
Abstract
Background
Secondhand smoke (SHS) exposure remains a critical public health concern, especially for adolescents, who are more susceptible to its harmful effects and may initiate smoking as a result. SHS, comprising both mainstream and sidestream smoke, contains over 7000 chemicals, many of which are carcinogenic. Adolescents exposed to SHS are more likely to experiment with smoking due to environmental influences, peer pressure, and familial smoking behavior.
Objective
This study aims to examine the relationship between SHS exposure and smoking attitudes and behaviors among adolescents aged 13-15 in the Gaza Strip, where SHS exposure and tobacco use remain prevalent.
Methods
Data were obtained from the 2019 Global Youth Tobacco Survey (GYTS), a cross-sectional, school-based survey targeting students in Gaza. The study employed a two-stage cluster sampling design to ensure a representative sample. SHS exposure was assessed in multiple contexts, including home, public enclosed spaces, and outdoor areas. Smoking attitudes, initiation behaviors, and demographic variables were also analyzed using descriptive statistics, Chi-square tests, and multivariable logistic regression to identify predictors of smoking behaviors.
Results
Of the 1536 adolescents surveyed, 62.3% reported SHS exposure at home, and 53.9% reported exposure in enclosed public spaces. Adolescents exposed to SHS were significantly more likely to experiment with smoking, with curiosity (62.2%) and peer influence being key motivators. Additionally, SHS exposure in both indoor and outdoor environments was associated with a higher likelihood of shisha experimentation. Females reported higher SHS exposure rates than males across all environments (P < .001).
Conclusion
SHS exposure significantly increases the risk of smoking initiation among adolescents in the Gaza Strip. These findings emphasize the need for targeted public health interventions, including stricter smoke-free legislation, parental education, and awareness campaigns aimed at reducing SHS exposure and preventing smoking uptake in youth.
Keywords
Introduction
Involuntary smoking, passive smoking, or environmental tobacco smoke (ETS) are all synonyms of secondhand smoking (SHS). 1 SHS is a combination of mainstream smoke (exhaled by the smoker) and sidestream smoke (emitted from the smoldering tip of a cigarette). Research has determined that SHS contains more than 7000 chemicals, with at least 69 being recognized as carcinogens, such as formaldehyde, benzene, and arsenic. These carcinogens, which have been associated with a variety of cancers and other severe health conditions, contribute to the health dangers associated with exposure to SHS. SHS exposure poses significant health risks, particularly for non-smokers, youths, pregnant women, and children. 2 It remains a global health problem, with 40% of children and 34% of non-smoking adults exposed. 3
There is no safe level of exposure to SHS; even brief exposure can cause immediate harm. Exposure to SHS induces immediate physiological responses. Approximately 2 500 000 individuals who did not smoke have passed away as a result of health complications resulting from exposure to SHS since 1964. 4 Research further indicates that SHS exposure in children, youths, and others has both immediate and long-term effects. Immediate effects include irritation of the eyes, nose, throat, and lungs, headaches, nausea, and dizziness. Exposure to SHS in children results in respiratory illnesses, chronic respiratory symptoms (such as asthma), ear infections and reduced lung function. Long-term exposure leads to severe conditions such as lung cancer, coronary heart disease, and cardiac death. The American Heart Association strongly warns against SHS exposure and calls for stricter smoke-free legislation to prevent SHS exposure among children and youth. 5
The World Health Organization is increasingly focused on reducing smoking rates and SHS exposure. Their efforts also aim to enhance public knowledge about the dangers of smoking, including respiratory and cardiovascular risks. 2 However, despite extensive campaigns and active social media efforts to explain the harmful effects of SHS, smoking remains a major public health issue, especially in low-income and densely populated areas where smoking bans are often poorly enforced. 5
Adolescence often marks the beginning of smoking experimentation, with smoking rates rising significantly during this period. “For instance, in various Western countries, smoking prevalence among 13-year-olds ranges from 3.5% to 12.5%, and this rate increases to between 17% and 24.5% by age 15”. 6 Early exposure to SHS is a key factor in increasing susceptibility to smoking initiation.3,7 Adolescents in smoking households are more likely to be exposed to SHS and start smoking themselves than those from nonsmoking homes. 8 Adolescents exposed to SHS, such as through parental smoking, are at a significantly higher risk of initiating smoking themselves. 7 Both inattentiveness and parental smoking can increase the risk of adolescent smoking initiation to 38%, compared to 5% without these risk factors. 9 Adolescents represent a critical age group at high risk of starting to smoke, requiring special attention from health policymakers and decision-makers. 10 Identifying smokers early in this group, along with the factors influencing smoking behavior, is key to reducing or preventing cigarette use. 11
Existing literature further emphasizes the behavioral impacts of SHS exposure. For instance, data from the 2002 Youth Lifestyle Study (YLS) in New Zealand revealed that frequent SHS exposure at home significantly increased the likelihood of becoming a daily smoker. 12 Similarly, a systematic review of 35 studies confirmed a strong association between SHS exposure and increased smoking susceptibility, nicotine dependence, and challenges in cessation efforts. 3 In Japan, a dose-response relationship between SHS exposure and smoking initiation was identified, with heightened risks as exposure levels increased. 13 These findings highlight the broader implications of SHS on adolescents’ smoking behaviors.
