
Abstract
Introduction
Secondhand smoke (SHS) (so called environmental tobacco smoke) is the smoke from burning tobacco products, like cigarettes, cigars, hookahs, or pipes. 1 It is a mixture of toxic chemical compounds, with more than 7000 chemicals and compounds in SHS, of which hundreds are toxic to human health, and 69 are human carcinogens. There is no safe level of exposure to secondhand smoke; even short exposure can pose serious health problems such as coronary heart disease, stroke, lung cancer and be deadly.2,3
Globally, more than a third of people are regularly exposed to SHS. 4 This is associated with more than 1.3 million deaths and 37.01 million disability-adjusted life-years each year among non-smokers. 5 Article 8 of the World Health Organization Framework Convention on Tobacco Control (WHO FCTC) recommends eliminating exposure to tobacco smoke in indoor workplaces, public transport, indoor public places and other public places. 6 Protecting people from tobacco smoke by creating smoke-free environment is highly cost-effective intervention.1,6 The number of countries implemented comprehensive smoke-free environments has been increasing from 10 in 2007 to 74 in 2022. 7 Despite the existing tobacco control regulations that prohibit smoking in public, there are still a number of people who are adversely impacted by SHS.4,8-10 Reported compliance is the highest in health care and educational facilities and the lowest in pubs, bars and cafes, followed by universities and restaurants. 7 Besides, there remains an equitably protection by smoke free policies and some groups in society are able to be affected by SHS. 11 These groups may include children and adolescents, people with lower income or less education, people living in rental and multi-unit housing and people who live with someone who smokes inside the home.11-16
Vietnam began implementing smoke-free policies by enacting the Law on Prevention and Control of Tobacco Harm (TC Law) in May 2013, and then the Circular No. 11/2023/TT-BYT in 2023 regulates clearly the implementation of smokefree places and consideration for conferment of tobacco-free environment.16,17 Since the regulation has been endorsed, smoking have been completely prohibited indoors and outdoor premises of healthcare facilities, educational institutions, facilities providing care and entertainment services for children, facilities, or areas with a high risk of fire or explosion, in automobiles, on aircrafts and on metro lines.16,17 Besides, the TC Law also mentioned a set of regulations about tobacco manufacturing and distribution, restriction on tobacoo advertising, promotion and sponsorship and tobacco cessation activities. 16 In Vietnam, it is estimated that approximately 34.5 million non-smokers are heavily impacted by SHS in their residences, restaurants, hotels and in the indoor workplaces, putting a significant number of people vulnerable for tobacco related diseases.8,17
The GATS 2010 and GATS 2015 in Vietnam provided valuable information for the advocacy for developing the Law on Prevention and Control of Tobacco Harms. After the GATS 2015, the PGATS (provincial GATS) using the GATS questionnaire was carried out in 34 provinces/cities throughout Vietnam in 2020 and then in 30 provinces/cities in 2022 to monitor and to assess the trend of tobacco use in 2010 and 2022 period, as well as for the comparison with other countries in the region and the world. This paper used data from the PGATS 2022 in Vietnam to describe the prevalence of exposure of the respondents and identify socio-demographic factors associated with exposure to SHS of the adult respondents in 2022. Results reported in this paper will contribute to update the existing evidence on tobacco exposure prevalence in various population groups in Vietnam.
Materials and Methods
Data Source and Study Population
This paper analyzed data from the PGATS 2022, which was conducted in 30 provinces and cities across Vietnam. Our dataset contained the primary information collected from 2022 PGATS questionnaire which was similar to the previous GATS surveys in 2010, 2015 and PGATS 2020. The Vietnam Tobacco Control Fund (VNTCF) under the Ministry of Health led the 2022 PGATS with support from Hanoi University of Public Health (HUPH), the World Health Organization (WHO), local Provincial Centers for Disease Control in the 30 participating provinces/cities and experts in the tobacco control field in Vietnam. As members of the research team, the authors were given full permission to analyze the dataset.
