
Abstract
Background:
Numerous studies have reported that shorter time to first cigarette (TTFC) is linked to elevated risk for smoking-related morbidity. However, little is known about the influence of early TTFC on self-reported health among current smokers. Hence, the objective of this study was to examine the association between TTFC and self-reported health among US adult smokers.
Methods:
Data came from the 2012-2013 National Adult Tobacco Survey (NATS). Current smokers aged 18 years and older (N = 3323) were categorized into 2 groups based on TTFC: ≤ 5 minutes (n = 1066) and >5 minutes (n = 2257). Propensity score matching (PSM) was used to control selection bias.
Results:
After adjusting for sociodemographic and smoking behavior factors, current smokers with early TTFC had higher odds for poor health in comparison with current smokers with late TTFC in the prematching (adjusted odds ratio [AOR] = 1.65; 95% confidence interval [CI] = 1.31-2.08) and postmatching (AOR = 1.60; 95% CI = 1.22-2.09) samples.
Conclusions:
In conclusion, smokers with early TTFC were associated with increased risk of poor health in the United States. To reduce early TTFC, elaborate efforts are needed to educate people about harms of early TTFC and benefits of stopping early TTFC.
Introduction
Smoking is one of the major behavioral contributors to preventable cause of death worldwide, 1 resulting in 4 million deaths a year with estimates projected at 10 million by the late 2020s. 2 Even though the smoking rate among US population over the age of 15 has consistently decreased from 1998 to 2013, 13.7% of this population was still current smokers in 2013 (Figure 1). 3

Smoking trend for US adults (over 15) 1998-2013.
Most smokers who want to quit smoking have little probability of long-term success due to nicotine dependence and withdrawal symptoms. 4 Many research studies have reported that the time to first cigarette (TTFC) of the day is one of the strongest indicators of nicotine dependence.5–8 Nicotine addiction can be analyzed through the Fagerstrom Test for Nicotine Dependence (FTND). 9 Time to first cigarette is one of the 6 measures of the FTND.10–12 Furthermore, shorter TTFC is considered a risk factor for smoking-related morbidity. Recent studies on the relationship between chronic obstructive pulmonary disease (COPD) and TTFC have reported that a shorter TTFC associates with an increased risk of COPD.13–15 Research studies on the association between hypertension and TTFC have reported that blood pressure is generally increased on waking,16,17 and the nicotine in tobacco can elevate blood pressure by approximately 10 to 15 mm Hg for about 30 minutes.18–22 Hence, a shorter TTFC after waking can lead to a morning elevation of blood pressure. Smokers who smoke a cigarette as soon as they get up could experience sharp blood pressure changes that bring about blood vessel damage and accelerated atherosclerosis.16,23–25 Also, some research studies have reported that a shorter TTFC is related to increased risk of smoking-related cancers26–30 and high blood cholesterol levels that might lead to cardiovascular disease. 31 Even though self-reported health is considered a significant predictor of morbidity and quality of life, 32 little is known about the influence of TTFC on self-reported health among current smokers. Hence, we need more research on this issue from a disease prevention perspective. For this reason, the objective of this study was to examine the association between TTFC and self-reported health among US adult smokers. This research study was an observational study using secondary survey data. Compared with experimental studies, observational studies are susceptible to selection bias.33,34 To identify a more robust measure of the association between TTFC and self-reported health, propensity score matching (PSM) is applied in the study.
Methods
Procedure and participants
This study used data from the 2012-2013 National Adult Tobacco Survey (NATS) (N = 60 192). The NATS is a nationally representative survey for collecting data about tobacco use among US adult aged 18 years and older. The NATS was created to evaluate the prevalence of tobacco use, as well as the factors promoting and impeding tobacco use among adults. The NATS was designed as a stratified, national, landline, and cell phone survey of noninstitutionalized adults aged 18 years and older residing in the 50 states or DC. It was developed to yield data representative and comparable at both national and state levels. The sample design also aims to provide national estimates for subgroups defined by sex, age, and race/ethnicity. 35 This study did not require approval from the institutional review board because the NATS data are secondary data that do not include personal information.
Measures
Time to first cigarette
Previous studies have reported that early TTFC (≤5 minutes) was associated with increased risk of smoking-related morbidity and higher cotinine level.13,28,36,37 Therefore, TTFC variable was converted to a binary index variable (>5 minutes:0, ≤5 minutes: 1) based on responses to the following item: minutes after waking up to first use cigarette/cigars.
