, of which articles 6-14 are measures for reduction in demand and articles 15-17 address the supply of tobacco products. Article 14 specifically focuses on the establishment of cessation services for demand reduction. 8 These include toll-free quit lines, behavioral tobacco cessation interventions and pharmacotherapy. 9 Toll-free quit lines provide cessation services to smokers who are willing to quit; after initial assessment for their readiness to quit, phone-based cessation sessions are offered to smokers. 10 Behavioral interventions include brief advice (5 As approach) for quitting tobacco use at primary care facilities, 11 whereas as effective pharmacotherapy includes Nicotine replacement therapy, and cessation medication like Bupropion and varenicline. 12 Monitor tobacco use & prevention policies protect people from tobacco smoke, offer help to quit tobacco use, warn about dangers of tobacco, enforce bans on tobacco advertising promotion and sponsorship, raise taxes on tobacco (MPOWER), a package for demand reduction intervention, was introduced by the WHO in 2008 to assist member states in implementing FCTC measures. 13 Pakistan, being a signatory to WHO FCTC since 2005, specifically lags behind in the “Offering help to quit tobacco use” segment of the MPOWER package. 14
In resource-constrained LMICs, a task-shifting approach can help in delivering cessation services through the existing health service system. Task shifting is an approach adopted in various resource-constrained settings to improve access to a highly skilled workforce for the delivery of specific health services. 15 Keeping in view the scarcity of skilled cessation counsellors in Pakistan, 16 task shifting approach can help in improving access of tobacco users to cessation services. If trained in cessation service provision, dentists and the dental healthcare system can be used as an alternative to specialist cessation counsellors. The dental setting lends itself as an appropriate option for the provision of tobacco cessation counselling for multiple reasons. 2 The routine dental sessions’ longer duration and increased frequency provide a window for the dental team to counsel tobacco user patients. 17 Additionally, the health effects of tobacco use are first expressed in the oral cavity, making it easier for dentists to convince the patient of the cause-and-effect relationship between tobacco and their health.
In Pakistan, there are an estimated 29000 licensed dentists practicing in Teaching dental hospitals (TDH) or providing dental health services in Private dental practices. 18 Considering the enormity of the dental healthcare workforce, the dental setting can be an efficient option19,20 to provide effective cessation services to tobacco user dental patients using the task-shifting approach. A recent study from Pakistan that assessed the feasibility of dental settings as an alternate source for cessation service provision asserted the need for dentists to implement tobacco cessation service in a low-resource setting. 20 However, there is a gap in the literature regarding the current extent of the provision of cessation services by dentists in Pakistan. In Pakistan, a large proportion of the population seek dental care through teaching dental hospitals (TDH); the primary healthcare setups are mostly deficient in specialized dental services due to resource constraints. Moreover, the TDH are not only the centers for all the dental healthcare provision services but also for the training and teaching for dental practitioners. Considering dental settings as an alternate source for tobacco cessation service provision, it is essential to understand dentists’ perceptions about executing this role. Our study aimed to assess the current practices and perceptions of dentists about tobacco cessation service in the dental health services in Pakistan.
Methods
This study adopted a cross-sectional design to assess dental healthcare providers’ current practices and perceptions of tobacco cessation services. This survey was conducted in all the Teaching Dental Hospitals (TDH) registered with Pakistan Medical & Dental Council (PM&DC). The Deans of all the current TDH (N = 11) were approached with letters of permission for data collection. Ethical approval was acquired from Ethical Review Board of Khyber Medical University. After getting permission for data collection, we secured lists of dental healthcare providers working as faculty members or as Trainee Medical Officers (TMO) in the respective teaching dental hospitals. Assuming a population size of 2000, hypothesized % frequency of outcome factor in the population (p): 50%+/−5, confidence limits as % of 100 (absolute +/− %) (d): 5%, and a Confidence level (%) 95%, a sample size of 323 dentists was calculated. Sample size was increased to 355 for compensation of 10% non-response rate. We constructed a sampling frame from the lists of dental health providers in the 11 teaching dental hospitals and included 348 dental health workers following a simple random sampling method. Following simple random sampling, DHCPs from the list were included and subsequently contacted through telephone. Participants who did not respond were contacted again, following which non responders were excluded.