Sample Size and Sampling Method
Study participants were Vietnamese citizens aged 15 years and older. The sample size was designed to estimate key variables by sex and region within each province/city. Each province/city aimed to survey 2400 people (1200 males and 1200 females). In total, the expected sample size was 72,000 individuals across the 30 provinces/cities.
In each province/city, administrative units were first categorized based on economic development status. Then, using simple random sampling, one city/town and two districts with medium or underdeveloped economic status were selected. Within each selected city/town/district, two communes were randomly chosen from the commune lists provided by the local authority in each province. 600 households were randomly selected from these communes (300 households each). In medium/underdeveloped districts, 900 households were randomly selected from three randomly chosen communes. One household member aged 15 years or older was invited from each selected household to complete the survey. There were 71,981 completed interviews, representing a 99.97% response rate.
Variables
The dependent variables in this study were exposure to SHS at home and at work. Exposure to SHS at home was assessed based on responses to the question “What is the level of smoking in your household?”. Besides, exposure to SHS at work was assessed using responses to “What is the level of smoking in your indoor workplace?” All the possible response options for these questions were: “Daily”, “Weekly”, “Monthly”, “More than once a month”, “Don’t know, don’t answer”. Participants who indicated smoking occurred in their household or indoor workplace “Daily”, “Weekly”, “Monthly” or “More than once a month” were considered exposed to SHS.
Independent variables included: Dichotomous variables: (1) Gender (male/female), (2) Ethnicity (Kinh/Other), (3) Being a member of any religion (Yes/No); and (4) Is a current smoker (Yes/No); Ordinal scale variables including: (5) Age groups (15-24, 25-44, 45-64, 65+); (6) The highest education level (Primary school or lower, secondary school, high school, college and higher); Nominal scale variables including: (7) Place of residence (rural and urban areas, in which respondents from cities/towns were classified as living in urban areas, and others from districts were classified as living in rural areas); (8) Occupation (employee, self-employed, housewife/student/retiree, unemployed); (9) Marital status (single, married, divorced/separated/widowed);. These independent variables were selected based on their common usage in the previous GATS 2010, 2015 and PGATS 2020 studies examining exposure to SHS among surveyed participants.
Data Collection
This survey was coordinated by VNTCF under the Ministry of Health. VNTCF supported the 30 participating provinces/cities by providing research assistance, while also collaborating with HUPH to offer technical guidance and field supervision during survey implementation. All interviews were conducted in-person and face-to-face using Android tablets or smartphones. Data were collected via the REDCap (Research Electronic Data Capture) application, which has been utilized in the PGATS 2020 and other recent studies due to its capabilities for optimizing questionnaire design, development, deployment, and data capture. This platform allowed for immediate transfer of data to the research headquarters for quality management, monitoring, and cleansing. 18 Data was transferred immediately to the research headquarters after the respondents finished their interviews.
Data Analysis and Statistical Method
Data management and analysis was conducted by STATA 18 software. Descriptive statistics, including frequencies and percentages, were used to summarize key dependent and independent variables. The prevalence of exposure to SHS at home and at work was estimated according to participant demographic characteristics. Bivariate analysis utilized chi-square tests to examine unadjusted associations between variables, applying a 95% level of statistical significance. Multivariate logistic regression modeling was then performed to adjust for potential confounding among independent variables. The strength of observed relationships was measured through unadjusted odds ratios (ORs) in bivariate analysis and adjusted ORs (aORs) from the multivariate logistic regression, both reported with 95% confidence intervals (CIs). Weight values calculated for each participant were incorporated into all statistical analyses to account for the complex survey design. We have examined and verified several key assumptions for logistic regression, including the linearity of the logit, independence of observations, and absence of multicollinearity.
Ethical Considerations
Ethical clearance for this study was sought from and granted by the Ethical Committee for Biomedical Research at the HUPH under the Decision No. 242/2022/YTCC-HD3 dated 15/6/2022.
