
Abstract
Background:
Tobacco smoking is a growing concern for health care systems as it is projected to become the leading cause of death in the developing world. Knowledge of how smoking behavior differs across socioeconomic groups is crucial for designing effective preventive policies and alleviating the disparities. The aim of this study was to report the prevalence of (1) smoking status, (2) early smoking initiation, and (3) association with socioeconomic status (SES) of the 2 among Malawian men.
Methods:
Cross-sectional data on 1693 men aged between 15 and 49 years were collected from the latest 2013-2014 Multiple Indicator Cluster Survey in Malawi. Educational qualification and wealth index quintile were used as the indicators of SES. Outcome variables were smoking status, first age of smoking being below 18 years, and ever using any form of smokeless tobacco products. Multiple logistic regression models were used to see the contribution of SES to smoking status and early smoking initiation.
Results:
Mean age of the sample population was 33.23 years (SD: 8.25). Prevalence of smoking, early initiation, and ever using any form of smokeless tobacco were, respectively, 46.6%, 33.7%, and 6%. Compared with men who had higher education, those who had no formal education, primary-level, and secondary-level qualification had, respectively, 21% (adjusted odds ratio [AOR] = 1.209; 95% confidence interval [CI] = 0.498-2.935), 40% (AOR = 1.4; 95% CI = 0.647-3.029), and 26% (AOR = 1.256; 95% CI = 0.593-2.661) higher odds of being a smoker. Those who had no formal education were 2.7 times (AOR = 2.734; 95% CI = 1.123-6.653) as likely to try smoking before reaching 18 years of age. Compared with the richest, those in the lowest wealth quintile had 32% lower odds (AOR = 0.676; 95% CI = 0.455-1.006) of early onset of smoking, 63% lower odds (AOR = 0.372; 95% CI = 0.201-0.690) of trying other tobacco products.
Conclusions:
Addressing the socioeconomic disparities could play a vital role in delaying early onset and limiting overall consumption of tobacco. Ongoing health policy talks to reduce the prevalence of smoking should take into consideration improving educational and material well-being among men.
Background
Tobacco is a prominent cause of avoidable illnesses and premature death across many countries. Intake of tobacco and secondhand smoking are known age-old risk factors of respiratory and cardiovascular diseases and other health problems including cancer,1,2 although the degree of the effect according to the level of involvement vary widely among smokers. Almost 1 billion men and 250 million women worldwide have been reported to be involved in smoking. 3
Overall, smoking is a prominent factor of health problems among adolescents, youth, and adults alike due to the effect of monoxide, tar, nicotine, and other toxic substances contained in cigar, pipe, cigarette, or tobacco.4,5 It is known that about 33% of smokers who had early initiation are susceptible to smoking-related sicknesses, such as cardiovascular diseases and lung cancer, leading to death. 6 Initiation into smoking at early age has immense negative influence on the practice or attitude of smoking at later stage in life. 7 Studies have shown that people who had early initiation into smoking are more likely to continue the habit after adolescence.7,8 Furthermore, reduced level of successful cessation in the habit of smoking among adult is correlated with early smoking initiation. Adults who start smoking at early adolescence are twice likely to grow into heavy smokers and have less ability to quit smoking at older age than those who have late involvement in smoking. 9 Thus, it is of top priority that public health programs seize the problem of early smoking initiation, specifically among young adolescents as well as strategize to terminate the practice of smoking.
Hitherto, several studies on early smoking initiation have examined its associations with behavioral, socioeconomic (SE), demographic, and environmental factors.10–12 Nevertheless, the effect of these associated predictors varied across socio-demographic groups due to diverse impact of cultural and social settings related to their perceptions about the attitude of smoking. 13
In contrast to high-income countries with improved access to health facilities and economic development, use of tobacco at early age is on the increase and becoming more prevalent in developing countries. 14 It has been influenced by numerous factors; among them, SE factors are key predictors of smoking lifestyle. In developed countries, several studies on smoking and SE inequalities have been conducted, and the results imply that people from lower SE status (SES) using education, wealth index, and other SES indicators are more prone to smoking.15–18 Knowledge of SE disparity in smoking over time with various degrees of tobacco use is paramount for public health research.