The role of familial and social influences in smoking initiation is well documented. A meta-analysis of 58 studies found that parental and sibling smoking strongly influenced smoking uptake among adolescents, with a pronounced effect when mothers smoked. 14 Additionally, SHS exposure was shown to mediate the link between parental smoking and children’s smoking initiation, as observed in a Hong Kong study, where each additional day of SHS exposure at home increased the risk of smoking initiation by 16%. 8 These findings underline the intergenerational nature of smoking behaviors.
This familial influence extends beyond just parental smoking. Research has shown that children raised in households where smoking is prevalent often develop a perception that smoking is socially acceptable. Children also learn behaviors by observing and imitating their parents. Numerous studies have supported the idea that parental smoking behaviors serve as a model for children, shaping their attitudes towards smoking. This normalization of smoking can reduce the perceived risks associated with smoking, making children more open to experimenting with cigarettes or adopting a more positive attitude towards smoking in general. 12
The normalization effect is further reinforced by environmental factors such as the presence of smoking tools (eg, ashtrays, cigarette packs) and frequent exposure to smoking in social settings and the usual environment. These environmental signs can influence children’s attitudes by making smoking appear as a routine, unremarkable, normal activity. 3 Additionally, the addictive nature of nicotine absorbed through SHS can lead to the persistence of smoking behaviors, making it more difficult for adolescents to quit once they have started. 15 SHS exposure also decreases adolescents’ ability to resist smoking, as repeated exposure lowers their defenses against peer pressure and reduces self-refusal.
Attitudes and beliefs shape adolescents smoking behavior. Supporting this, a study found that experimental smokers were more likely than nonsmokers to believe that smoking offers benefits, such as helping people relax, controlling weight, and making them feel more comfortable in social situations. Experimenters were also less likely to express negative views about being around smokers and tended to believe they could quit smoking anytime they wanted. 16 According to Social Cognitive Theory (SCT), the likelihood of smoking is influenced by outcome expectations and self-efficacy. 17 Adolescents who smoke may have multiple positive outcome expectations, such as social confidence, 18 stress reduction, 19 and attractiveness, 20 mistakenly believing that smoking provides these benefits. 21 The literature also emphasizes that positive attitudes toward tobacco control policies can contribute to their effectiveness in altering smoking-related behaviors.22,23 Conversely, negative smoking outcome expectations, such as the fear of health consequences, can motivate individuals to quit. However, the complexity of these attitudes requires addressing both positive and negative expectations in smoking cessation efforts. 24
Research indicates that while SHS exposure increases the likelihood of smoking initiation, individuals who are aware of its harmful effects are less likely to be influenced by exposure. For example, over 80% of respondents in a study reported recent SHS exposure, but those who recognized the dangers of SHS were less likely to start smoking, and smokers who acknowledged the risks were more motivated to quit. 25 This highlights how attitudes about SHS can act as a protective factor, counteracting the effects of exposure. Furthermore, studies from Ethiopia show that knowledge of SHS risks can strengthen anti-smoking attitudes, even in households where smoking is common, suggesting that beliefs can diminish the impact of SHS exposure. 26 Interestingly, adolescents from non-smoking households, who are less exposed to SHS, are more likely to support smoking bans, reinforcing how reduced exposure fosters stronger opposition to smoking. 27 On a societal scale, smoke-free policies magnify these effects, reducing SHS exposure while promoting negative attitudes toward smoking, creating a feedback loop that strengthens public opposition to tobacco use. 28 These findings underscore the complex and synergistic relationship between exposure and attitudes in driving smoking-related behaviors.
