
Abstract
Objective:
This study examined caregiver perception of harm and child secondhand exposure to nicotine in a sample of e-cigarette-exclusive, cigarette-exclusive, and non-tobacco/nicotine users (non-users).
Methods:
Cigarette-exclusive (n = 19), e-cigarette-exclusive (n = 12), and non-users (n = 20) and their children (N = 51, Mage = 10.47) completed self-report questionnaires about perceptions of harm, child secondhand exposure, and provided urine to assess child nicotine exposure (cotinine). ANOVAs examined differences between caregiver use status on tobacco harm perceptions and child cotinine levels. Independent samples t-test compared differences in caregiver-reported child secondhand exposure in the home and car.
Results:
All 3 caregiver groups rated cigarettes as highly harmful (P = .14), but e-cigarette users rated all 3 types of e-cigarette products (Cartridge-based: P < .001; Tank: P < .001; Box Mod: P < .001) as less harmful than cigarette users and non-users. Caregivers from the e-cigarette user group reported greater child secondhand exposure than caregivers using cigarettes (past 7-day in-home exposure (P = .03); past 7-day exposure in-home + in-car exposure (P = .02); in-home exposure by caregivers and other people exposure (P = .02)). Children from the cigarette user group had significantly higher levels of cotinine (M = 16.6, SD = 21.7) compared to children from the Non-User group (M = .43, SD = .95; P = .001), but no significant difference when compared to children from the E-Cigarette User group (M = 6.5, SD = 13.5).
Discussion:
In this sample, caregivers who used e-cigarettes perceived them as less harmful, reported using them more frequently at home and in the car, even when their children were present, compared to cigarette users. As a result, children appear to be exposed to nicotine at levels similar to children living with cigarette users. Future caregiver prevention and intervention efforts should target education around the potential harms of secondhand e-cigarette aerosol to children.
Introduction
Rates of smoking and secondhand smoke (SHS) exposure have decreased over the past few decades. Public awareness of the health effects of smoking and SHS has increased, and comprehensive total smoke-free policies have subsequently been implemented to prevent smoking in public places such as workplaces or restaurants.1-3 Secondhand smoke contains harmful chemicals and carcinogens 4 (eg, formaldehyde, benzene, vinyl chloride, arsenic, ammonia, and hydrogen cyanide). Cigarette smoking rates are the lowest on record, with 14% of adults in the United States reporting use of conventional combustible cigarettes in 2018. 5 Tobacco control measures, including smoke-free laws, have been effective in reducing the overall smoking prevalence among adults in the United States.1,3,6,7 However, child exposure to SHS remains high—of the nonsmokers exposed to SHS in 2014, almost 40% were children between ages 3 and 11. 2 Childhood is a particularly vulnerable period in which children are susceptible to the physiological health effects of SHS 8 (eg, respiratory illness, asthma) and may be prone to initiate smoking in the future as a result of regular exposure.6,7,9 Moreover, the greatest levels of SHS exposure for young children occur as a result of caregivers using cigarettes either in the home or car. 10 Therefore, heightened attention must be placed on increasing caregiver awareness of the health implications of SHS so that rates of exposure among children may be minimized.
Use of electronic cigarettes (e-cigarettes) has increased since their introduction in 2007.5,11 E-cigarette aerosols contain nicotine, flavorings, or other additives, while lacking the high levels of carcinogens found in conventional cigarette smoke. 12 To many adult smokers, e-cigarettes are used or viewed as cessation aids and are perceived as safer to use than conventional cigarettes.13,14 However, it is well documented that the aerosol exhaled by e-cigarette users, referred to as secondhand aerosol (SHA), can contain harmful substances including nicotine, heavy metals, ultrafine particulate, volatile organic compounds such as formaldehyde and acetaldehyde, and other toxicants.15-19 In addition, similar to SHS, SHA can remain on surfaces as thirdhand exposure in areas which may expose children to nicotine and other potentially harmful substances. 20
A limited amount of published research has evaluated caregiver perceptions of health outcomes associated with both SHS and SHA exposure in children. A 2015 cross-sectional study found 45% of adults believed SHA caused some to no harm to children. 21 Another recent study among a sample of parents who were cigarette, e-cigarette, or dual users suggested that caregivers,, perceived e-cigarettes as safer to use around children in comparison to cigarettes, regardless of which product they used. 22 Further, this study found that parental characteristics associated with not having smoke/vape bans included smoking more than 10 cigarettes per day, current use of an e-cigarette, and having a youngest child >10 years old. 22 These studies highlight that parental perceptions, specifically as they relate to e-cigarettes, may place children at increased risk of SHS and/or SHA exposure.