Numerous reports gave the link between SES and the use of tobacco among different cohorts over time. Vedoy 19 revealed that the odds of regular use of tobacco reduced across cohorts having higher education compared with less educated class in conformity with the data in Norway for the years 1976 through 2010. Conversely, it was reported in a study involving Americans that there were variations in the degree of smoking across SES for cohorts investigated. Researchers obtained the association between SES and the use of tobacco, particularly among younger groups, whereby high SE class had less involvement in smoking vis-à-vis low SES had high use of tobacco.20,21 Increased incidence of smoking among adolescents and adults of low SES begins with increased early smoking initiation.22–25
Countries such as Malawi, Zimbabwe, and Tanzania that cultivate tobacco experience more challenges. It is a complex task to make a case for health and against the use of tobacco when the crop promotes the sustainability of the country. For example, Malawi obtains more than 60% of her share of total exports on tobacco, parting some to claim that cultivating tobacco is in the nation’s top economic and social interest.26,27 Government and stakeholders of health are participating in the cultivation of tobacco and have a venture in the success of the crop.27,28 Hence, early smoking initiation and SE disparities in the use of tobacco become interesting to research in Malawi.
This study examined prevalence and predictors of early smoking initiation and SE inequalities in smoking behaviors using nationally representative data. More so, prevalence of smokers, people who started smoking early in life (first smoking before 18 years) and use of other tobacco products were evaluated by socio-demographic predictors from the data previously collected in nationwide survey in Malawi.
Methods
Ethical considerations
Approval for this study was not required because the data are secondary and are available in the public domain. More details regarding Multiple Indicator Cluster Survey (MICS) data and ethical standards are available at the following Web site: https://www.unicef.org/statistics/index_24302.html.
Survey and data collection
The study is based on secondary data from the latest (fifth round) MICS in Malawi 2013-2014, which was conducted by the National Statistical Office (NSO), Malawi. The MICS program developed by United Nations Children’s Fund (UNICEF) is global initiative, which started the mission in 1990s and is operational in more than 100 countries. Multiple Indicator Cluster Survey is a household survey program that aims to provide internationally comparable data on various health and socio-demographic indicators. The outcomes of the surveys have also proved instrumental in monitoring progress toward the Millennium Development Goals and developing health policies and programs to meet the internationally agreed commitments by the participating nations.
Multiple Indicator Cluster Survey employs a multistage cluster-sampling strategy to select country representative samples. The sample encompassed Northern, Central, and Southern regions including both urban and rural areas across 27 districts in the country (excluding Likoma). For the Malawi survey, questionnaires were based on the MICS 5 model questionnaire in English, which were customized and translated into Chichewa and Tumbuka. Questionnaires were pretested and were modified based on the pretest results. The fieldwork lasted from November 2013 till April of the next year. The Malawi 2013-2014 survey initially selected 7818 men aged between 15 and 49 years, of which 6842 were successfully interviewed with a response rate of 87.5%. Further details regarding the survey are published elsewhere.29,30
Variables
Outcomes variables were current smoking status, age of initiation of smoking, and smoking products other than tobacco. Participants were asked whether they ever tried tobacco and alcohol and could answer—Yes/No. Main explanatory variables were (1) educational attainment (none/primary/secondary/higher) and (2) wealth index quintile (poorest/second/middle/fourth/richest).
The following covariates were included in the analysis as potential confounders: age: 15 to 19/20 to 24/25 to 29/30 to 34/35 to 39/40 to 44/45 to 49 years; region: Northern/Central/Southern; religion: Christian/Islam/Other; frequency of listening to radio: almost every day/at least once a week/less than once a week/not at all; frequency of watching TV: almost every day/at least once a week/less than once a week/not at all.
Data analysis
The data set was checked for potential outliers and was cleaned for missing values and was weighted before analysis. Frequencies tables described basic socio-demographic characteristics. Prevalence of smoking, early initiation, and the group differences (smoking vs not smoking, age of onset: <18 vs 18/18+ years, smoking vs not smoking other tobacco products) were calculated by cross-tabulation. The χ2 bivariate tests were performed for statistical significance with smoking status and the explanatory variables. The variables which were significant at P < .05 were selected for the multivariate analysis. Finally, multivariable regression was performed to calculate the odds ratios of the associations of smoking, early initiation, and trying other tobacco products. Three separate regression models were run for the 3 outcomes variables. A 2-tailed P value of <.05 was considered statistically significant for all associations. All analyses were performed using SPSS V.21.