In Palestine, gradients in risk for youth smoking increased in association with the number of risk behaviors reported, which increases their likelihood of smoking. 29 Males start smoking at younger ages (74.4% by 18 years). Adolescents who smoke are more likely to hold lower anti-smoking beliefs. Despite some willingness to quit, challenges such as mood changes and lack of self-control persist, highlighting the need for strategies that address both smoking initiation and SHS exposure among youth. 30 Understanding the dynamics of smoking is crucial for developing effective interventions aimed at reducing smoking initiation among children, particularly in families where smoking is prevalent. This research aimed to explore the complex interplay between parental smoking, SHS and children’s attitudes, with a focus on identifying strategies to break the intergenerational cycle of smoking
The aim of the study is to assess the relationship between secondhand smoke (SHS) exposure, smoking behaviors, and demographic variables among adolescents in the Gaza Strip, as well as to evaluate adolescents’ attitudes toward smoking based on their responses to relevant statements from the 2019 Global Youth Tobacco Survey (GYTS) Conducting this research utilizing Gaza Strip GYTS is particularly important, as the region’s unique socio-economic, political, and cultural influences may impact SHS exposure and smoking behavior. Understanding these factors is crucial for developing effective prevention strategies that are tailored to the specific needs of adolescents in this region.
Methodology
Study Design and Population
This study utilized data from the 2019 Global Youth Tobacco Survey (GYTS), a cross-sectional, school-based survey developed to monitor tobacco use, tobacco-related knowledge, and global adolescent attitudes. The GYTS uses a standardized protocol to ensure data comparability across different countries. The survey was conducted in the Gaza Strip, targeting adolescents aged 13-15 enrolled in public and private schools. These age groups were selected because they represent a critical developmental period where behaviors and attitudes toward smoking are often formed and solidified.
The GYTS employed a two-stage cluster sampling design to obtain a nationally representative sample of students. In the first stage, schools were selected with a probability proportional to their enrollment size. In the second stage, classes within selected schools were randomly chosen, and all students in the selected classes were eligible to participate. The Inclusion Criteria included students aged 13-15 years, grades 7 through 10 (or equivalent), typically representing the middle or early high school years in the governmental and private schools, and informed consent. We excluded youth outside this age group, those not enrolled in school, those outside the formal education system, and those not representative of the broader adolescent population in the country (for example, those in special education or residential institutions).
The sample size for the GYTS was determined using a standardized methodology designed to ensure national representativeness and reliable estimates. The sample size calculation was based on the desired precision for key indicators, typically set at a 95% confidence level with a margin of error of ±3%. The formula used incorporates an assumed proportion of 50% (the most conservative estimate), and adjustments are made for the design effect, which accounts for the clustering of students within schools (typically ranging from 1.5 to 2.0). The Center of Communicable Disease (CDC) CDC processed the raw data using standard GYTS procedures. A weighting factor was applied to reflect the likelihood of sampling each student and to reduce bias by compensating for differing patterns of non-response. Also, a statistical analysis of correlated data was used to compute 95% confidence intervals. This weighting process ensures the results are representative of the target population and enhances the reliability and validity of the findings. 31 The initial sample size was then increased to account for non-response, such as absenteeism or refusal to participate, ensuring the final sample size is large enough to produce reliable estimates. These calculations ensure that the sample is sufficiently powered to analyze tobacco use prevalence, SHS, and attitudes toward smoking among adolescents. Theresponse rate was 88.1%. A total of 1536 eligible students in grades 7-10 completed the survey, of which 1115 were aged 1315 years. Data are reported for students aged 13-15 years 32 Participation in the survey was voluntary, and informed consent was obtained from both students and their guardians. Ethical approval for this study was obtained from the Institutional Review Board (IRB) of the College of Medicine at Hebron University, with the approval reference number ER.CM.11\2024.