Prior to data collection, a detailed participant information sheet was shared, and written informed consent was secured from all the participants. All practicing dental healthcare workers possessing a valid PM&DC license to practice and performing their roles as faculty or as TMOs from the clinical departments and dental public health were eligible for inclusion in the survey. House officers, dental students and dental auxiliary staff were excluded.
We adopted a previously used questionnaire (appendix I) from a study in Canada. 21 Initially we conducted the face validity of the questionnaire with tobacco cessation experts and researchers, following which the questionnaire was pilot-tested. After pilot testing a final session of face validity for agreement on the content of the instrument was conducted with the same experts. The questionnaire had 3 sections. The first section (15 items) consisted of questions about the practices of cessation services of the dental health care providers (DHCP). The second section (04 items) was about the practices of DHCPs in their private dental practices, and the third section (11 items) had questions about the perceptions of DHCPs about provision of cessation programs in the future. Data was collected by a team of 4 dentists holding Bachelor’s in Dental Surgery (BDS) degrees and with additional postgraduate qualifications. The data collection team was extensively trained for familiarization with the content and the administration of the face-to-face structured data collection instrument. Data about the type of hospital sector, type of cadre of the DHCPs, age, gender of the DHCPs, years of clinical experience of the DHCPs, and private dental practice status of the DHCPs were also collected using the same data collection instrument. Data about the perceptions of DHCPs regarding provision of cessation support, the type of tobacco user dental patient (all patients, patients with a specific disease), the preferred method of cessation support, and the venue for providing cessation support services within the TDH were also collected.
Data Analysis
Data were analyzed using STATA version 14 (Stata Corp). Continuous variables like age and years of experience were transformed into categorical variables. The participants’ clinical experience was categorized into 3 groups (<5 years, 5 to 10 years, and 10.1 to 35 years) based on promotion criteria set by the Pakistan Medical and Dental Council. The chi-square test was used to assess correlations between tobacco use history assessment, provision of cessation service in teaching dental hospitals, and categorical variables including gender of provider, type of hospitals, years of experience, private dental practice, cessation training status, and type of cadre of participants. Likewise, the Chi-Square test was used to assess the correlation between perceptions of the provision of cessation services and the above-mentioned variables.
Logistic regression analysis was done to determine the association between ‘provision of cessation service’ and ‘perceptions for provision of cessation services’, and potential predictors including gender of provider, type of hospital, years of clinical experience, private dental practice, cessation training status, and type of cadre of participants. A 95% confidence interval with a P < 0.05 was considered significant.
Results
Response Rate
One of the total Teaching dental hospitals (n = 11) refused to participate in the survey. More than half of the TDH (56%) were primarily from the public sector, and the overall response rate of the participants was 98%. More than half of the study participants (62%) also had a private dental practice.
Demographics
The mean age of the participants was 35.6 (7.1) years, and there was a slight male preponderance (53.2%). The majority of the participants had up to 5 years (40.8%) of clinical experience, followed by “5 to 10” years (34.2%), while 25% had between “10 to 35” years of experience. Most participants held postgraduate qualifications in their respective clinical specialties (56.6%), and almost two-thirds (65.8%) of the study participants were faculty members.
Tobacco-use Screening
Distribution of Obtaining Tobacco History Among the Study Participants

aSignificant. Overall means irrespective of categories.
Tobacco Cessation Service Provision
Distribution of Tobacco Cessation Service Provision Among the Study Participants

aSignificant. Overall means irrespective of categories.