Self-reported health
Self-reported health variable was categorized into 5 groups (excellent, very good, good, fair, poor) in data set. This variable was converted to a binary index variable (treatment group = poor, control group = ≥fair), based on responses to the following item: Would you say that in general your health is?
Covariates: sociodemographic variables
Sex was categorized into 2 groups (male and female). Age was categorized into 2 groups (18-39 and 40+). Race was categorized into 2 groups (white and non-white). The education level was categorized into 4 groups (<high school diploma; high school diploma; some college, no degree, post high school certificate or diploma; and bachelor’s degree, master, professional, or doctoral degree). The household income level was categorized into 4 groups (<US $20 000, US $20 000-US $39 999, US $40 000-US $69 999, ≥US $70 000).
Covariate: smoking behavior variable
There is no formal category and guideline that defines a light or heavy smoker now. Amount of smoking per day was categorized into 2 groups (>10 cigarettes a day and ≤10 cigarettes a day).
Statistical Analysis
Descriptive statistics
Descriptive statistics with χ2 test (Table 2) and dot chart (Figure 4) was presented to summarize the data. Statistical analysis was conducted using STATA (version 15.0; StataCorp LLC., College Station, TX, USA).
Propensity score matching
Propensity score matching was first suggested by Rosenbaum and Rubin in 1983. This statistical method is based on a counterfactual concept and can help reinforce causal arguments in observational studies by reducing selection bias.38,39 The propensity score is a balancing score and can be estimated using logistic regression if missing values are deleted in covariates. 40 First, TTFC (>5 minutes: 0, ≤5 minutes: 1) was used as dependent variable and sociodemographic/smoking behavior variables (sex, age, race, education level, household income level, amount of smoking per day) were used as covariates in PSM. Second, treatment case (≤5 minutes) is matched with control case (>5 minutes) using 1:1 nearest neighborhood matching. Finally, relative multivariate imbalance test and covariates difference analysis were performed after PSM to check the effect of matching. Statistical analysis was conducted using SPSS (version 23.0; SPSS Inc., Chicago, IL, USA).