Data Collection
Data collection was carried out using a standardized core questionnaire from the GYTS. This questionnaire is globally recognized for its reliability in capturing key information related to tobacco use among youth. The core GYTS questionnaire was enhanced with additional questions explicitly tailored to the Gaza Strip to ensure the data collected was relevant to the local context. 33 These modifications were aimed at capturing region-specific factors influencing tobacco use and exposure to SHS.
This study addressed various aspects of tobacco use, including smoking in different forms (cigarettes, smokeless tobacco, hand-rolled cigarettes), age at first tried a cigarette, reasons for starting to smoking, frequency and intensity of smoking, quitting attempt, exposure to SHS, participants’ attitudes toward tobacco use. The primary outcome variable is the adolescents’ smoking attitudes and behaviors, which encompass their smoking status, frequency of smoking, and attitudes toward smoking. The leading independent variable of interest is exposure to SHS, examined in various contexts, such as at home, in enclosed public spaces, and in outdoor public areas over the past seven days.
Environmental and Social Influences such as exposure to SHS in various environments, parental smoking behavior, and the smoking behaviors of closest friends are used as SHS variables. Participants’ perceptions of harm from tobacco smoke, their opinions on banning smoking in public places (both enclosed and outdoor), beliefs about the difficulty of quitting once started, perceptions of smoking’s social acceptability, and their agreement with statements like “I think I might enjoy smoking a cigarette,” were used to assess the attitudes and beliefs regarding smoking. Sociodemographic Variables such as age, sex, and weekly spending money were also used as these variables are deemed essential for understanding how smoking behaviors and attitudes may vary across different segments of the youth population.
The measurement tools employed in this study were rigorously assessed to ensure clarity and appropriateness for the target population. Variables were categorized according to their respective scales of measurement. Dichotomous nominal variables included binary responses, such as gender (boy/girl) and behavioral indicators (eg, “Have you ever tried smoking cigarettes?” with responses of yes or no). Ordinal variables, which provide a ranked order without consistent intervals, encompassed items such as age categories (“12 years or younger” to “15 years or older”) and perceptions of harm related to smoking (“Definitely not” to “Definitely yes”). Nominal variables without inherent order, such as reasons for starting smoking (eg, curiosity, peer pressure, model influence), were also included. Continuous or interval-scale measurements were not applicable, given the categorical nature of the survey questions (Supplemental Material).
Students completed the survey themselves during school hours, and their responses were recorded on scannable paper-based forms. This method was chosen to maintain the participants’ anonymity and confidentiality, which is crucial in obtaining honest and accurate responses, especially on sensitive topics like smoking.
Data Analysis
The GYTS applies comprehensive quality control measures during data collection, entry, and processing. For our analysis, we reviewed the dataset for any inconsistencies or missing data to maintain data cleanliness and enhance the reliability of the results. Data were analyzed using SPSS version 25. Descriptive statistics, including frequencies, percentages, were used to summarize the characteristics of the study population. Chi-squared tests were utilized to examine associations between categorical dependent variables (Secondhand smoke inside the home, Secondhand smoke indoors, and Secondhand smoke outdoors) and the independent variables. The assumption of expected cell frequencies was checked, and all cells had expected counts greater than 5, satisfying the requirements for chi-squared tests. Further, multivariable analysis was conducted using binary logistic regression to adjust for potential confounders and to identify independent predictors of smoking attitudes and behaviors.
To ensure the validity of our logistic regression analyses, we tested key assumptions, including multicollinearity and the influence of outliers. Given that all predictors were binary variables, the linearity of the logit assumption does not apply. The goodness-of-fit of the multivariable logistic regression models was assessed using the Hosmer-Lemeshow test, and pseudo R-squared values (eg, Nagelkerke R-squared) were reported to evaluate model performance. Additionally, Cook’s distance was calculated to identify influential data points, and no observations exceeded the threshold (Cook’s distance > 4/n), indicating that no single observation disproportionately influenced the model. Significant two-way interactions among key predictors were also evaluated and included in the analysis where relevant. These interactions provide insights into the relationships between variables and their combined effects on outcomes. All assumptions relevant to our logistic regression with binary predictors were met, supporting the robustness of the results. Adjusted odds ratios (aORs) with 95% CIs were reported. A P-value of <.05 was considered statistically significant.