Caregiver harm perceptions may play a significant role in reducing SHS and SHA exposure among children. More information regarding the health effects and exposure to harmful and potentially harmful constituents is needed. The perception that e-cigarettes are less harmful than regular cigarettes may impact caregivers’ choices to use e-cigarettes at home and in their car with children present. Therefore, the purpose of this study is to examine how caregiver perception of harm may be associated with child exposure (both objective and subjective) in a sample of e-cigarette-exclusive, cigarette-exclusive, and non-tobacco/nicotine users.
Methods
Participants
This study was conducted at 2 large medical centers in the Midwestern and Southeastern United States. Fifty-one child (aged 5-17 years) and caregiver dyads were recruited to participate in the study. Caregivers were eligible to participate if they lived in the same residence as the participating child and were either (a) non-users of tobacco or e-cigarette products, (b) current conventional combustible cigarette users, who reported smoking at least 10 cigarettes per day for the past 3 months, or (c) current e-cigarette users, who reported using e-cigarettes daily for the past 3 months. Cigarette smoking status was biochemically verified via exhaled breath carbon monoxide (eCO) and via self-report. Caregivers in the control and vaping groups were included if they reported no use of cigarette products and had a breath eCO value less than 6 ppm. 23
Procedures
The study protocol was administered during in-laboratory visits at either the Midwestern or Southeastern medical centers. The IRB at both medical centers approved the protocol and data sharing agreement. All participants completed informed consent/assent prior to completing study procedures. Caregivers completed a series of self-report measures related to current and previous tobacco and e-cigarette use, perceptions of harm related to tobacco products, and home/car smoking/vaping bans. If age appropriate (greater than 10 years of age), children completed a self-report measure to assess their smoking status. Children and caregiver dyads were provided with urine collection cups and instructed to collect a urine sample while in the clinic for analysis of urinary cotinine (a biomarker of nicotine). Families received modest monetary compensation for participation.
Measures
Caregiver variables
Demographics, cigarette, e-cigarette use, household rules, and home-ban
Caregivers provided sociodemographic information for themselves (eg, age, sex, marital status, ethnicity, years of education), their household (eg, number of people in the household, and income range), and child (eg, age, sex, grade, ethnicity). Caregivers provided information regarding household ban (vaping + smoking in-home), self-reported nicotine dependence (Hooked on Nicotine Checklist; higher scores indicative of greater dependence; range 0-10), and number of household users (cigarette or e-cigarette). Cigarette users provided information on number of cigarettes in past 24 hours and ever quit attempts. E-Cigarette users provided information on flavor of e-liquid use, type of e-cigarette, and recency of vaping.
Caregiver-reported child exposure
Child SHS and SHA exposure was assessed with a structured interview with caregivers.24,25 This measure has been used in previous research to elicit self-reported child exposure to smoking (ie, number of cigarettes) in the home and car.24,25 In this study, items were scored to provide estimates of child exposure in the following domains: (a) caregiver past 7-day in-home exposure; (b) total caregiver past 7-day exposure in-home + in-car; (c) total exposure by other people (eg, relatives, visitors) and other places (eg, public places); and (d) total in-home exposure by caregivers and other people. Cigarette users were asked to provide the estimated number of cigarettes the child was exposed to in each of these settings and e-cigarette users were asked to provide the estimated number of minutes/hours the child was exposed to in each of these settings. In order to compare caregiver-reported child exposure, Cigarette User values were transposed from number of cigarettes to number of minutes/hour using past research (see Zacny and Stitzer 26 and Data Analytic Overview section for procedure).
Caregiver perceptions of harm
Caregivers reported on general perceptions of harm associated with use of different nicotine/tobacco products (ie, “How harmful is the following product to your health?”; 100-point scale; 0 = no harm, 100 = extremely harmful). In the present study, harm perceptions related to different e-cigarette products (ie, cartridges, tanks, and modified systems) were evaluated among caregivers.
Child variables
Children self-reported current or previous tobacco product use without the presence of the caregiver. Self-report of youth smoking status was measured with a report of if they have ever smoked a cigarette. The questionnaire includes existing items that have been used in several studies of adolescent smoking. 27 All children provided urine samples.