Perception of Tobacco Cessation Service Provision
Distribution of the Perception of Tobacco Cessation Service Provision Among the Study Participants
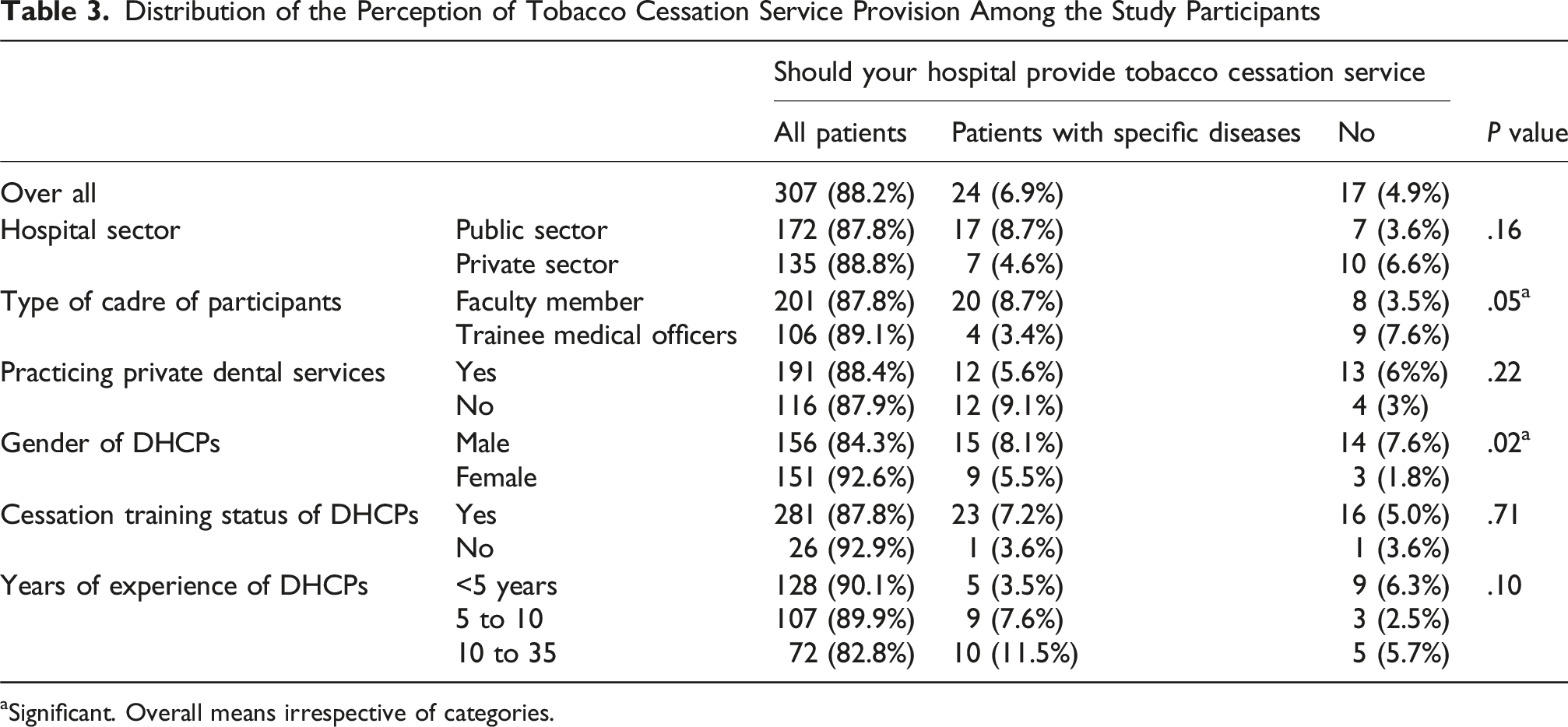
aSignificant. Overall means irrespective of categories.