Ethical Considerations
The 2019 GYTS was conducted following ethical standards, and approval was obtained from the relevant institutional review boards (IRBs) in the Gaza Strip. Participation in the survey was voluntary, and written informed consent was obtained from both students and their parents or guardians. All data were de-identified before analysis to ensure participant confidentiality.
Results
Background characteristics of the study participants (n = 1536).

Distribution of second-hand smoke among youth in the Gaza strip (N = 15007).

Abbreviation: SHS: secondhand smoke.
Internet Café, school rooms and corridors, shops, restaurants, shopping malls,
schoolyard, playgrounds, sidewalks, entrances to buildings, parks, beaches.
Distribution of attitudes in youth in GAZA strip (N = 1536).

Abbreviation: SHS: secondhand smoke.
*Internet Café, school rooms and corridors, shops, restaurants, shopping malls,
†schoolyard, playgrounds, sidewalks, entrances to buildings, parks, beaches.
The association age sex and smoking characteristics in home, indoors, and outdoors SHS.
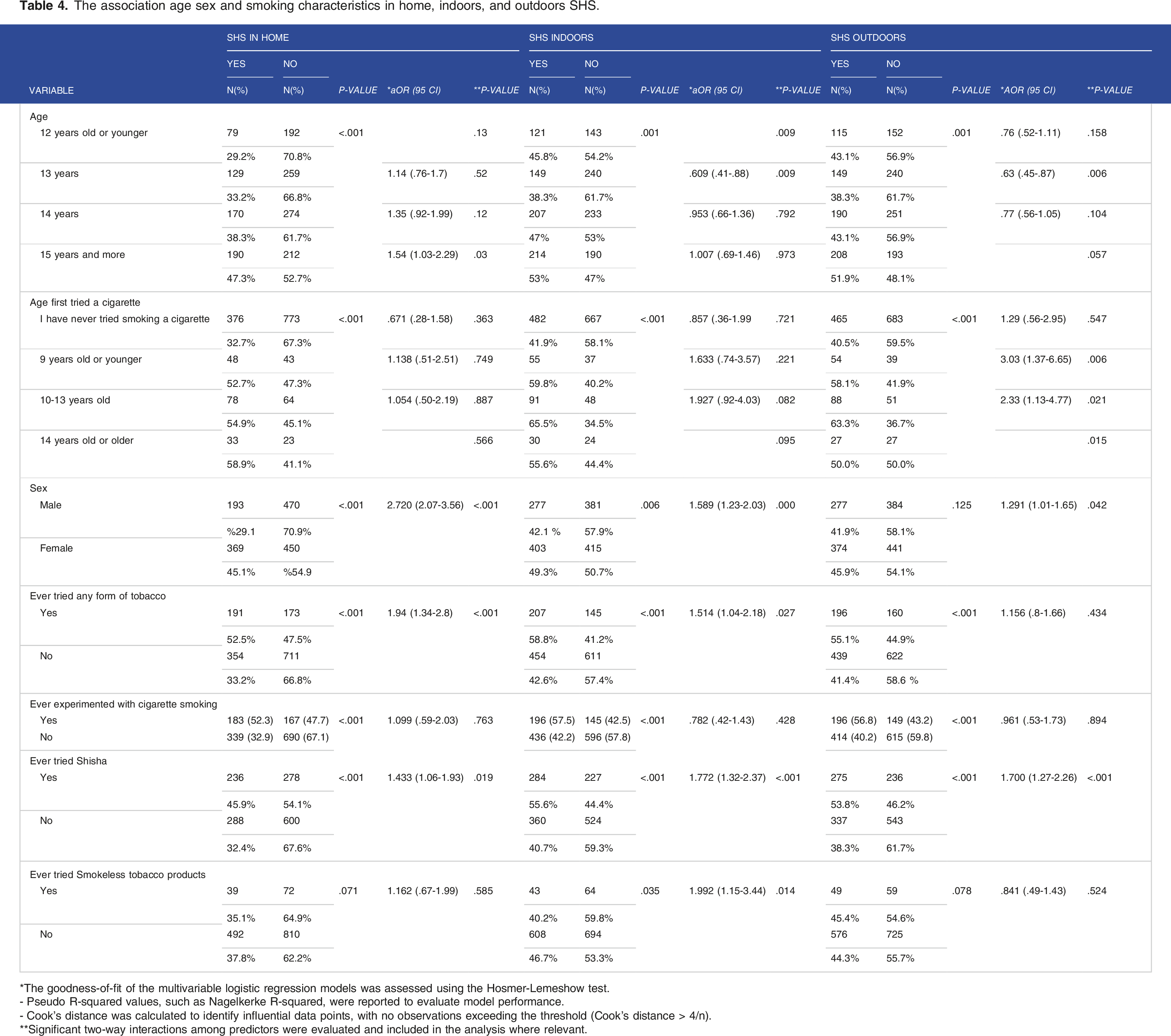
*The goodness-of-fit of the multivariable logistic regression models was assessed using the Hosmer-Lemeshow test.