Objective secondhand exposure: Analysis of urinary cotinine
Analysis of urinary cotinine 28 was performed in a combined procedure as previously described. 28 Briefly, urine samples were mixed with isotope-labeled internal standards, subjected to β-glucuronidase treatment, and purified by solid-phase extraction. To decrease the impact of batch effects, samples from children living with cigarette users, e-cigarette users and non-users were analyzed in randomly assigned batches. The purified samples were analyzed by liquid chromatography-tandem mass-spectrometry (LC-MS/MS).
Data analytic overview
A P-value of <.05 was considered statistically significant for comparisons. Analyses were performed using SPSS version 26. A series of one-way analyses of variance (ANOVAs) were used to examine harm perceptions of different products. ANOVA was also used to examine differences in child cotinine as a function of caregiver use status. In this analysis, secondhand exposure by others besides the caregiver (eg, friends/relatives; other places), was included as a covariate. Given the differences in how data reflecting child exposure was collected (ie, number of cigarettes vs number of minutes vaped), descriptive statistics are reported by product use for caregiver estimated child exposure for in-home, in-car, and total secondhand exposure. Comparisons in the number of hours of child secondhand exposure in each setting (as outlined above) by group were examined by independent sample t-test. To calculate number of hours for the cigarette user group, number of cigarettes were multiplied by 5 (eg, 5 cigarettes/week = 25 minutes of secondhand exposure), as recommended by previous research. 26
Results
Demographics, cigarette, e-cigarette use, household rules, and home-ban
Caregivers in the total sample were primarily female (73%), 35 years-old (SD = 5.74 years), and Caucasian (43%). Children were mostly female (53%), 10 years-old (SD = 2.78) and Caucasian (43%). Caregivers in the cigarette group reported an average of 8 life-time quit attempts, reported using cigarettes for an average of 20 years, and 14.7 cigarettes in the past 24 hours. The majority of e-cigarette and cigarette users reported having a home smoking ban, but only 1 e-cigarette using caregiver reported a home vape ban. Self-reported nicotine dependence was higher for cigarette using caregivers (M = 7.5; SD = 2.5) than e-cigarette users (M = 2.3; SD = 2.5). Tank-style e-cigarettes, fruit and dessert flavored e-liquid, and self-reported demographic and child variables by caregiver use are reported in Table 1.
Caregiver and child demographics.

Abbreviations: M, mean; SD, standard deviation.
Child use of e-cigarette products was only asked among a subset of participants due to survey error.
Caregiver perceptions of harm
