
Abstract
Background:
Garlic, as an additive, a spice, and an ancient herbal medicine, has been proposed as a potential treatment for type 2 diabetes mellitus (T2DM). This systematic review and meta-analysis provides a comprehensive evaluation of the effects of garlic supplementation on fasting blood sugar (FBS), hemoglobin A1c (HbA1c), and lipid profile in patients with T2DM.
Methods:
All articles published up to November 2024 were reviewed through the PubMed, SCOPUS, and Web of Science databases to gather all randomized clinical trials (RCTs) on T2DM patients in which garlic was used as a treatment. A random-effects model was used to measure pooled effect sizes. Weighted mean differences (WMDs) and 95% confidence intervals (CIs) were used to report pooled effect sizes. Subgroup analysis was utilized to investigate heterogeneity.
Results:
Finally, 8 studies were included in this systematic review and meta-analysis. Our pooled meta-analysis showed a significant decrease in FBS after garlic therapy based on 10 effect sizes (WMD: −12.41; 95% CI: −15.13 to −9.69; I² = 99.2%) and in HbA1C based on 7 effect sizes (WMD: −0.5; 95% CI: −0.66 to −0.33; I² = 96.4%). Also, total cholesterol (TC) was significantly reduced (WMD: −8.26; 95% CI: −14.65 to −1.88; I² = 90.9%) based on 7 effect sizes, while changes in HDL-C, TG, and LDL-C were not significant overall. However, when garlic was combined with oral hypoglycemic agents, a significant reduction in LDL-C was observed (WMD: −8.64; 95% CI: −10.54 to −6.78; I² = 95.6%) compared to garlic alone. Moreover, longer duration of garlic supplementation significantly improved all lipid profiles in patients with T2DM. Significant improvements in HDL-C, LDL-C, and TC were also noted in older patients after garlic therapy.
Conclusions:
The findings of this systematic review and meta-analysis support the potential effect of garlic therapy for the management of T2DM. However, due to the low quality of the studies included in this review, further high-quality RCTs should be conducted based on our findings.
PROSPERO registration number:
CRD42024628780.
Introduction
Type 2 diabetes mellitus (T2DM) is one of the most significant public health concerns worldwide. 1 T2DM is caused by impaired insulin secretion and beta-cell dysfunction. 2 So far, more than 530 million people worldwide have been diagnosed with diabetes (3). There are affordable therapy options for the management of T2DM, including lifestyle modifications, healthy eating patterns, and physical activity. 3 Also, sugar-lowering medicines, including thiazolidinediones, biguanides, and sulfonylureas, can be effective in the management of blood sugar levels in diabetic patients. 4 These methods have been used for T2DM, although some adverse effects have been observed in a few patients after using these medications. 5 Most antidiabetic medicines prescribed to these patients have various side effects. 6 Therefore, traditional treatments attract more attention than any available modern medicine (8).