Results
General Characteristics of the Study Respondents
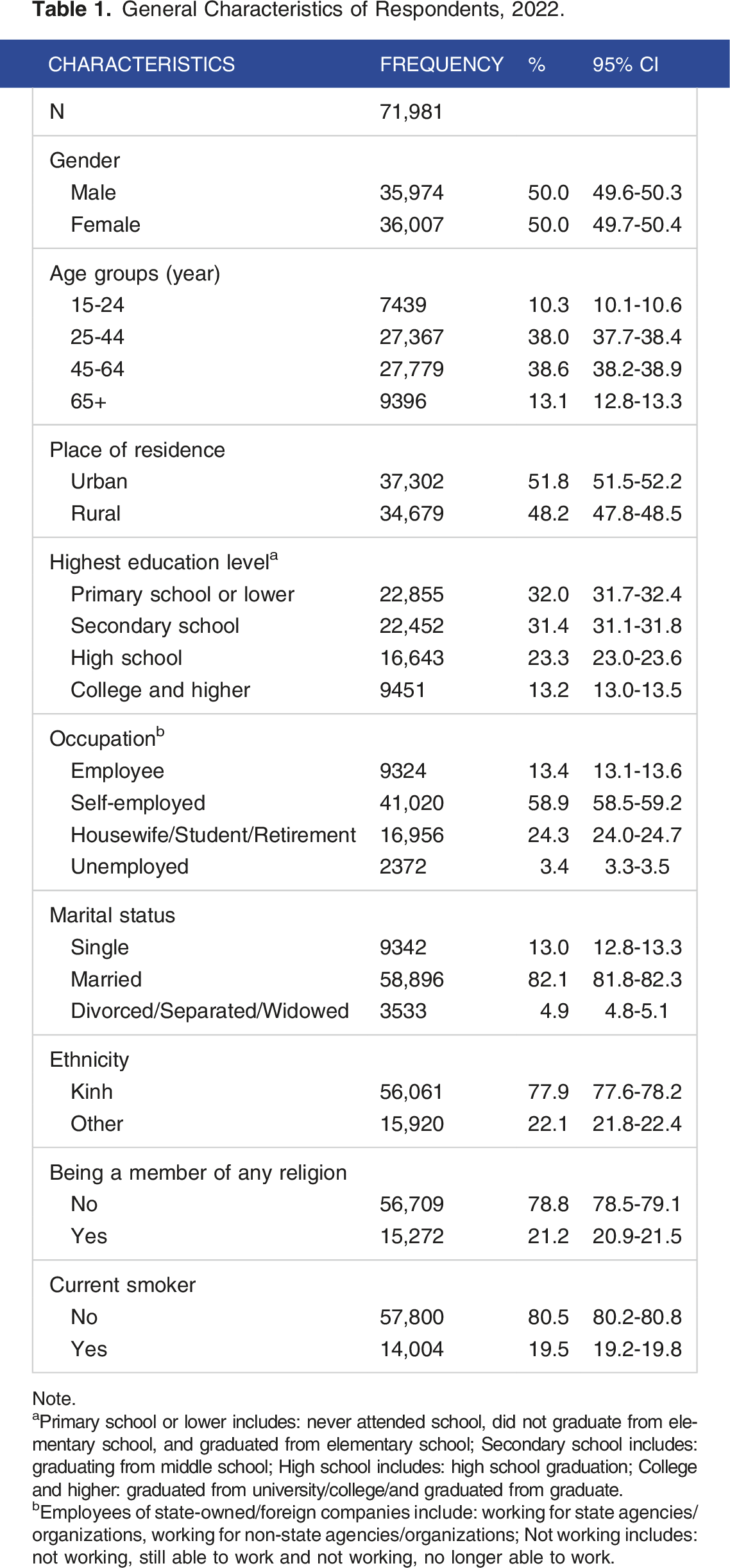
General Characteristics of Respondents, 2022.
Note.
aPrimary school or lower includes: never attended school, did not graduate from elementary school, and graduated from elementary school; Secondary school includes: graduating from middle school; High school includes: high school graduation; College and higher: graduated from university/college/and graduated from graduate.
bEmployees of state-owned/foreign companies include: working for state agencies/organizations, working for non-state agencies/organizations; Not working includes: not working, still able to work and not working, no longer able to work.