All 3 caregiver groups (ie, Cigarette Users, E-Cigarette Users, and Non-Users) rated cigarettes as highly harmful, with no significant differences between groups (F(2, 27) = 2.2, P = .14). E-cigarette users rated all 3 types of e-cigarette products as less harmful than cigarette users and non-users. Among e-cigarette users, cartridge e-cigarettes (F(2, 27) = 15.1, P < .001) were rated as more harmful than e-cigarette tank systems (F(2, 27) = 49.4, P < .001) and e-cigarette modified systems (F(2, 27) = 47.4, P < .001). See Table 2 for harm perceptions by product and among the caregiver product use group.
Caregiver perception of harm for combustible cigarettes and e-cigarette products.
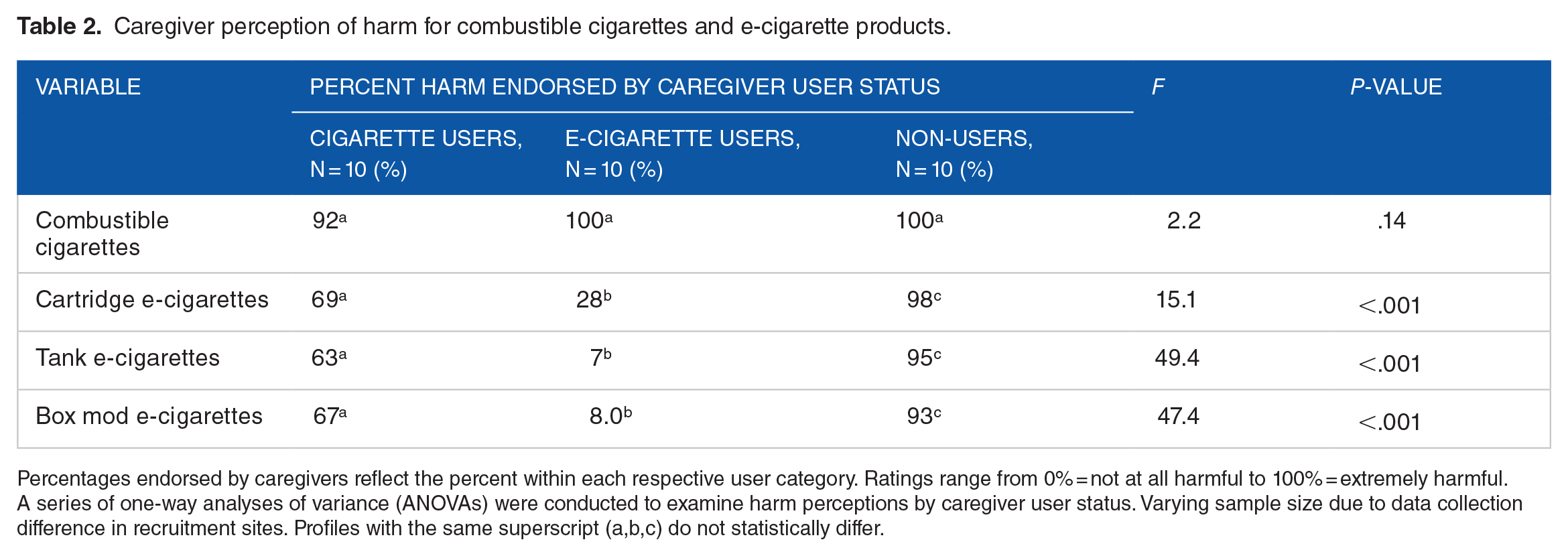
Percentages endorsed by caregivers reflect the percent within each respective user category. Ratings range from 0% = not at all harmful to 100% = extremely harmful. A series of one-way analyses of variance (ANOVAs) were conducted to examine harm perceptions by caregiver user status. Varying sample size due to data collection difference in recruitment sites. Profiles with the same superscript (a,b,c) do not statistically differ.
Caregiver-reported child exposure
Cigarette users
Caregivers reported using an average of 16.4 (SD = 21.1) cigarettes/week in-home around their children. Caregivers also reported that children were exposed to an average of 17.8 (SD = 31.2) cigarettes/week by other people (eg, relatives, friends) or at other places (eg, public spaces, friend’s home).
E-cigarette users
Caregivers reported using e-cigarettes on average of 30.1 (SD = 38.8) hours/week in-home around their children. Caregivers also reported that children were exposed to an average of 21.3 (SD = 20.7) hours/week by other people (eg, relatives, friends) or at other places (eg, public spaces, friend’s home).
Comparison of estimated child exposure: Number of hours by user group
Caregivers from the e-cigarette user group reported greater child secondhand exposure than caregivers from the cigarette user group in the following settings: caregiver past 7-day in-home exposure (Mean Difference = 28.7 hours; t(11) = 2.6, P = .03); total caregiver past 7-day exposure in-home + in-car exposure (Mean Difference = 31.7 hours; t(11) = 2.7, P = .02); and total in-home exposure by caregivers and other people exposure (Mean Difference = 29.3 hours; t(11) = 2.6, P = .02). No significant differences were observed by user group (e-cigarette or cigarette users) for total exposure by other people (eg, relatives, visitors; cigarette users vs e-cigarette users) and in other places (eg, public places; (Mean Difference = 19.8 hours; t(4) = 2.1, P = .10); cigarette users vs. e-cigarette users). Descriptive data for caregiver-reported child exposure by caregiver product use is also reported in Table 3.
Descriptive child exposure by caregiver user status.