Many ancient herbal therapies, such as ginger, turmeric, flaxseed, cinnamon, and fenugreek, have long been used to treat patients with metabolic disorders.7 -12 Anciently, garlic (genus Allium) was used as a spice, additive, and medicinal plant in many foods around the world. 13 Many studies have demonstrated the tremendous medical advantages of garlic in both humans and animals.14,15 In addition, garlic, as one of the dietary ingredients, has beneficial effects on diabetic complications.16,17 These beneficial effects of garlic are likely due to the presence of sulfur compounds.18,19
According to one study, blood glucose was significantly lower in the group of raw garlic-treated diabetic rabbits than in the control group. 20 Furthermore, a study found that the administration of garlic extract led to a decrease in serum glucose levels in diabetic rats. 21 Also, some human studies reported that taking garlic supplements did not decrease blood sugar levels in patients with T2DM. 22
Although some reports support the beneficial effects of garlic in diabetic patients, a recent study showed that garlic pills, as a safe medicine, could reduce fasting blood sugar (FBS) in women with prediabetes between 24 and 28 weeks of gestation. 23 Also, some studies have suggested that garlic has a lipid-lowering effect in diabetic patients.22,24
S-allyl cysteine sulfoxide, a compound found in garlic, has demonstrated the ability to stimulate insulin secretion in diabetic rats. 25 Furthermore, garlic contributes to reducing the risk of atherosclerosis by lowering blood pressure, cholesterol levels, and potentially managing diabetes mellitus. It also prevents the formation of blood clots.26,27 In addition, garlic may support the reduction of cholesterol and blood glucose, aiding in the management of hyperlipidemia and diabetes.28,29
Furthermore, it is important to consider that the simultaneous use of antidiabetic medications and garlic may have different effects on T2DM compared to their separate use. Current study aimed to answer whether consuming garlic alone has a different effect compared to taking it simultaneously with antidiabetic medicines. A few studies have investigated the simultaneous use of antidiabetic drugs and garlic in patients with T2DM. 21 A previous study indicated that garlic alone or in combination with sulfonylurea derivatives has a similar effect on FBS in patients with T2DM. 30 However, another study showed that metformin combined with garlic has a stronger therapeutic effect than metformin alone. 31
As mentioned above, many studies have reported that garlic is used to improve metabolic parameters in people with type 2 diabetes. However, results from randomized clinical trials (RCTs) on garlic’s effects on glycemic markers have been inconsistent. To the best of our knowledge, no systematic review has currently evaluated the therapeutic impact of garlic supplements with or without antidiabetic medications on the metabolic profile of patients with T2DM. Therefore, we conducted a meta-analysis of RCTs to assess the efficacy of garlic in managing type 2 diabetes.
Methods
Search Strategy
Current systematic review and meta-analysis was conducted on RCTs following the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The protocol of our study was registered in PROSPERO (No. CRD42024628780). This study aims to evaluate the effects of garlic on hemoglobin A1c (HbA1c), FBS, total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C).