Multivariate logistic regression
Multivariate logistic regression was performed to examine the association between TTFC and self-reported health among US adult smokers before and after PSM. Independent variable was TTFC and dependent variable was self-reported health. Sociodemographic/smoking behavior variables including sex, age, race, household income, education, and amount of smoking per day were used as covariates in logistic regression model. The first logistic regression model was generated based on the full sample (prematching sample) of US adult smokers (over 18). After PSM, the second logistic regression model was generated based on the reduced sample (postmatching sample) containing only those cases included in the matches (Figure 2). Statistical analysis was conducted using STATA (version 15.0; StataCorp LLC.).
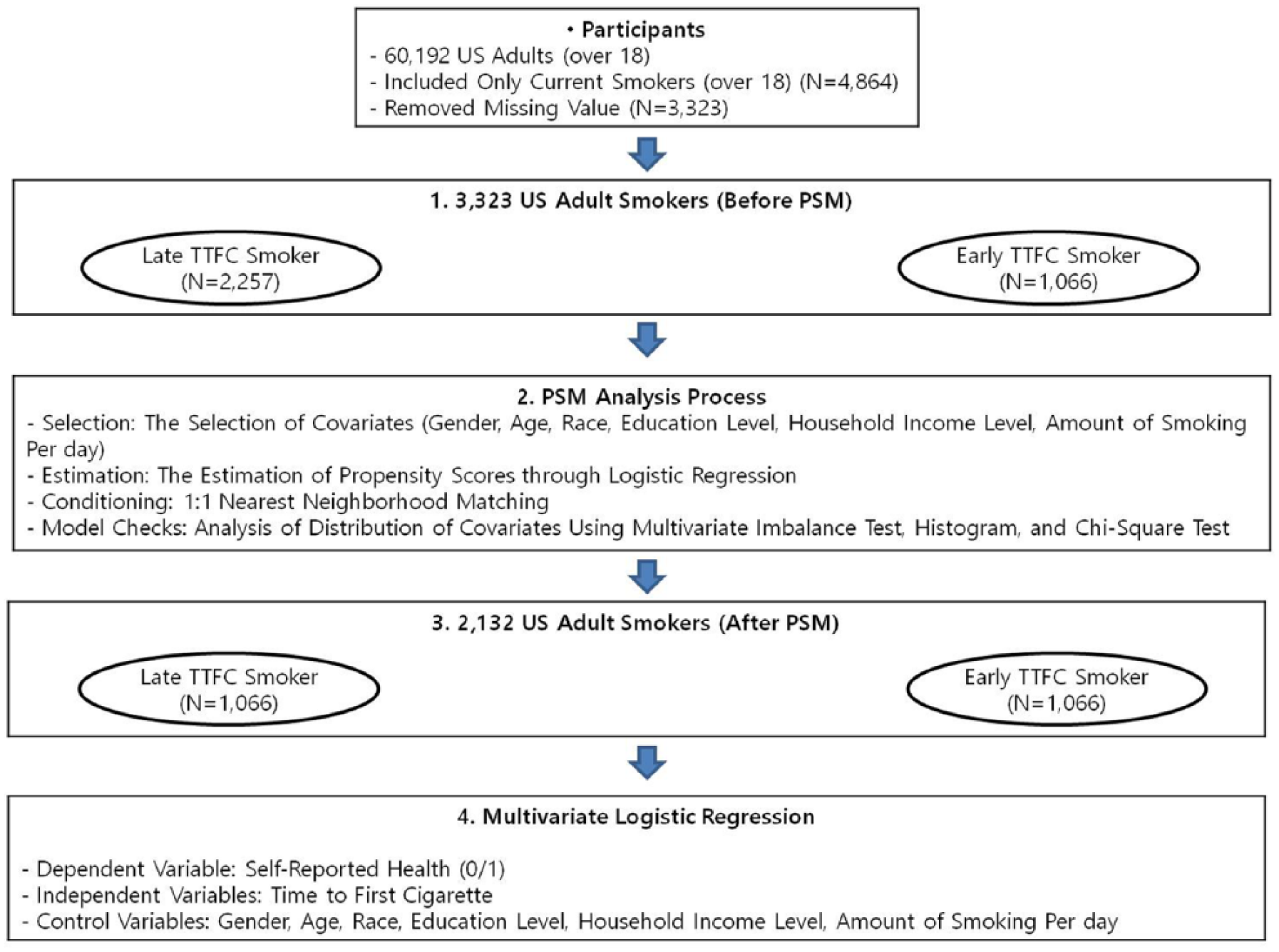
Sample flow diagram: National Adult Tobacco Survey (2012-2013).
Results
Table 1 shows the results of relative multivariate imbalance test before and after matching. Matching leads to identical multivariate distributions as we get multivariate imbalance measure closer to 0 after matching. 41
Relative multivariate imbalance test.
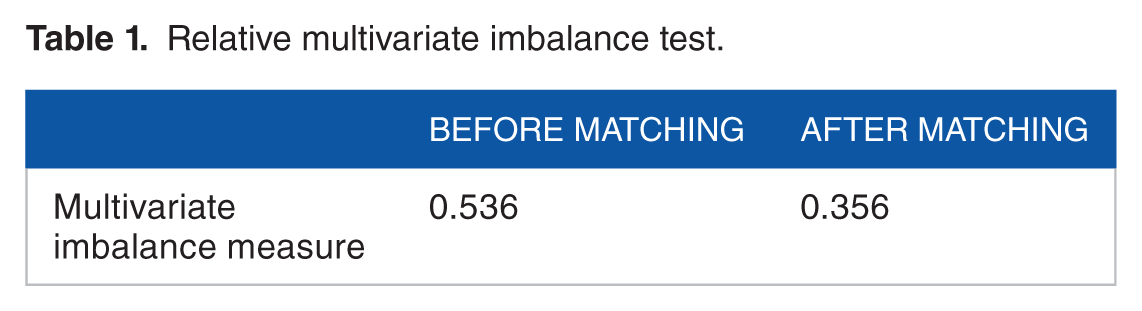
First, multivariate imbalance measure is 0.536 which means only 46.4% of the density of the 2 histograms (unmatched) in Figure 3 overlap before matching. Second, multivariate imbalance measure is 0.356 which means 64.4% of the density of the 2 histograms (matched) in Figure 3 overlap after matching. According to Figure 3, also, the histograms before matching on the left differ to some degree. In contrast, the histograms after matching on the right are relatively similar. Hence, both Table 1 and Figure 3 show that matching worked relatively well. 41

Histograms of propensity score before and after matching.
Figure 4 displays the dot chart of the association between mean of TTFC and self-reported health. As shown in Figure 4, participants with ≥fair self-reported health had late TTFC than those who with poor self-reported health (17.54 minutes versus 14.01 minutes).

Dot chart of the association between mean of time to first cigarette (TTFC) and self-reported health among US adult smokers.