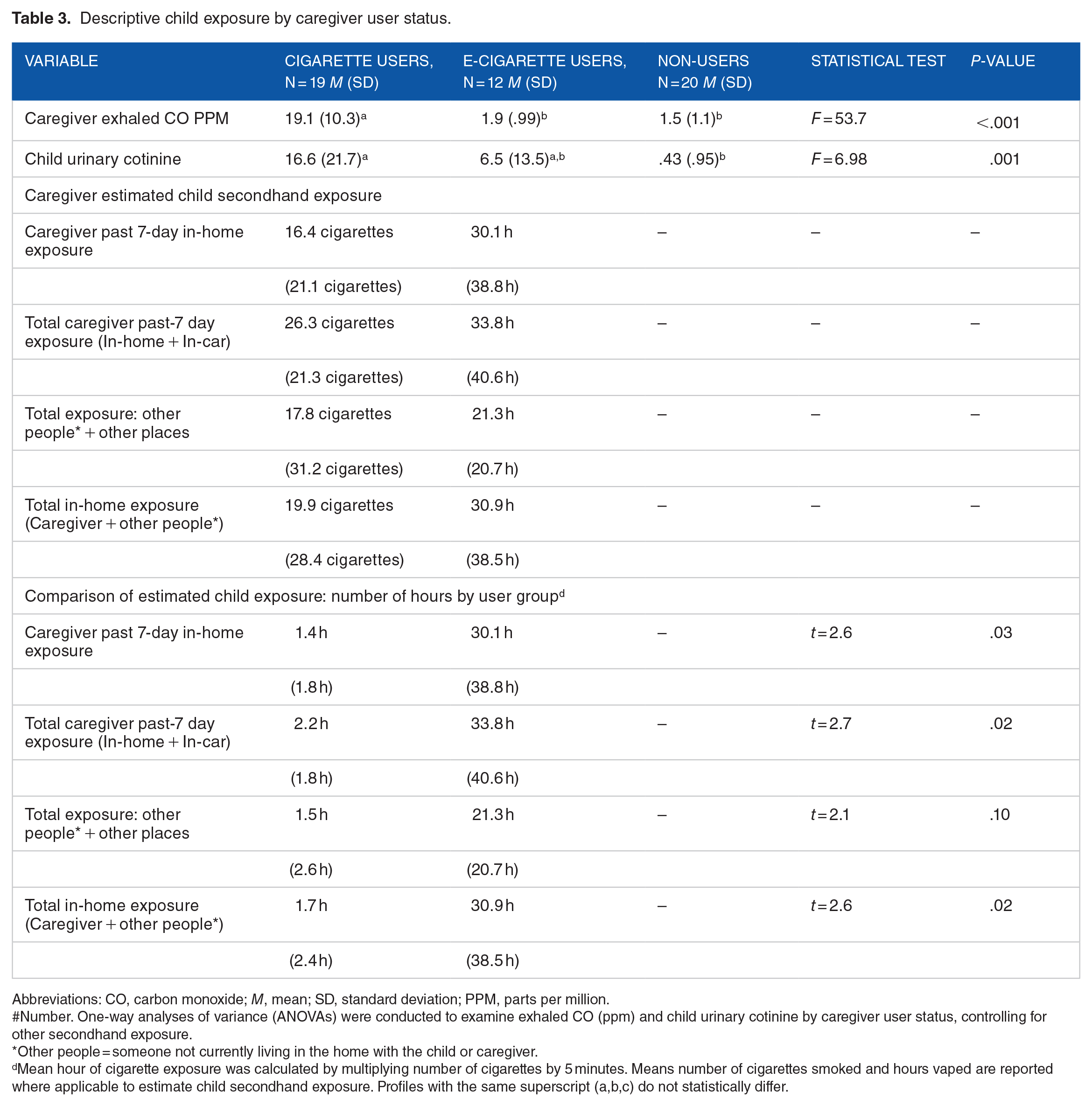
Abbreviations: CO, carbon monoxide; M, mean; SD, standard deviation; PPM, parts per million.
#Number. One-way analyses of variance (ANOVAs) were conducted to examine exhaled CO (ppm) and child urinary cotinine by caregiver user status, controlling for other secondhand exposure.
Other people = someone not currently living in the home with the child or caregiver.
Mean hour of cigarette exposure was calculated by multiplying number of cigarettes by 5 minutes. Means number of cigarettes smoked and hours vaped are reported where applicable to estimate child secondhand exposure. Profiles with the same superscript (a,b,c) do not statistically differ.
Objective secondhand exposure: Analysis of urinary cotinine
Children from the cigarette user group had significantly higher levels of cotinine (M = 16.6, SD = 21.7; see Table 3) compared to children from the non-user group (M = .4, SD = .95; F(3, 49) = 6.98, P < .01), but not significantly different when compared to children from the e-cigarette user group (M = 6.5, SD = 13.5). Children in the e-cigarette user group did not have significantly higher cotinine levels as compared to the non-user group.
Discussion
Our primary objective was to assess differences in tobacco product harm perception and child nicotine exposure—both subjective (caregiver reported) and objective (ie, child urinary cotinine) as a function of caregiver product use status. While non-users, smokers, and e-cigarette users all reported similarly high levels of perceived harm for cigarettes, e-cigarette users rated e-cigarettes as significantly less harmful as compared to ratings of e-cigarettes from the other 2 use groups (cigarette and non-users). Interestingly, most of the vaping caregivers in this sample were male. Previous literature29,30 has highlighted that perceptions of harm differ by gender, particularly males (vs females) often perceive e-cigarettes or other non-cigarette products as less harmful.29,30 As such, larger sample sizes with a more inclusive representation of gender identity (eg, females, and non-binary gender identities) are needed to understand how perceptions of harm may influence use and child exposure (eg, perception that e-cigarettes are not harmful/less harmful increases use indoors and around others).
