
Abstract
Background:
Smaller workplaces frequently employ low-wage earners, who have higher smoking rates. Organizational culture and workplace health climate are two characteristics that could influence employee smoking. The purpose of this study was to examine the associations between organizational culture, workplace health climate, and smoking among employees at small (20-99 employees) and very small (<20 employees) workplaces. We proposed the following hypotheses: a stronger clan culture will be associated with a better workplace health climate (HP1); a better workplace health climate will be associated with lower odds of current smoking (HP2); and there will be an association between workplace health climate and smoking intensity (HP3) and between workplace health climate and quit intention (HP4).
Methods:
Executives and employees completed separate online questionnaires. Data collection occurred between June and October 2017. We used regression and Fisher’s exact tests to answer study hypotheses.
Results:
Workplaces with stronger clan cultures had a better workplace health climate (b = 0.27, P < .05), providing support for HP1. A better workplace health climate was associated with lower odds of being a current smoker (odds ratio [OR] = 0.08; 95% confidence interval [CI]: 0.01, 0.53), providing support for HP2. No significant relationship existed between workplace health climate and smoking intensity (P = .50) or between workplace health climate and intention to quit smoking (P = .32); therefore, HP3 and HP4 were not supported.
Conclusion:
Certain culture types may inform an organization’s health climate. Despite a lower likelihood of current smoking in workplaces with better health climates, a better health climate may not be sufficient to produce changes in smoking behavior and intentions.
Introduction
Smoking cigarettes increases the risk for disease and places an excessive burden on the economy.1,2 Small and very small workplaces, defined here as places employing between 20 to 99 employees and less than 20 employees, respectively, comprise 98% of all workplaces in the United States. 3 Compared with larger workplaces, smaller companies more commonly employ low-wage employees, 4 whose smoking rates tend to be higher. 1 Knowing this makes it important to understand factors that contribute to smoking behavior among employees at these workplaces.
Organizational culture and organizational climate may be important to health promotion in the workplace. Culture refers to the basic assumptions and norms shared by members within an organization,5,6 while climate is defined as the shared perceptions and meaning given to practices and policies within an organization. 7 Ashforth 8 suggested that culture informs climate by helping individuals understand their experiences and indirectly through its impact on the objective environment of the workplace. Others have defined climate as reflecting the norms and values of culture. 9
Previous studies have found associations between culture and climate. The competing values framework, initially developed by Quinn and Rohrbaugh, 10 describes four cultural domains with competing expectations: clan, adhocracy, hierarchy, and market. Team building, collaboration, and human resources development characterize clan culture. Innovation, entrepreneurship, and creativity characterize adhocracy culture. Efficiency, timeliness, and control characterize hierarchy culture. Competition, goal setting, and profitability characterize market culture.10,11 Stronger clan or constructive cultures in particular have been positively associated with dimensions of organizational climate (e.g. safety climate).12–15
One aspect of climate relevant to tobacco control is workplace health climate, defined as the shared perceptions related to an organization’s priorities and practices for health. 16 Workplaces perceived by employees as valuing their health and supportive of healthy behaviors are said to have better health climates. 17 Workplace health climate has been positively correlated with the number of tobacco programs offered. 18 Evidence regarding the relationship between health climate and smoking status is mixed, with some studies finding a negative correlation between health climate and current smoking 19 and others showing no significant relationship. 18
Studies examining the relationship between workplace health climate and other smoking behaviors (e.g. smoking intensity) are limited. As noted by Hoert, 20 few studies exist in which workplace health climate is operationalized and even fewer that measure employee health outcomes. Research on the association between organizational culture and workplace health climate also warrants further attention; knowing how culture influences workplace support for health, and how this support could directly impact smoking, is critical for the development of organizational-level strategies to reduce the harmful effects of this behavior. Finally, studies have primarily focused on larger workplaces, despite calls to address health promotion within smaller organizations. 21 Given the increased potential for smoking-related health disparities among employees at smaller workplaces, it is especially important to understand what organizational characteristics impact their health behavior.
The purpose of this cross-sectional study was to examine the associations between organizational culture, workplace health climate, and smoking among employees at small and very small workplaces. We proposed the following hypotheses:
HP1. A higher clan culture score will be associated with a higher (better) workplace health climate.
HP2. A better workplace health climate will be associated with lower odds of being a current smoker (vs non-smoker).