Table 2 shows the descriptive statistics of current smokers with early TTFC and current smokers with late TTFC before and after matching. In the prematching sample, there were significant differences between samples of early TTFC and late TTFC for each of the covariates. In the postmatching sample, there were no longer significant differences on all observed covariates between early TTFC and late TTFC, as shown by the smaller number of variables and larger P value for χ2 test.
Descriptive statistics of covariate imbalance before and after matching on the propensity score.

Table 3 shows the results of the multivariate logistic regression that determined the association between TTFC and self-reported health status among US adult smokers in the large (prematching) and small (postmatching) samples. The analysis using the prematching sample identified a significant association (adjusted odds ratio [AOR] = 1.65, P < .001) between early TTFC and poor health among US adult smokers after adjusting for sociodemographic and smoking behavior variables in the model. The prematching analysis also showed significant associations between poor health and the following covariates: sex, age, education level, and household income level.
Multivariate logistic regression models of the association between time to first cigarette (TTFC) and poor health among US adult smokers.
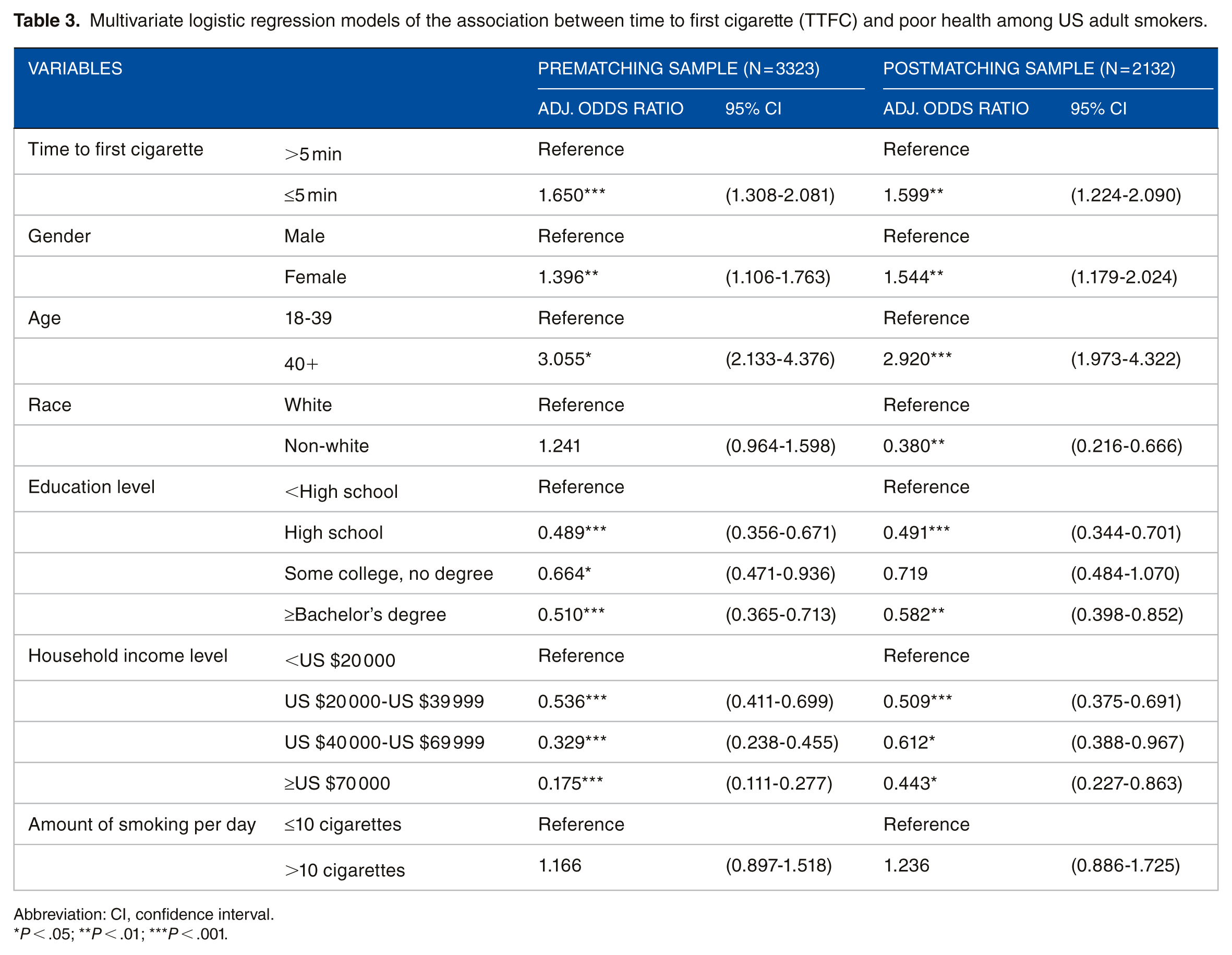
Abbreviation: CI, confidence interval.