Results
Basic sample characteristics are shown in Table 1. Mean age of the respondents was 33.23 (SD: 8.25) years. Results showed that most of the participants were between 30 and 34 years of age, residents of the central region (45.1%), and practiced Christian faith (82.0%). Frequency of following radio and TV was, respectively, 41.7% and 11.5%. About three-fifth had primary-level educational qualification and 8.2% had no formal education. One-fifth of the participants belong to the lowest and 23.3% to the highest wealth quintile. Close to half the men reported smoking (46.6), one-third reported smoking first time before reaching 18 years, and 6% reported ever trying any form of smokeless tobacco products.
Frequency distribution of sample characteristics, Malawi Multiple Indicator Cluster Survey (MICS) 2013-2014.

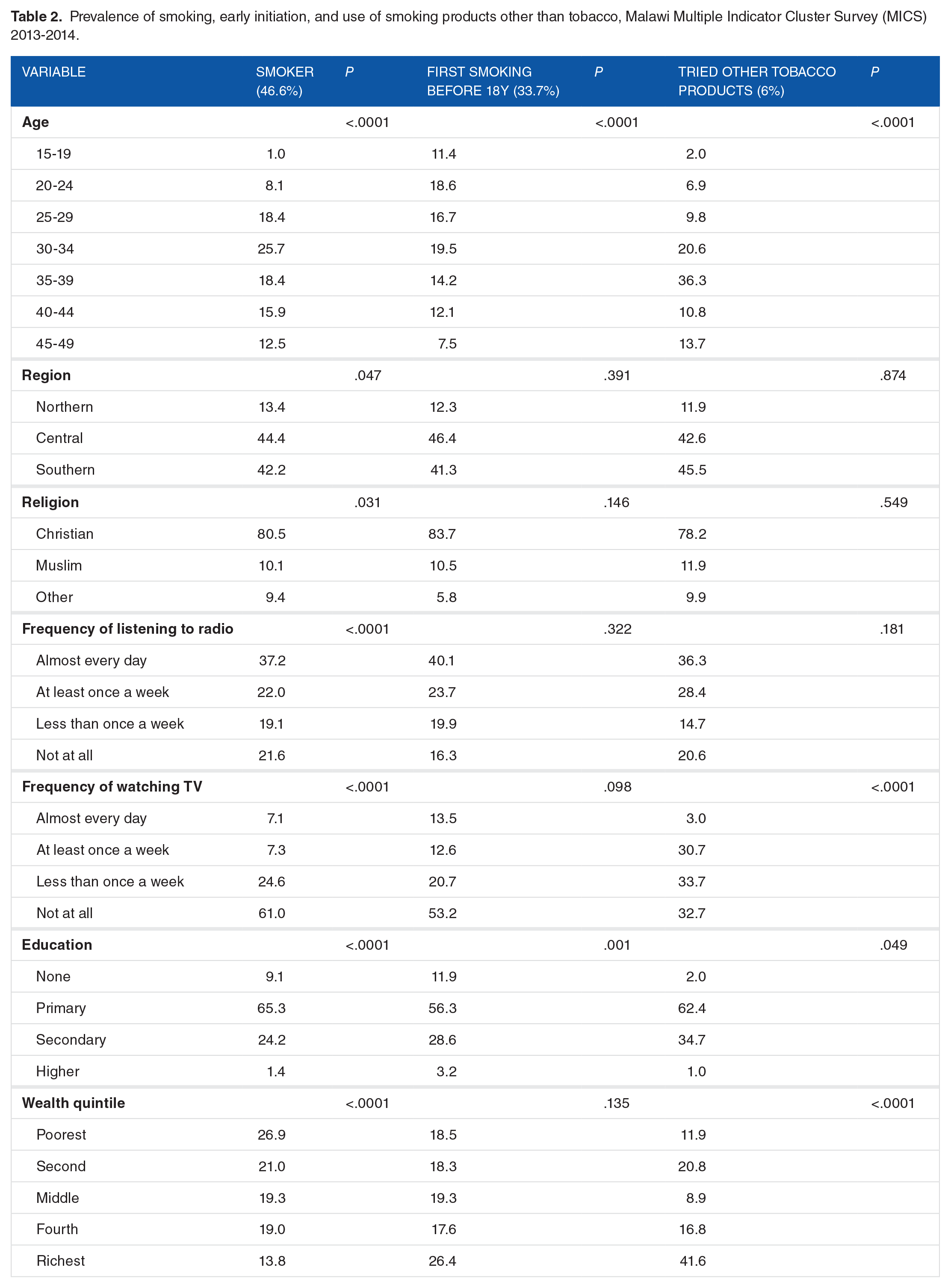
Results of χ2 tests of association in Table 2 indicate that all the explanatory variables were significantly associated with smoking status. However, for early initiation of smoking, region, religion, listening to radio, and wealth status did not show any significant association. For the use of other tobacco products, significant association was observed with age, frequency of watching TV, educational attainment, and wealth quintile.