Perceptions About the Preferred Type of Cessation Support
Most (92%) of TDH preferred minimal counselling (5 As method) for cessation support, irrespective of the type of patients and clinical department in the hospital. This was followed by self-help material (87.9%), intensive counselling (83.6%), referral to external cessation support services (77.9%), NRTs (74.7%), and prescription medications (74.2%) in descending order of preference, respectively. For ‘patients with a specific disease’, the preferred venue for all the types of cessation support was the relevant clinical specialty department.
Predictors of DHCPs Providing Cessation Support
Association Between Tobacco Cessation Service Provision and its Predictors

The Reference category for all dependent variables is not aware. aOR are adjusted for all other independent variables in the respective model.
aStatistically significant. aOR adjusted odds; ref, reference.
Predictors of Perceptions of DHCPs for Providing Cessation Support
Association Between the Perception of Tobacco Cessation Service Provision and its Predictors

The Reference category for all dependent variables is not aware. aOR are adjusted for all other independent variables in the respective model.
aStatistically significant. aOR adjusted odds; ref, reference.
Discussion
Our study highlights the lack of tobacco cessation service provision through the dental healthcare system in Pakistan. We also report a very low percentage of tobacco use screening by DHCPs and a very small percentage of DHCPS (8%) formally trained in cessation support-related skills. However, a large majority of the DHCPs, if provided the opportunity, were willing to deliver cessation support through the dental settings, and an overwhelming majority favored brief advice (5 As method) as the preferred cessation method.
Routine screening of patient’s tobacco use is an essential first step for effective tobacco cessation services. Asking patients about their tobacco use helps healthcare workers to understand their behavior, the extent of their addiction, and the intensity of their tobacco use, and devise a cessation plan accordingly. It also helps discern between tobacco users and non-users, thus channeling resources and time for more efficient service provision to those who use tobacco. We observed a very low practice of routine tobacco use history assessment in the dental settings. Literature reports mixed evidence regarding patients’ tobacco use history-taking by DHCPs. Studies from similar LMIC contexts to Pakistan have also reported a lack of tobacco history-taking during visits to dental clinics.22,23 Evidence from HICs, however, is in contrast to our findings, with a high preponderance of tobacco screening during dental appointments 24 These differences can be explained by differences in the adoption of robust cessation services in HICs and the lack of resources in LMICs.
Evidence suggests that cessation support given by healthcare professionals increases the likelihood of successful quit attempts by tobacco users.. 25 We report a low cessation support provision through the dental settings, which is in contrast to the advisory of the WHO, that recommends the use of healthcare services for provision of cessation support including the dental healthcare services.26,27 Low cessation support in healthcare settings can be attributed to the shortage of resources, including the infrastructure needed to provide cessation support to tobacco users. 28 Lack of motivation of healthcare professionals due to workload, time constraints, incentives and low confidence in providing cessation support due to lack of training are amongst the known barriers to cessation support provision mentioned.20,29,30 Our findings are in agreement with available literature regarding the low practices of healthcare professionals in providing cessation support in LMIC context.14,31
Health professionals trained in tobacco cessation methods are more likely to provide cessation advice and offer self-help material and referrals to specialized cessation services compared to their non-trained counterparts. 32 The low percentage of tobacco cessation-trained DHCPs in our study is similar to the findings from other LMICs, where the lack of training has been highlighted as a significant barrier to cessation service provision. 33 This lack of cessation training can be attributed to the scarcity of resources, motivation of DHCPs, and cessation training not being an integral part of health professional’s curricula.34,35 There is a substantial body of evidence that healthcare workers trained in cessation services positively affect their competency in offering help to tobacco users who want to quit 36 Among the predictors for cessation support practice, DHCPs trained in cessation support were 6 times more likely to engage in cessation support activities compared to their non-trained counterparts. Similar findings have been reported from elsewhere, where positive attitudes towards tobacco cessation and the use of cessation guidelines in assisting tobacco users quit their tobacco habit were found in the trained dental workforce.. 37