P < .05; **P < .01; ***P < .001.
Table 3 also displays the association between TTFC and self-reported health among US adult smokers in a small (postmatching) samples determined through PSM using the 1:1 nearest neighborhood matching. After adjusting for all covariates in the model, early TTFC remained a significant predictor (AOR = 1.60, P < .01) of poor health among US adult smokers. The postmatching analysis also showed significant associations between poor health and the following covariates: sex, age, race, education level, and household income level.
Discussion
This study used PSM to analyze the association between TTFC and self-reported health among US adult smokers. This study results revealed that compared with current smokers with a late TTFC (>5 minutes), those who with an early TTFC (≤5 minutes) were associated with increased risk of poor health. The association was statistically significant even after adjustment for sociodemographic and smoking behavior variables including sex, age, race, education level, household income level, and amount of smoking per day. Numerous previous research studies reported that shorter TTFC is considered a risk factor for smoking-related morbidity such as COPD,13–15 hypertension,16,23–25,42 smoking-related cancers,26–30 and high blood cholesterol level. 31 This study found that shorter TTFC is also associated with increased risk of poor self-reported health. Self-reported health status is a significant indicator of morbidity and has been turned out to be a stronger predictor of quality of life outcomes than other measures of morbidity. 32 Gathering self-reports is more cost-effective and it can potentially be more perfect than a medical record review. 43 Hence, poor self-reported health status among current smokers with early TTFC can be a useful predictor for smoking-related morbidity. There are several feasible mechanisms through which shorter TTFC increases risk of poor health. The early TTFC smokers may have inhaled more deeply and promptly to make up for nicotine insufficiency in the morning immediately after getting up and this behavior can be severely influence the cardiovascular system.19,44 Also, blood pressure is generally elevated on waking16,17 and cigarette smoking can be independently associated with hypertension.18–22 Early TTFC-related high blood pressure may induce blood vessel damage that can be lead to increased risk of atherosclerosis, cerebrovascular disease, and cardiovascular disease.16,23–25,42 Therefore, the early TTFC smokers with poor self-reported health should be encouraged to quit smoking. However, most smokers who want to quit smoking have little chance of long-term success due to nicotine dependence and withdrawal symptoms such as depression, nicotine dependence, and irritability. 4 If quitting smoking in a short period of time is difficult for them, they should be educated to postpone lighting their first morning cigarette. Carefully designed late TTFC guideline or mass media campaigns that highlight the benefits of stopping early TTFC may contribute to the reduced early TTFC among current smokers.
Results of this study should be considered in light of several limitations. First, although this study used PSM to control selection bias; there were still biases in the study. This is because it is impossible to eliminate all biases that potentially may have been introduced by confounders that were not measured in the 2012-2013 NATS. Second, the temporal causal relationship between TTFC and self-reported health cannot be determined because the study design is cross-sectional. Therefore, follow-up studies using prospective longitudinal and randomized controlled research design need to verify the findings of this study. Third, this study only included amount of smoking per day as a smoking behavior covariate, excluding other smoking behavior variables because of a number of missing values. Finally, this study could not apply weighting adjustment method to data analyses.
Conclusions
Despite the above limitations, this study demonstrated the worth of identifying the association between early TTFC and poor health among US adult smokers. Also, this finding provides clinical implications to prevent smoking-related morbidity among early TTFC smokers. Methodologically, this study is significant in the sense that it was a first attempt to apply PSM to analyze the association between TTFC and self-reported health among US adult smokers. The PSM method employed in this study yielded a more accurate estimate of the effects of early TTFC on poor health. In conclusion, smokers with early TTFC were associated with elevated risk of poor health in the United States. Although the US government raises about US $25.8 billion a year in cigarette taxes from smokers, 45 the total economic costs of cigarette smoking in the United States is about US $300 billion a year including about US $170 billion in direct treatment costs and about US $156 billion in reduced productivity due to poor health and premature death. 46 In consideration of the social and health implications of early TTFC, public health authorities need to increase their efforts to reduce early TTFC among US adult smokers.
Footnotes
Acknowledgements
The author would like to thank officials from the CDC for help with data collection.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All of manuscript contents were made by BS. Conceived and designed the study: BS. Analyzed the data: BS. Wrote the first draft of the manuscript: BS. Made critical revisions: BS. The author reviewed and approved of the final manuscript.