HP3. There will be an association between workplace health climate and smoking intensity, with a higher proportion of light (vs moderate/heavy) smokers existing at workplaces that have a higher (vs lower) workplace health climate.
HP4. There will be an association between workplace health climate and intention to quit smoking, with a higher proportion of smokers who intend to quit smoking within 6 months (vs no intention) existing at workplaces that have a higher (vs lower) workplace health climate.
Methods
Sample and design
We recruited workplaces through ReferenceUSA, a national database of businesses in the United States. 22 We used the following inclusion criteria to select businesses from the database: defined as being a small (20-99) or very small (<20 employees) workplace, having an executive e-mail address available and verified as an open business. To compare and contrast findings between this and a related study, 23 we restricted the sample to workplaces in Iowa. Approximately 40 000 workplaces qualified to participate and 10 470 were sampled using quasi-random sampling techniques. To ensure an adequate sample of both small and very-small workplaces, we stratified the sample by workplace size.
After removing duplicate records and workplaces contacted for a related study, 23 9470 workplaces remained. The first author (C.M.K.) sent e-mails to executives from these workplaces between June and October 2017, inviting them to participate in a brief online questionnaire. Up to two reminders were sent to non-respondents by e-mail and telephone. Executives who completed the questionnaire were provided with an e-mail containing a link to access the employee survey. Executives distributed this e-mail to their employees on behalf of the first author. As incentive for participation, executives and employees were entered into separate drawings to win one of three US$75 gift cards. The University of Iowa’s Institutional Review Board approved all research protocols.
Measures
Executive questionnaire
The executive questionnaire asked questions about smoking policies, cessation activities, and general workplace characteristics. These measures were used as covariates in analysis and created based on previous studies and measures.23–26 In addition to answering questions about indoor and outdoor smoking restrictions, we asked respondents to check, from a list of items, other initiatives adopted by their workplace that went beyond state law requirements. Example smoking policy items included the following: “Are employees allowed to smoke inside the building at your worksite?” and “In addition to cigarettes, e-cigarette use is restricted or prohibited at my worksite.” We calculated a smoking policy strength score by summing the coded responses to all smoking policy items, with higher scores representing a more comprehensive smoking policy (range: 0-9).
For cessation activities, we asked executives to indicate, from a list of items, what programs or activities their worksite offered to help employees quit smoking. An example item: “Your worksite or a contracted vendor provides referrals to employees for smoking cessation assistance (e.g. telephone number to state telephone quitline, information for local counseling services).” Based on the responses to these items, we classified workplaces as either offering or not offering activities.
Executives reported their workplace industry based on North American Industry Classification System codes. 27 Example industries listed on the questionnaire included “Agriculture, forestry, and fishing,” “Wholesale and retail trade,” and “Service.” Executives also reported the percentage of full-time employees, whether most of their employees worked in the building or out in the field, and whether their workplace offered health insurance. We adapted and created these items based on previous study findings.25,28,29
Due to small cell sizes, we collapsed and recoded the following variables: workplace industry (service vs non-service), percentage of employees employed full-time (0%-75% vs greater than 75%), and health insurance (yes vs no/not sure). Using information provided by ReferenceUSA, we created variables for workplace size (small vs very small) and county area designation where the workplace resided (noncore; micropolitan; small metro; and medium metro), the latter of which based on the 2013 National Center for Health Statistics Urban-Rural Classification Scheme for Counties. 30
Employee survey
We assessed organizational culture using a measure from Yeung et al, 31 which contains three items corresponding to each culture type described in the competing values framework (12 items total). We asked employees to indicate how similar each item was to their own workplace, with responses ranging from low to high. One example item from this measure: “This organization is a very production oriented place. People are concerned with getting the job done.” We averaged together the items corresponding to each culture type to create culture scores. Cronbach’s alpha coefficients for the four cultural archetypes ranged from 0.73 to 0.79.
We measured workplace health climate using a five-item subscale from a worksite health and safety climate measure. 18 Employees indicated the extent to which they agreed or disagreed with each item, with responses ranging from strongly disagree to strongly agree. An example item from this scale is “My supervisor encourages me to make changes to improve my health.” We averaged these items to create a climate score, with higher scores indicating a better workplace health climate (range: 0-5). Cronbach’s alpha for this scale was 0.69. We also created a dichotomous version of this variable by splitting responses at their median, with workplaces coded as having a lower or higher health climate (refer to the data analysis section for more details).