We found that an overwhelming majority of DHCPs were in favor of cessation support provision through the dental health care system. Our findings are consistent with available literature about positive attitudes of dentists towards their role in the provision of cessation support.38,39 A study from Finland reported a positive attitude of dentists towards cessation support despite low practices of delivering the service. 40 The 5 As approach tobacco cessation was the most favored approach in our sample. Brief advice like the 5 As approach has been reported to be an effective and cost-efficient intervention for smoking cessation. 41 Our findings suggest a six-fold higher likelihood of positive perceptions of DHCP-delivered cessation support among the female respondents compared to males about the provision of cessation services. This preponderance can be explained by the relatively lower prevalence of tobacco use among females globally, 7 where evidence suggests that the likelihood of a health care provider engaging in cessation activities is driven by, among other factors, their tobacco use status. 42 Our findings are in line with an Iranian study exploring the familiarity of dentists with a cessation program (5-As approach), reporting female dentists were more likely than their male counterparts to engage in cessation activities. 43
We observed poor integration of cessation support through the dental health care system in Pakistan, which is not in accordance with the guidance of the WHO FCTC. Considering the vital role of DHCPs in identifying, diagnosing and management of oral pathologies related to tobacco use, integrating cessation support through the dental health care system can be the way forward to reduce the burden of tobacco use, and increase access of tobacco users to cessation support services.
Given the lack of literature on TCS within the Pakistani context, our study is the first to provide evidence of the state of tobacco cessation in a dental healthcare setting. This study was adequately powered with representation from 95% of the dental health care hospitals in KPK province, Islamic Republic of Pakistan, and a very high response rate. However, our study adopted a cross-sectional design, which has some inherent limitations, including the inability to establish causality and temporality and cannot provide long-term insights. A specific limitation of our study is that our findings were self-reported, and we did not observe the actual practices of the DHCPs at their workplace. Some of the findings may have been a function of the distribution of the research participants, for example gender and years of clinical experience, and have had a play on the reported findings. The confidence intervals around some of the estimates are wide, likely being a function of the low numbers of DHCPs providing cessation support. Additionally, our study could have included dental auxiliary staff for a more holistic view of cessation services offered in these dental settings, given their essential role in a dental team. Our study did not include DHCPs practicing in non-teaching hospitals and clinics in rural areas, this should also be considered as a limitation of this study. Although we have conducted face validity during adaptation of the instrument, we did not conduct formal content validity which is a limitation of our study. However, the content in general is relevant to various dental settings and has been used extensively in different contexts. Another limitation of our study is that we did not formally assess inter and intra examiner variability. In order to minimize such variability, we have conducted rigorous training of the data collection team for calibration on the structured data collection tool and conducted pilot testing prior to the main data collection phase.
Conclusion
This study highlights a general lack of tobacco cessation support services and training in Pakistan, but it also touches up on the willingness of DHCPs to provide cessation support providing a window of opportunity that bodes well for interventions like this. To implement such intervention, formal training of tobacco cessation can be a good avenue for strengthening tobacco cessation services.
Footnotes
Acknowledgements
This study is part of a doctoral project titled “Tobacco Cessation in the Dental Settings in Khyber Pakhtunkhwa: the Current State of Practice and Intervention Adaptation”. It is partially funded by the Office of Research Innovation and Commercialization, Khyber Medical University, Peshawar.
Author Contributions
BA, ZoK, WS, contributed to conception of the research BA, AN, AS, AR, contributed to acquisition of data BA, AN, ZKH, WS, contributed to analysis of data BA, ZoK, FA, ZKH, AN, contributed to interpretation, initial draft and final approval of the manuscript for publishing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is partially funded by the Office of Research & Innovation, Khyber Medical University Peshawar (2023/19/43/22). The authors declare no conflict of interest.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The study is part of the doctoral thesis, and the doctoral research scholar secures the data set. After the thesis has been submitted and defended successfully, the data set will be available on a secured server at Khyber Medical University and will be available on request.