- Pseudo R-squared values, such as Nagelkerke R-squared, were reported to evaluate model performance.
- Cook’s distance was calculated to identify influential data points, with no observations exceeding the threshold (Cook’s distance > 4/n).
**Significant two-way interactions among predictors were evaluated and included in the analysis where relevant.
Discussion
The data reveal that 25.5% of adolescents in Gaza have experimented with smoking, with a significant proportion beginning this behavior before the age of 15. This early initiation is alarming and mirrors trends observed in neighboring regions; for instance, a national survey in Jordan found that 27% of adolescents aged 13 to 15 had experimented with smoking. 34 Globally, the World Health Organization (2019) reported that approximately 24% of adolescents have tried tobacco before the age of 18. 35 In Greece, it found that 32.1% of students had tried tobacco 36 which is notably higher than the rate observed in this study. Similarly, data from Turkey’s GYTS conducted in 2003 indicated that almost 30% of students aged 13 to 15 had smoked cigarettes at some point, with a higher prevalence among boys. 37 In Brazil, 29.3% of adolescents reported having experimented with smoking, 38 Again, this slightly exceeds the 25.5% observed in this study. These differences may be attributed to cultural, social, and economic variations across regions and the effectiveness of anti-smoking campaigns and public health interventions.
These findings indicate that smoking experimentation remains a prevalent issue among youth, regardless of geography. Furthermore, research shows that individuals who start smoking at younger ages are more likely to develop nicotine dependence and engage in regular smoking later in life. For example, a study found that those who first smoked between ages 14 and 16 were 1.6 times more likely to become dependent compared to older initiators. 39 This connection underscores the urgency of implementing targeted prevention strategies to address early smoking initiation and reduce exposure to risk factors such as secondhand smoke, thereby mitigating the long-term consequences of tobacco use among adolescents.
Our study demonstrates that the two main reasons for starting smoking among youths who use tobacco are curiosity (62.2%, P < .001) and modeling effects (17%, P < .001). Meanwhile, other studies have supported our findings. For example, a study conducted in Pakistan in 2018 shows that the initiation of smoking among non-smokers is often driven by factors such as curiosity, peer pressure, social trends, and a perceived need for experimentation, with curiosity emerging as a predominant motivator influencing individuals to begin smoking. 40 Similarly, a study in Indonesia in 2021 found that several factors contribute to adolescent smoking behavior, including peer pressure, parental smoking habits, perceptions of masculinity, and curiosity. The findings suggest that adolescents view smoking as a social activity, yet their attitudes are often conflicted. Peer influence plays a significant role, alongside modeling behaviors observed from parents who smoke. Additionally, smoking is associated with expressions of masculinity and is often driven by curiosity. 41 Another study focused on e-cigarette use in the United States in 2014 showed similar results, illustrating that the primary reasons for initiating e-cigarette use include curiosity (53%), the influence of friends or family members who use, offer, or provide e-cigarettes (34%), and the desire to quit or reduce traditional smoking (30%). 42
On a global scale, 40% of children are exposed to second-hand smoke. The exposure varies significantly by region, with the Western Pacific (68%) and European (58%) regions showing the highest exposure rates. Conversely, the African region has the lowest exposure rate at 12%. In low-and-middle-income countries of the Americas, 28% of children are exposed, while the Eastern Mediterranean and Southeast Asian regions show exposure rates of 35% and 39%, respectively. High-income countries report a similar rate to that of Southeast Asia, at 39%. These statistics highlight the disparities in SHS exposure among different regions. 43
Our study elaborates that as the child’s age increases, there is a notable rise in exposure to SHS within the home environment. The data for the age group “15 years and more” show a statistically significant association (P = .032, aQR = 1.5) with increased SHS exposure at home. This suggests that older children and adolescents are more likely to be exposed to SHS at home, which may contribute to the adoption of harmful health behaviors, such as smoking initiation and other adverse health effects. A study in Turkey elaborated a clear relationship between people’s age and their exposure to tobacco smoke. 44 A study conducted in 68 low- and middle-income countries shows that tobacco use is approximately 1.6 times higher at ages 14-15 years than at ages 12-13 years. 45 Another study conducted in China implicated that home SHS exposure had a greater impact on tobacco use among adolescents. 7 Additionally, a systematic review of 35 studies found that SHS exposure was associated with a greater likelihood of being a smoker, increased susceptibility to and initiation of smoking, greater nicotine dependence among nonsmokers, and poorer smoking cessation. 3 These findings conclude that the longer the interval of exposure, the higher the susceptibility to smoking. This highlights the importance of targeted interventions to reduce SHS exposure, particularly in older children and adolescents, to mitigate both immediate and long-term health risks.