To assess smoking status, we asked employees to indicate whether they had smoked at least 100 cigarettes in their entire lifetime and if they currently smoked cigarettes every day, some days, or not at all. Based on previous recommendations, 32 we classified employees who smoked at least 100 cigarettes in their lifetime and smoked every day or some days as current smokers. Employees who smoked at least 100 cigarettes in their lifetime but did not currently smoke were classified as former smokers. Employees who smoked less than 100 cigarettes in their lifetime were classified as never smokers. We dichotomized smoking status into current smoker (= 1) versus non-smoker (= 0) for analysis.
To measure smoking intensity, current smokers reported the average number of cigarettes that they smoked per day on the days that they smoked. Similar to previous studies, 33 we classified smokers as either light (1-9 cigarettes per day) or moderate/heavy smokers (10+ cigarettes per day). We measured intention to quit smoking by asking current smoking employees whether they seriously intended on quitting smoking within the next 6 months (yes vs no).
We measured demographics known or hypothesized to influence smoking behavior and used these measures as covariates in analysis. Specifically, employees reported their age, sex, race, ethnicity, education level, income, occupation, job tenure, and hours worked per week. These questions were taken or adapted from previous measures.34–37 Due to small cell sizes, we collapsed and recoded the following variables: race (white vs non-white); education (college graduate vs some college or less); income (less than US$75k vs US$75k or more); and occupation (management, professional, and related; service; sales and office; and other).
Data analysis
We conducted data analysis in Stata 15.0 38 and R Studio 3.3.2. 39 We calculated descriptive statistics for each variable, followed by bivariate and multivariable analysis. We used linear regression to test HP1. Clan culture was the main independent variable of interest, but given this study’s broader focus on organizational culture, we also included three other culture types (adhocracy, hierarchy, and market) in the regression model. We tested HP2 using mixed-effects logistic regression, an approach that takes into account nested data (e.g. employees nested within organizations). We used a random-intercept model, which allowed the intercept to vary across workplaces. The intraclass correlation coefficient (ICC [1]) for the fully unconditional model was 0.07 (95% confidence interval [CI]: 0.00, 0.64), indicating that 7% of the variance in smoking status was due to differences across workplaces and suggests a small to medium effect. 40
Descriptive statistics: Workplace and employee characteristics.

Descriptive statistics for workplace health climate and organizational culture were calculated only among workplaces with employee data available (n = 68). Due to missing data, percentage denominators may be smaller than the listed sample sizes for executives and employees.
Given the small sample of current smokers in this study (n = 34), we ran Fisher’s exact tests using the dichotomous workplace health climate variable to test HP3 and HP4. The Fisher’s exact test does not rely on asymptotic theory and is valid for small samples. 41 All multivariable analyses included the organizational- and individual-level covariates described earlier (note: due to extremely small cell sizes, ethnicity was not included as a covariate). To obtain organizational-level measures of culture and climate, we averaged employee responses across each workplace. We calculated rho-within-group coefficients for multi-item scales, rwg(j), 42 for each of the four culture types and health climate. The mean coefficient for clan was 0.76, for adhocracy 0.73, for hierarchical 0.73, for market culture 0.78, and for workplace health climate 0.88, indicating an adequate mean level of agreement on these measures. 43
Results
Participants
A total of 264 executives participated in the study. A total of 405 employees from 71 workplaces completed the employee survey, with the number of participating employees at each workplace ranging from 1 to 22 (M = 4.11). Three workplaces were found to employ over 99 employees, and two executives who participated in the executive questionnaire had recently retired. Based on this information, we excluded these executives (n = 5) and their employees (n = 116) from analysis. We excluded nine additional employees because they incorrectly entered their workplace ID on the survey, which made it impossible to link their responses to their executive’s data. The final sample sizes for analysis were 259 executives, 280 employees, and 68 workplaces.