A total of 71,981 individuals participated in the survey. The results reveal an equal distribution of males (50%) and females (50%) among the respondents. While most of the surveyed respondents belonged to the age groups of 25-44 and 45-64 (38.0% and 38.6%, respectively), there was a relatively smaller proportion of the participants at the age group of 15-24 (10.3%) and 65+ (13.1%, Table 1). Geographically, 51.8% of the respondents resided in urban areas, while the remaining 48.2% lived in rural regions. Regarding educational level, a similar proportion completed primary school or lower and secondary school (32.0% and 31.4%, respectively) and 23.3% completed high school education. Most of the respondents were self-employed (58.9%), followed by housewives, students, or retirees (24.3%), employees (13.4%) and only 3.4% were not employed. Regarding marital status, 13.0% of participants were single, 82.1% were married, and the remaining were divorced/separated/widowed. More than ¾ of the participants were Kinh ethnicity (77.9%), 22.1% were other ethnics of Vietnam, and a similar proportion was non-religious (78.8%). 80.5% were non-smokers while 19.5% were current smokers (Table 1).
Prevalence of SHS Exposure in the Past 30 Days Among the Study Respondents in 2022.

a“Daily”, “weekly”, “monthly” and “more than once a month” exposures; excludes people who report not being allowed to smoke indoors.
bFor those who work somewhere other than housing.
Table 2 provides an overview of the prevalence of the exposure to SHS at home and the indoor workplace within the study population. The results revealed that 44.4% (95% CI: 44.0-44.9) of respondents experienced SHS exposure at homes, while 23.1% (95% CI: 22.6-23.6) were exposed at indoor workplaces. Notably, females exhibited lower levels of SHS exposure in both home and indoor workplace environments compared to males. The prevalence of SHS exposure remained consistent across all age groups and other demographic characteristics.
Multiple Logistic Regressions for the Exposure to SHS of the Respondents, 2022.

Data in bold showing statistically significant.
In the adjusted model for SHS exposure at the indoor workplace, females had lower odds of exposure compared to males, with an odds ratio of .86 (95% CI: .80-.92). The results also revealed that participants residing in urban areas had 1.15 times higher odds of SHS exposure at the indoor workplace than those in rural areas (95% CI: 1.08-1.22). Furthermore, current smokers had 2.2 times higher odds of exposure to SHS at the indoor workplace compared to non-smokers (95% CI: 2.05-2.37).
Discussion
The Prevalence of Exposure to Secondhand Smoke Among the Study Respondents
Our study contributes to update the national statistics about the exposure to SHS in Vietnam among the adult population. It pointed out that the percentage of SHS exposure among the respondents at home was relatively high (44.4%). Among those who did not smoke, the percentage was 34.1%. These findings were much lower than the GATS’s results in 2010 and 2015 and PGATS 2020 in Vietnam that used the same data collection tool, of which, the rate of SHS exposure at home was 73.1%, 59.9% and 56% for all participants and 67.6%, 53.5% and 44.4% for non-smokers in respective years.19-21 The SHS exposure at home in our study and GATS were measured by the level of smoking inside the household of all members in the family. Comparing to the international database, our results were higher than a study finding in Germany (25.1% among the non-smokers) 9 and lower than another study finding in Bangladesh (54.9%). 22
Regarding the SHS exposure of study population and those who did not smoke at indoor workplaces, the finding showed that the rates were 23.1% and 18.8%, respectively. Comparing to the findings of the GATS in 2010 and 2015 in Vietnam in general, the SHS exposure at indoor workplaces has been decreased significantly. At those times, the rates were 55.9% and 42.6%, respectively. 23 The rates in PGATS 2022 were also lower than those reported in PGATS 2020, which were 30.9% for all participants and 26.7% for non-smokers. 21 This substantial reduction could be implied that efforts in implementing, and enforcement of the TC Law in Vietnam might have brought significant contribution in reducing the prevalence of smoking at indoor workplaces and at homes, therefore reducing community exposure to SHS both at homes and at indoor workplaces. Compared to the foreign studies, our results were also lower than the findings from Germany (40.9%) 9 and US (25.2% among the non-smokers). 24 The difference could be due to the different time of data collection, the regulations for smoking behavior at indoor workplaces and enforcement levels in each country.