Prevalence of smoking, early initiation, and use of smoking products other than tobacco, Malawi Multiple Indicator Cluster Survey (MICS) 2013-2014.
Results of multivariable analysis on the association between education and wealth status with smoking patterns are presented in Table 3. Findings indicate that compared with men who had higher education, those who had no education, primary-level, and secondary-level qualification had, respectively, 21% (adjusted odds ratio [AOR] = 1.209; 95% confidence interval [CI] = 0.498-2.935), 40% (AOR = 1.4; 95% CI = 0.647-3.029), and 26% (AOR = 1.256; 95% CI = 0.593-2.661) increase in the odds of being a smoker. Those who had no education were 2.7 times (AOR = 2.734; 95% CI = 1.123-6.653) as likely to try smoking before reaching 18 years of age. The odds of trying other tobacco products were, respectively, 1.7 times (AOR = 1.704; 95% CI = 0.079-36.862), 9.9 times (AOR = 9.947; 95% CI = 0.967-102.304), and 13.4 times (AOR = 13.382; 95% CI = 1.247-143.57) higher among those who had no education, primary-level, and secondary-level qualification.
Association between education and wealth status with smoking patterns, Malawi Multiple Indicator Cluster Survey (MICS) 2013-2014.

Abbreviations: AOR, adjusted odds ratio; CI, confidence interval.
Adjusted for age—region, religion, frequency of listening to the radio, frequency of watching TV, education, wealth index quintile.
Adjusted for age—religion, frequency of watching TV, education, wealth index quintile.
Adjusted for age—frequency of listening to the radio, frequency of watching TV, education, wealth index quintile.
Significant variation in smoking status was observed across the 5 wealth groups. Compared with men in the highest wealth quintile, those in the lower quintiles had a declining likelihood of being a smoker: 3.9 times, 2.2 times, 2.1 times, and 1.9 times for fourth, middle, second, and lowest quintiles, respectively. Belonging to the lower than richest wealth quintile also reduced the likelihood of early onset of smoking and trying other tobacco products. Those in the lowest wealth quintile had the lowest odds (83% lower compared with the richest) of smoking before reaching 18 years of age, and those in the second lowest wealth quintile had the lowest odds (33% lower compared with the richest) of trying other tobacco products.
Discussion
The findings of the study indicate that education and wealth status were significantly associated with smoking patterns.
All the 3 groups, ie, those with no education, those with primary level of education, and those with secondary level of education had higher odds of being smokers compared with those with higher education. The findings are consistent with previous studies.31 –33 One study for example found that the annual reduction in smoking prevalence was 5 times higher among the most educated compared with those with lesser education. The study also concluded that the number of pack years smoked was higher in those individuals with less than high-school level of education. 31 It should be noted that the findings were not consistent across these 3 groups. So, for example, those with primary level and secondary level of education were relatively more likely to be smokers compared with those with no education. This finding is in line with a previous study which has concluded that the relationship between education and smoking is not monotonic. The study has recommended to categorize education as per the number of years of education. 32 This, however, was beyond the scope of this study.
More so, educational attainment has been of major interest to researchers as a key factor in many health-related problems including the practice of smoking. Several authors have analyzed relationships between early smoking initiation and the education of the people. In line with the reports from previous studies, early smoking initiation was found to be correlated with educational attainment of respondents. Lack of formal education was a dominant factor influencing early smoking initiation.21,34,35 Also, the use of other tobacco products such as the smokeless tobacco was found to be higher among participants of lower educational status.