Main findings
The mean workplace health climate score was 3.08 (SD = 0.48). The mean values for culture were similar, ranging between 3.12 (SD = 0.69) to 3.81 (SD = 0.68). Most executives reported that their workplace was in the service industry (54%, n = 138), had employees who primarily worked in the building versus in the field (82%, n = 210), offered health insurance (69%, n = 178), and had greater than 75% full-time employees (57%, n = 146). About a third of workplaces resided in areas classified as medium metro (i.e. 250 000-999 999 residents). The mean smoking policy strength score for workplaces was 4.84 (SD = 1.92). Only 23% (n = 59) of workplaces offered smoking cessation activities.
The mean age for employees was 42 (SD = 12.69). Most employees were female (70%, n = 190), non-Hispanic, Latino/a, or Spanish (99%, n = 270), white (96%, n = 263), college graduates (63%, n = 172), and made at least US$75 000 a year (50%, n = 135). The most common occupation type was management, professional, and related (38%, n = 104). The mean number of years on the job was 11 (SD = 9.60), with an average of 42 (SD = 10.41) hours worked per week. Only 12% (n = 34) of employees were current smokers, with an equal proportion of light versus moderate/heavy smokers. Most smokers intended to quit smoking within the next 6 months (68%, n = 23).
All four culture types were associated with workplace health climate in bivariate analysis (P = .000 to P = .026) (results not shown). After adjusting for several organizational characteristics, only clan culture remained significantly associated with health climate (Table 2). Providing support for HP1, an increase in clan culture was associated with a better workplace health climate (b = 0.27, P = .046).
Linear regression predicting workplace health climate (n = 62).

P < .05; **P < .01; ***P < .001.
Workplace health climate was not associated with smoking status in bivariate analysis (P = .276) (results not shown). However, adjusting for several organizational- and individual-level characteristics revealed a significant association (Table 3). Providing support for HP2, a better workplace health climate was associated with lower odds of being a current smoker (odds ratio [OR] = 0.08; 95% CI: 0.01, 0.53). A significant association also existed between organizational culture and smoking status, with employees working at places with stronger adhocracy and hierarchical cultures more likely to be current smokers (OR = 11.39; 95% CI: 2.08, 62.24 and OR = 5.42, 95% CI: 1.18, 24.82, respectively).
Multivariate mixed-effects logistic regression on smoking status.
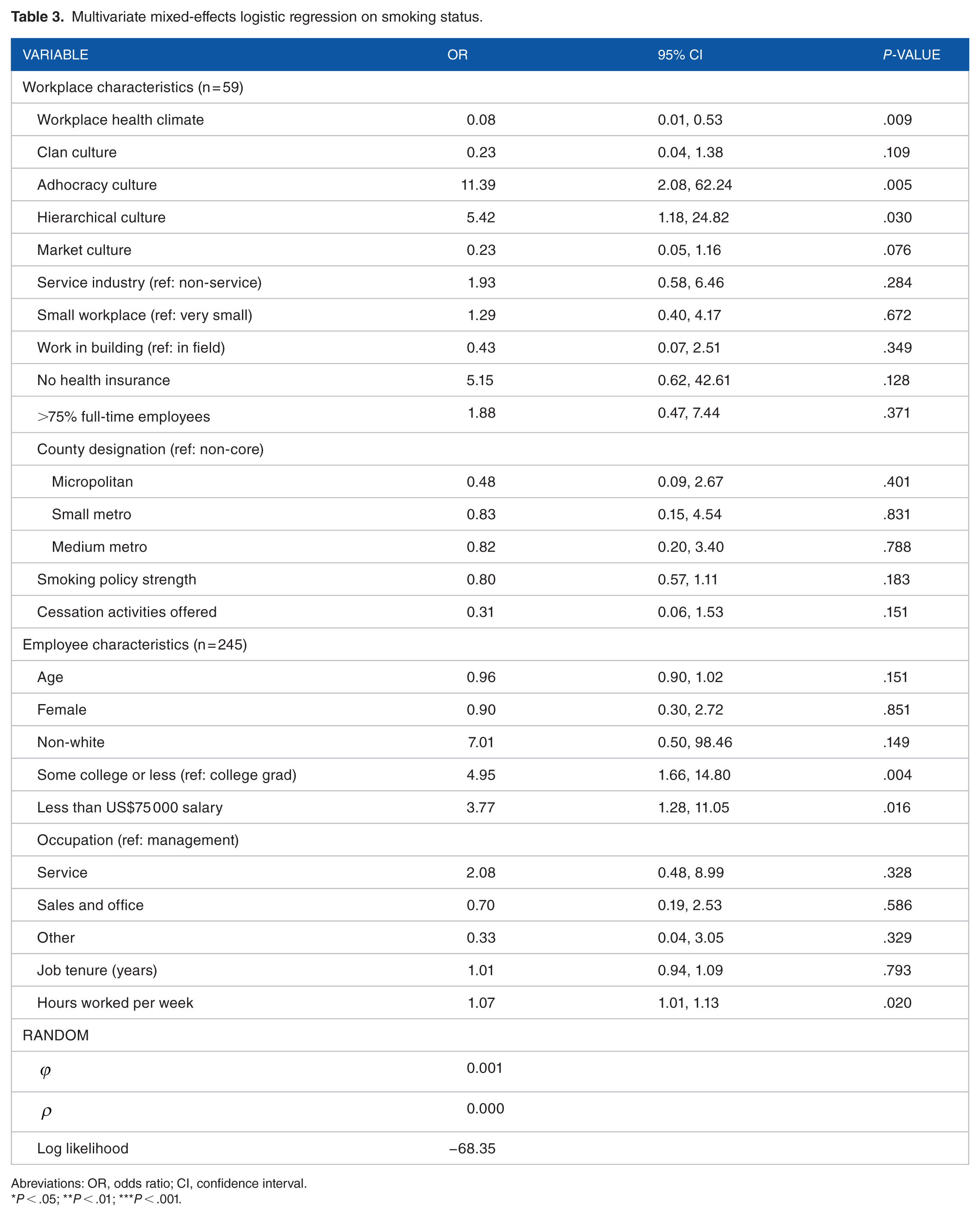
Abreviations: OR, odds ratio; CI, confidence interval.
P < .05; **P < .01; ***P < .001.
Table 4 shows the Fisher’s exact test examining workplace health climate’s relationship to smoking intensity and quit intention. No association existed between workplace health climate and smoking intensity (P = .500). Similarly, we found no association between health climate and intention to quit smoking (P = .316) (Table 5). Therefore, HP3 and HP4 were not supported.
Fisher’s exact test: smoking intensity (n = 34).

P < .05; **P < .01; ***P < .001.