Females are more frequently exposed to SHS than males across most environments (in the home, indoors, and outdoors) in this analysis. In the home, 45.1% of females are exposed compared to 29.1% of males (P < .001). This group was also vulnerable to SHS in Turkey. 46 Similarly, 49.3% of females experience SHS exposure indoors, slightly higher than the 42.1% of males (P = .006). Although outdoor exposure is more comparable, with 54.1% of females and 41.9% of males exposed, this difference is not statistically significant (P = .125). Similarly, a cross-sectional study found that in 57% of homes in the studied countries, women were more likely to be exposed to SHS than men were. For instance, in India, 72.4% of women were exposed to SHS at home compared to 45.8% of men. In Bangladesh, the findings were 64.2% for women and 48.1% for men, reflecting cultural patterns in smoking behaviors. 47 These findings emphasize the need for targeted interventions aimed at reducing SHS exposure among females, especially in home and indoor environments. Prior research supports the need for gender-specific public health strategies to mitigate SHS risks, particularly in vulnerable populations. 48 Other studies highlight that women, especially in domestic settings, tend to experience higher levels of SHS due to cultural and social roles, which should be addressed in SHS prevention programs. 49
Our research reveals that adolescents who are frequently exposed to SHS, whether in-home or indoor settings or public spaces exhibit a markedly higher susceptibility to smoking, especially traditional smoking, and Shisha. These findings provide critical insights into the dynamics of smoking initiation, illustrating that SHS not only presents significant physical health risks but also contributes to the normalization of smoking behavior among young individuals. The WHO report noted that children exposed to SHS, particularly from caregivers, are 70% more likely to try smoking by age 15. 50 Similarly, the Centers for Disease Control and Prevention (CDC) notes that young people are more inclined to use tobacco products if they are regularly exposed to smoking in their environment, as it becomes normalized. 51 Research indicates that Adolescents exposed to SHS were at higher odds of being susceptible and currently smoking. 7
Our study highlights a significant awareness among youth in the Gaza Strip regarding the bad effects of secondhand smoke (SHS), with 65.2% acknowledging that it is definitely harmful. This awareness likely influences their strong support for smoke-free policies, as evidenced by 73.5% favoring smoking bans in enclosed public spaces and 67.9% supporting bans in outdoor areas. A study conducted in Turkey indicates that social connections, especially close ones, can increase the likelihood of SHS exposure, possibly because trusted family or social groups might include smokers, leading to passive exposure. 52 This implies that social and family behaviors significantly influence exposure to SHS, aligning with the idea that reducing SHS in public and social environments could foster positive behavioral changes, particularly among youth. Despite recognizing the harmful effects of SHS, 43.5% of participants find SHS in social settings uncomfortable, and 55.4% believe smoking makes young people less attractive. However, 48.8% consider quitting smoking challenging, highlighting the addictive nature of smoking and the need for accessible cessation programs.