In terms of wealth index, consistently higher wealth index was associated with higher odds of an individual being a smoker. The findings are consistent with previous studies from some of the countries, for example, the Balkans. In addition, wealth index as one of the indicators of SE characteristics is a dominant factor in many health-related practices. In the assessment of the respondents who currently smoke irrespective of the frequency and those who have used other tobacco products in relation to wealth index, an association was observed. 11 Previous studies have reported that young people with more money have higher degrees of smoking.36,37 Although the contrary has also been reported, saying adolescents from lower SE backgrounds were more likely to smoke. 38 These conflicting reports may suggest, to some extent, different attitudes and beliefs about smoking as well as other environmental and interpersonal predictors. More so, the differences could also be attributed to the 4 stages of tobacco pandemic as discussed by Lopez et al. 39 With nearly 50% of men reporting smoking and with those in the higher wealth quintile being more likely to be smokers, the situation may be akin to the second stage of the tobacco pandemic as discussed by Lopez et al. 39 Based on this study, there might be lack of strategic tobacco control activities as well as lack of political will and support toward tobacco control strategies in Malawi. The policy implications from this could be profound and in line with one of the studies which concluded that reduction in smoking prevalence is inconsistent across geographies, development stage, and sex. The study further emphasized preventing initiation and promoting cessation of smoking through exhaustive and strategic policies requiring greater political commitment. 40
Impact of SE disparities must be considered in early smoking initiation as key factor influencing smoking behaviors or lifestyle. Generally, the trends in smoking prevalence across different age categories are dynamic and reveal a combination of period, cohort effects, and age. However, in most situations, smoking initiation typically ensues during adolescence and its prevalence rises until adulthood. Going beyond that, a decline in smoking occurs with age. This drop with age reveals the collective effect of smokers quitting or smokers dying early over time. The trends across age categories in a country are centered on variations in the rate and age of smoking initiation and the forms of cessation, which vary over time consequent on the interaction between the factors for and against the use of tobacco.8,41
Strengths and Limitations
This study, which was based on the MICS survey of Malawi 2013-2014, is secondary data analysis. The authors were able to examine many variables simultaneously, which could be potential confounders toward the relationship between SE factors and smoking behavior. However, the study has certain limitations. For example, the authors had no control over the type and quality of the data analyzed. Also, even though a significant association was found between wealth status and smoking patterns as well as education and smoking patterns, no causal inference could be drawn from this association. In the absence of a host of confounding variables, such as genetic influences, parental smoking habits, and peer pressure, the study could only have limited inference about the association of these variables with smoking patterns. Also, for the study of education, as recommended in one of the previous studies, the authors were not able to categorize education years to further study the relation between education and smoking, particularly when this relation is not monotonic. It would also have been nice to analyze and incorporate details on the political commitment of the government through variables such as money spent on tobacco control programs or even the intricate details of the tobacco control campaigns and their success rates.
Conclusions and Policy Suggestions
The focus of this study was the relation between SE factors and the prevalence of people who currently smoke, people who had early smoking initiation, and the use of other tobacco products, such as smokeless tobacco, using nationally representative data in Malawi.
Reduction in the use of tobacco is a conquerable battle as we have the science and other exertion and support for evidence-based, cost-effective methods that we can implement to improve on the nation’s health.
The findings in this study provide evidence that can coordinate high-impact interventions and campaigns. Community-level variations protecting citizenry from secondhand smoke and customs are effective in reducing early smoking initiation and high prevalence of smoking among youth. It is a necessity that we continue to invest in tobacco use prevention and control.
As seen in the study, predominant proportions of respondent who currently smoke use other tobacco products or reported ages of initiation into smoking were at late adolescence. This period is usually associated by increased instability and major life options, which include going to school, working or living independent lifestyle, and so forth. As people approach the adulthood, the unhealthy attitude initiated earlier could be abandoned or developed into more consolidated behaviors. Hence, it is paramount to approach promotion of health at this stage.
Footnotes
Acknowledgements
The authors thank the UNICEF for their support and for free access to the original data.
Peer Review:
Three peer reviewers contributed to the peer review report. Reviewers’ reports totaled 275 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
SY and GB participated in the conception and design of the study, data cleaning and analysis, results interpretation, and drafting and revision of the manuscript. SY, GD, VS, and ME participated in the review of statistical methods, results interpretation, and revision of the manuscript. All authors read and approved the final manuscript.
Availability of Data and Materials
Data for this study were sourced from the latest (fifth round) Multiple Indicator Cluster Survey in Malawi 2013-2014 and available online.
Consent for Publication
No consent to publish was needed for this study as we did not use any details, images, or videos related to individual participants. In addition, data used are available in the public domain.