Fisher’s exact test: intention to quit smoking (n = 34).

P < .05; **P < .01; ***P < .001.
Post-hoc analyses
To assess potential differences by workplace size, we ran stratified models for small and very small workplaces. For the linear regression predicting workplace health climate, we found no major differences between the two models. Stratified models for the mixed-effects analysis predicting smoking status revealed a few differences. While relationship directions remained the same, workplace health climate, adhocracy culture, and education showed significant associations for very small workplaces only. Income was significant for small workplaces but not for very small workplaces. We were unable to conduct further tests for workplace size effects due to small sample size and modeling constraints (i.e. the addition of an interaction term to the mixed model was not possible).
Discussion
The purpose of this cross-sectional study was to describe the relationships between organizational culture, workplace health climate, and smoking among employees at smaller workplaces. Previous studies have examined the culture-climate relationship, but few have looked at workplace health climate specifically. This study also examined health climate’s association with employee smoking and contributes important insight into these relationships at smaller workplaces, which have gone understudied.
Consistent with HP1, we found a positive association between clan culture and workplace health climate. This finding is consistent with previous studies showing an association between culture and dimensions of climate12–15 and has been more broadly suggested by others who have described how culture can inform climate.8,9 However, it is important to note here that except for clan culture, no other culture types were significantly associated with health climate. This could mean that there are characteristics salient in clan culture that facilitates a healthy work environment. For example, shared values, concern for others, and a strong organizational commitment to employees exemplify this culture type. 11 These characteristics may translate into greater concern for employee well-being and stronger encouragement to improve health.
Consistent with HP2, we found an association between workplace health climate and smoking status. However, health climate was not associated with smoking intensity (HP3) or quit intention (HP4). These findings may seem counterintuitive, especially for quit intention. Presumably, a smaller percentage of current smokers exist within organizations where quit intentions are higher (i.e. those who intend to quit go on to be non-smokers). However, intentions do not always lead to behavior change, with effect sizes for these relationships medium at best. 44 Furthermore, smoking intensity and quit intention both focus on the behavior and intentions of employees already existing within an organization. In the case of smoking status, it could be that smokers are less inclined to work for companies with strong health climates, or that companies with a health focus are less likely to hire smokers. In these cases, having a strong health climate may not be sufficient to produce actual changes in employee smoking behavior.