Smoking tobacco through water pipes, or shisha, is prevalent in Middle Eastern countries and is increasingly popular worldwide, especially among youth. Many mistakenly perceive shisha as a safer alternative to cigarettes; however, it contains harmful substances, including carcinogens, and poses serious health risks to both users and those exposed to secondhand smoke. A 40-minute shisha session can have detrimental effects comparable to smoking over 100 cigarettes. 53 Raising awareness of these health risks is crucial, necessitating coordinated global efforts to address its impact. Notably, we found in our research that adolescents exposed to SHS at home are significantly more likely to experiment with cigarettes (OR: 1.94, P < .001) and shisha (OR: 1.51, P = .027). Indoor and outdoor SHS exposure also increases the likelihood of shisha experimentation (OR: 1.77, P = .002; OR: 1.70, P < .001). These findings underscore the link between SHS exposure and increased tobacco experimentation among adolescents.
Conclusion
The findings of this research underscore the urgent need to address secondhand smoke exposure, particularly among females and adolescents, who are disproportionately affected. Targeted public health interventions are crucial in mitigating the risks associated with SHS, as this exposure not only poses immediate health threats but also contributes to smoking initiation and normalization of tobacco use. Presenting these findings alongside the connection between curiosity, modeling effects, and the initiation of tobacco use among youths. In our opinion, this underscores the need for education and awareness programs for adolescents about the potential social and medical harms of smoking. School-based programs, youth-targeted campaigns, and engaging young people as peer educators to spread anti-smoking awareness in their communities are crucial steps. More importantly, we must focus on increasing awareness among parents and school teachers, given their significant influence on adolescent smoking behavior through modeling effects. Parental education should encourage open communication about the risks of smoking and the modeling of healthy behaviors by not smoking themselves. Additionally, promoting smoke-free homes and providing teachers with thorough training on the health risks of smoking, including secondhand smoke and vaping, will help reinforce positive behavior
Limitations
One significant limitation of the study is its reliance on self-reported data, which may introduce recall bias or under-reporting, particularly regarding sensitive behaviors such as smoking or SHS exposure. Additionally, the cross-sectional design limits the ability to infer causality between SHS exposure and smoking behaviors, as longitudinal studies would be needed to track these associations over time. The study is also context-specific, focusing on adolescents in the Gaza Strip, which may limit the generalizability of the findings to other regions with different socio-economic and cultural factors. Furthermore, the study’s age range is restricted to adolescents aged 13-15, potentially missing insights from younger children or older adolescents who may exhibit different smoking-related behaviors and SHS exposure levels. Finally, we did not perform an independent sample size or power calculation, as it was based on secondary data from the Global Youth Tobacco Survey (GYTS), which uses a standardized methodology to determine sample size. This may limit the analysis’s ability to tailor to the study’s objectives.
However, the study has several strengths that bolster its credibility. Using data from the Global Youth Tobacco Survey (GYTS) ensures a large, nationally representative sample, enhancing the statistical power and the ability to draw robust conclusions. Moreover, the uniformity of the data collection process across different schools increases the reliability of the findings and allows for better comparability with similar studies conducted globally.
Supplemental Material
Supplemental Material - Secondhand Smoke Exposure and Smoking Attitudes and Behaviors Among Adolescents in the Gaza Strip: Findings From the 2019 Global Youth Tobacco Survey
Supplemental Material for Secondhand Smoke Exposure and Smoking Attitudes and Behaviors Among Adolescents in the Gaza Strip: Findings From the 2019 Global Youth Tobacco Survey by Beesan Maraqa, Mahmoud Abu Mayaleh, Seya Arafeh, Kenana Altell, Ahmad khleif, Abdallah Najjar, and Bayyena Aburadwan in Tobacco Use Insights
Footnotes
Acknowledgments
We would like to extend our deepest gratitude to the adolescents and their families who participated in this study and were willing to contribute to this research. We are also grateful to the school administrators and teachers across the West Bank who supported us in facilitating data collection. We are especially thankful to Hebron University for providing the necessary resources and institutional support to conduct this research. We also thank our Department of Family and Community Medicine colleagues for their valuable input throughout the study design and analysis stages.
Author Contributions
B.M., contributed to the study's concept and design. BM, M.A., S.H., K.A., A.K., A.N., and B.A. collected, analysed and interpreted the data. M.A., S.H., K.A., A.K., A.N., and BA drafted the initial draft of the manuscript. BM revised it and prepared it for submission. All authors provided feedback on earlier drafts. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.