When examining objective indicators of child exposure, children living with cigarette users showed significantly higher levels of cotinine as compared to non-users, but no significant difference when compared to children living with e-cigarette users. Caregivers reported using an average of 16 to 26 cigarettes/week around their children either in home or in car, equating to an estimated 1.4 hours of exposure; whereas e-cigarette users reported vaping an average of 30 hours per week around their children. While most e-cigarette and cigarette-using caregivers reported a home smoking ban, only 1 caregiver who used e-cigarettes reported having a home vape ban. Together, these data highlight that caregivers in this sample were exposing their children to a relatively high level of secondhand smoke/e-cigarette aerosol. However, even in the context of high rates of secondhand exposure, only the children of cigarette users had significantly higher rates of cotinine as compared to non-users.
The extant literature suggests e-cigarette use is less harmful than conventional cigarette use in terms of traditional carcinogenic markers, but not entirely without harm.14,31-33 While the harm associated with secondhand smoke from cigarettes appears to be recognized by most caregivers, the harm associated with secondhand e-cigarette aerosol is less clear. To date, only 1 study reports on the effects of e-cigarettes within a home setting through both measured airborne nicotine and salivary/urinary cotinine. Ballbè and colleagues found significant differences between adult non-tobacco users living with smokers, e-cigarette users, and other non-tobacco users (control): the highest levels of both ambient and biochemical exposure were observed in those living with smokers, followed by e-cigarette users, followed by non-tobacco users—all mean differences were significant. 34 Additionally, limited laboratory-based studies suggests that exposure to secondhand e-cigarette aerosol leads to similar serum cotinine levels as compared to passive smoking, 35 but may not increase biomarkers of inflammation 36 or impact lung function. 35 However, child nicotine exposure is harmful to neuro-development37-40 and a cause for concern, regardless of the source (secondhand smoke, secondhand e-cigarette aerosol, thirdhand exposure to residue in the living environment).
While our results must be considered preliminary due to the small sample, they are parallel in many ways to what has been reported to date. The current study expands on the literature by examining urinary cotinine in children of cigarette users and e-cigarette users in their natural environment. Similar to the findings of Ballbè et al., children living with smokers had the highest mean urinary cotinine levels, followed by children living with e-cigarette users, followed by children living with non-users; however, observed mean differences were only significant between children living with cigarette users and non-users. In summary, this report demonstrates differences between caregiver’s rating of e-cigarettes based on their own product use status, differences in estimated hours of child exposure based on product use status, and lastly—differences in children’s cotinine levels as a function of caregiver use status. The non-significant differences observed between cotinine levels in the children of e-cigarette users and both non-users and smokers highlights the need for future studies to examine this important question in a larger sample.
This study included limitations that are important to note that impact the generalizability of the current findings, including a small sample size. Future studies should improve upon the current design with a larger sample. Additionally, more recent types of e-cigarette devices may influence outcome variables. While we report on the type of e-cigarette device used, these data were collected in 2016 and as such, e-cigarette devices and e-liquid have rapidly changed. Future studies that develop and utilize validated scales for assessing nuances of e-cigarette aerosol exposure (such as characteristics of the living environment; eg, home/apt./ or sq. ft. of dwelling) will also help to clarify the impact of use on exposure. In order to better understand how secondhand aerosol exposure compares to combustible cigarette exposure, more work is needed to identify common measurement techniques to better capture child secondhand aerosol exposure, particularly when objective measurements like cotinine or ambient dosimeters are unable to be utilized.
In conclusion, the current study demonstrates that e-cigarette use is perceived as less harmful by caregivers who use them and, based on reported exposure time, children living with caregivers who use e-cigarettes may be at higher risk for secondhand nicotine exposure than those living in non-tobacco-using homes. Further research is needed to confirm these preliminary results.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Oklahoma Tobacco Settlement Endowment Trust (APT + TLW), National Heart, Lung, and Blood Institute (5K01HL148907 (APT)), the University of Florida Clinical and Translational Science Institute (DAF), which is supported in part by the NIH National Center for Advancing Translational Sciences under award UL1TR001427, the National Institute on Drug Abuse (U01DA04553 (TLW); R21DA046333 (TLW)), and the National Cancer Institute (R01CA20489 (TLW)). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or the Food and Drug Administration.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.