Limitations
The response rate for this study was low; therefore, our findings may not accurately reflect the general population of small worksites and their employees. For example, the worksites that chose to participate may be more engaged in health promotion or have a stronger interest in tobacco control. Similarly, most employees who participated in this study were college graduates (63%), 50% made at least US$75 000 a year, and approximately 40% worked in management, professional, or related positions. This population may differ from less-educated or blue collar workers, who have noted disparities in smoking behavior. 45 Given the small sample size for current smokers (n = 34), our subsample analyses assessing health climate’s relationship to smoking intensity and quit intention were limited in scope. Specifically, we did not adjust for characteristics that might influence these relationships and used a dichotomous measure for health climate, resulting in a loss of statistical power. Despite these limitations, this study provides valuable and needed information on the relationship between organizational characteristics and smoking behavior and is likely relevant to smaller workplaces with similar contexts.
Implications for practice and research
Practitioners working to reduce smoking in the workplace should consider how culture and climate influence behavior, and if necessary, collaborate with organizations to intervene upon these factors. Culture change efforts involve a diagnosis of current and preferred culture types, followed by the development of an action plan for change. 11 Given clan culture’s positive association with workplace health climate, efforts to strengthen this culture type within an organization could include placing a greater emphasis on employee support and involvement in the workplace. 11 Strategies to decrease adhocracy culture, which was associated with a significant increase in current smoking odds, could include eliminating unnecessary rules or procedures. 11 To better prioritize and tailor organization change strategies, additional research is first needed to elucidate the specific characteristics within these culture types that are important to workplace health promotion and employee health behavior.
Strategies to increase the workplace health climate might involve stricter enforcement of tobacco-related policies or enhancing supervisor encouragement for cessation. To help facilitate change in smoking behavior and intention, worksites should focus on implementing evidence-based tobacco control initiatives such as smoke-free policies and improved access to quitline. 46 While 68% of current smokers in our study intended to quit smoking within the next 6 months, only 23% of worksites offered smoking cessation activities to help employees quit. These data suggest a continued need to focus on smaller worksites for tobacco control and is consistent with previous studies that have found low rates of health promotion program adoption among smaller worksites. 47
Future research should examine differences by workplace size, as post-hoc analyses revealed here that some factors affect very small but not small workplaces and vice versa. However, these findings should be interpreted with caution given the limitations of this analysis, namely very small sample sizes. Conducting this analysis among a larger sample of workplaces, or collecting more in-depth qualitative data on health climate within smaller workplace settings, would provide more robust data to better understand the nature of these relationships.
Future studies should also explore whether workplace health climate mediates the relationship between organizational culture and smoking behavior. This study was not powered to detect mediation effects, but the relationships between culture, health climate, and smoking status found here suggest that climate could serve as an important mediator. We look forward to future studies powered to explore these characteristics, as they will further extend our understanding of relevant factors important to tobacco control at smaller workplaces.
Conclusions
Smoking can lead to several health and economic consequences, making it important to understand factors that can reduce the negative impact of this behavior. The findings from this study suggest that organizational culture and workplace health climate affect smoking outcomes among employees at smaller workplaces. However, this may not be universally true—associations between culture, health climate, and smoking were only found for certain culture types and for certain smoking outcomes. It is important to have a full understanding of these worksite characteristics when developing tobacco control initiatives to protect employees from the harmful effects of smoking.
Footnotes
Funding:
This publication was supported by the Centers for Disease Control and Prevention (cooperative agreement no.: 1 U48 DP005021-01). The findings and conclusions of this journal article are those of the author(s) and do not necessarily represent the official position of the Centers for Disease Control and Prevention. This work was also supported by the University of Iowa Graduate & Professional Student Government student research grant and an Advancing Graduate Student Success Award from the College of Public Health, The University of Iowa.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author’s Note
Dr. Baquero is also affiliated to the Health Promotion Research Center at the University of Washington.
Author Contributions
CMK and EAP contributed significantly to study conception and design. CMK collected and analyzed study data and wrote the first draft of the manuscript. EAP, BB, SJC, PAG, MS, and DKS critically revised and reviewed the manuscript. All authors read and approved the final manuscript.