Socio-Economic Factors Associated With the Exposure to Secondhand Smoke
In our study, female respondents were more exposed to SHS at home but less exposed to SHS at indoor workplace than male participants. It might be referred to the percentage of SHS exposure at indoor workplaces was much lower than that at homes. It could be explained that the Vietnam TC Law and its sub-law documents prohibit smoking at indoor working places and require the responsibilities of the heads or bosses of organizations/agencies to implement this regulation, 17 while no legislative documents regarding prohibiting smoking at home was released in Vietnam up to present. Communication campaigns on the harmful effects of tobacco and smoking were among the solutions to target banning smoking at indoor home areas and no enforcement was available. Due to this fact, female non-smokers might have been inhaled tobacco smoke from smokers living in the same homes and this resulted in the higher prevalence of exposure to SHS at homes than at indoor workplaces. These findings were relevant to that of the GATS 2010, 2015 and PGATS 2020 in Vietnam.21,23 Results of the two GATS 2010 and 2015 also showed the similar result about the SHS exposure of women at indoor workplaces. 23 The findings related to the female SHS exposure at home was similar to previous studies conducted in Vietnam and Bangladesh that being female was an increasing risk of exposing to SHS at home. 25 Other studies in The Gambia also revealed that women and girls was easier to be exposed to SHS at public places or at home. 10 However, the study in Germany found the contradict findings that men could have higher chance of exposing to SHS than women, especially at indoor workplaces. 9 It might be referred to the different smoking ban policy at the working place in particular and tobacco control law in each country. Our findings imply that it is needed to reinforce and improve the smoking ban policies in the working areas, so as reducing exposure to SHS among both genders at indoor workplaces.
It is shown in our study that all groups of older age were likely to be less exposed to SHS at home than the reference age group of 15-24 years old (P < .001). This result was similar to another study in Khanh Hoa, Vietnam which indicated that the younger groups were at higher level of SHS exposure comparing to reference age group. 25 The oldest age group above 65 years old also was significantly less exposed SHS at indoor workplaces than young people aged 15-24. The Vietnam Labor Code 2019 regulates in its article 169 that the retirement age of men and women in Vietnam will be 62 and 60 respectively by the time 2028, while the previous Labor Code had regulated the retirement age by 60 for men and 55 for women. 26 This could support the explanation of the likely lower exposure to SHS among the age group 65+ in this study, and those old people might have worked in the private sectors because the regulations apply mainly for the public sectors. Generally, our study’s findings also were in accordance with other studies in Germany, 9 the US15,27 that younger age is also an important factor associated to the SHS exposure.
Respondents living in urban areas were likely to be exposed to SHS at indoor workplaces more significant than those living in rural areas. This result was not relevant to results found in GATS 2010, 2015 in Vietnam or a study in Germany, as these two studies found no difference between living location to SHS exposure at indoor workplaces.9,23 It could be due to the time of data collection and proportion of respondents who live in urban or rural areas in each study. Other international studies also revealed that urban residence was strongly associated with exposure to SHS at the public places, such as in the Gambia 10 or at some other places in Germany. 9
Surprisingly, in our study, people with primary educational level and lower had a lower exposure to SHS at indoor workplaces than people with higher education levels, while the respondents with college or higher education level had lower likelihood of exposure to SHS at home than respondents with primary or below education level. Some other studies in the US, Gambia, Myanmar and Germany showed that higher level of education was associated with lower odds of exposure to SHS.9,10,24,28 Obviously, people with higher level of education may have better knowledge about smoking harm and have better preventive measures to protect their health from SHS, especially at homes. We suggest to investigate more in-depth understanding about the association between educational level and exposure to SHS at indoor workplaces.
Our study indicated that ethnic minorities were less likely to be exposed to SHS than Kinh people. Since ethnic minorities normally live in their communities those were far away from the centers with lower socio-economic status comparing to Kinh people while the Kinh people accounted for the majority of total population and in our study population, it was obvious that ethnic minorities had less chances to expose to SHS. Other studies in the US and the Gambia also showed that ethnicity was associated with exposure to SHS.10,27 However, some other studies could not find any association between ethnicity and reported exposure to SHS. 29
One of factors affecting to the SHS exposure at home is the religions of the community. In Vietnam in general and this study in particular, it is a fact that people who do not follow any religion account for a significant proportion. Respondents who were following any religions were likely to report lower exposure to SHS at home than non-religious respondents. This result was contradicted with a study finding in Myanmar that Buddhist women had a greater risk of SHS exposure than others. 28 It can be explained by the differences of study subjects, sample size and local culture between our study and the Myanmar’s study (407 pregnant women).
Current smokers have higher exhibition of exposure to SHS at home and indoor workplaces compared to non-smokers. This result was not congruent with the GATS studies in Vietnam in 2010 and 2015 while there was no difference of smoking status and reported exposure to SHS. 23 In common, smokers are likely to smoke if other smokers are smoking around him/her, therefore the chance of being exposed to SHS would be greater. Other studies in Bangladesh, Malaysia and Portugal also revealed similar results that current smokers had higher odds of being exposed to SHS at various places.22,29,30
Strengths and Limitations of the Study
One of the strengths of this study is to adopt the verified data collection questionnaire of the GATS study so that the validity and reliability of information collected is assured. The sample size of this study is quite large, with 71,981 participants living in 30 provinces/cities throughout the country, which could provide reliable estimates. In addition to some strengths, our study also has limitations. For example, it was possible for the occurrence of recall bias since the information collected was asked within the recent 30 days before the time of data collection. To overcome this weakness, we have trained the data collectors skills to ask the respondents for their maximized thoughts of what happened during the time of 30 days for the best data collection. The time frame of recalled 30 days was also used by other studies in different types of studies.
Conclusion and Recommendations
Although there have been lots of efforts in tobacco control since the TC Law has been enacted, the prevalence of exposure to SHS at home in Vietnam in 2022 was still relatively high amongst the adult population, while there was a significant reduction of SHS exposure at indoor workplaces, with a higher prevalence of women to be exposed to SHS at home while a lower of exposure to SHS at work among women. The prevalence of expousre to SHS was approximately similar among various socio-demographic characteristics of the study population.
The Vietnamese Government should take efforts to continue strictly implementing the smoke-free environment provision at indoor workplaces to protect people from tobacco smoke while consider more effective communication campaign to encourage community, especially women, avoiding exposure to SHS at home.
Footnotes
Acknowledgements
The survey of tobacco uses among adults at 30 provinces/cities in Vietnam in 2022 (PGATS 2022) was successfully implemented with the valuable contribution from many organizations, including WHO office in Vietnam, the Vietnam Tobacco Control Fund, Hanoi University of Public Health, and the proactive collaboration from provincial CDCs. We also valued the collaboration and supports of both governmental, non-governmental organizations, and experts in tobacco harm prevention in Vietnam.
Author Contributions
TTTH, PVC, HVM, LNK, PTH, NTL, DTA, and LTH conceived and designed the study, agreed with the results, conclusions and came up with arguments for the manuscript. TTTH, PVC, LTH, LNK, PTH, NTL, DTA, NDT, and HVM coordinated data collection. LTTH, LTH, PVC, NTT, NQA, PTTT, NTH, and DLHM analyzed the data. LTTH, LTH, NTT, TTTH, NQA, PTTT, NTH, DLHM and HVM wrote the first draft of the manuscript. All the authors made critical revisions and agreed on the final versions of the manuscript, which was submitted by TTTH.
Data Availability Statement
Raw data were generated at Hanoi University of Public Health, Vietnam. Derived data supporting the findings of this study are available from the corresponding author on request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Vietnam Tobacco Control Fund under Grant number 29/2022/HĐ-QPCTHTL-ĐHYTCC dated 28/4/2022.