The search strategy is provided in Supplemental File 1. We did not apply any language restrictions in this study, and to avoid missing relevant studies, we also reviewed the references cited in previous systematic reviews.
Inclusion Criteria
Table 1 shows the PICOS (Population, Intervention, Comparison, Outcome, and Study Design) criteria. We included studies involving patients with T2DM who were able to consume garlic and complete the trials.
The Inclusion Criteria of PICOS.

Exclusion Criteria
Studies that met any of the following criteria were excluded from our study: those conducted on animals, children, or cells; studies involving lactating or pregnant women; dissertations and conference abstracts; studies without a placebo group; and studies lacking sufficient information.
Data Extraction and Quality Assessment
The eligibility of the studies was assessed by 2 authors (AE, LS). The following information was extracted from each study: author’s name, year of publication, country, subjects and gender, age range, study design, daily garlic dosage, study duration, outcomes, method of outcome assessment, sample size, mean and SD of outcomes in the intervention and control groups, and any additional interventions.
Cochrane criteria were used to assess the methodological quality of the studies. Two independent authors (AE and MAI) evaluated the risk of bias based on random sequence generation, blinding of personnel and participants, allocation concealment, blinding of outcome assessors, selective outcome reporting, completeness of outcome data, and other potential biases. For each study, the risk of bias was classified as low, high, or unclear. 32
Data Synthesis and Statistical Analysis
To determine between-study heterogeneity, Cochran’s Q test and I-square statistics were used (I² > 50% indicating significant heterogeneity). Pooled effect sizes were reported as weighted mean differences (WMD) with 95% confidence intervals (CI) using random-effects analysis. Fixed-effect analysis was applied for all subgroup analyses. Statistical analysis was performed using STATA version 11.0. Sensitivity analyses were per-formed for all outcomes. Sensitivity analyses were performed using a leave-one-out method. In this approach, each study was sequentially removed from the meta-analysis to assess its individual influence on the overall effect size and the stability of the pooled results. Only Begg and Mazumdar’s test was performed to assess publication bias due to having fewer than 10 studies. 33
Characteristics of the Included Studies
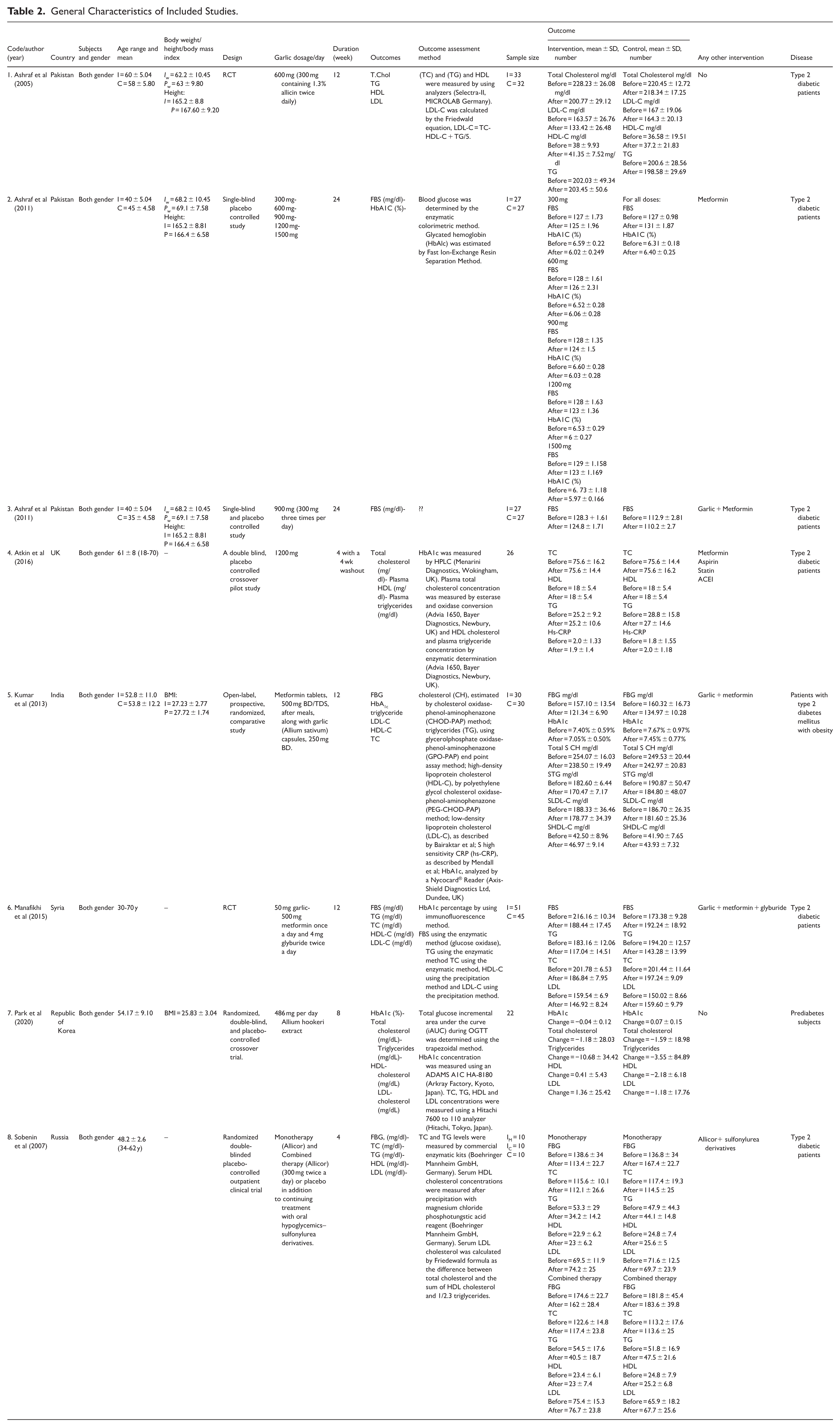
By searching the database, 3318 articles were retrieved. After screening titles and abstracts, 715 duplicates were removed, leaving 2603 articles. Based on the inclusion and exclusion criteria, we included 8 studies with 13 effect sizes in this systematic review and meta-analysis (Figure 1). Included studies were published between 2005 and 2020. In total, 607 participants of both genders were divided into 307 in the intervention group and 300 in the placebo group. The average age of the patients ranged from 18 to 75 years. Garlic was administered daily in dosages ranging from 50 to 1500 mg in the included studies. The duration of the intervention varied between 4 and 24 weeks (Table 2).
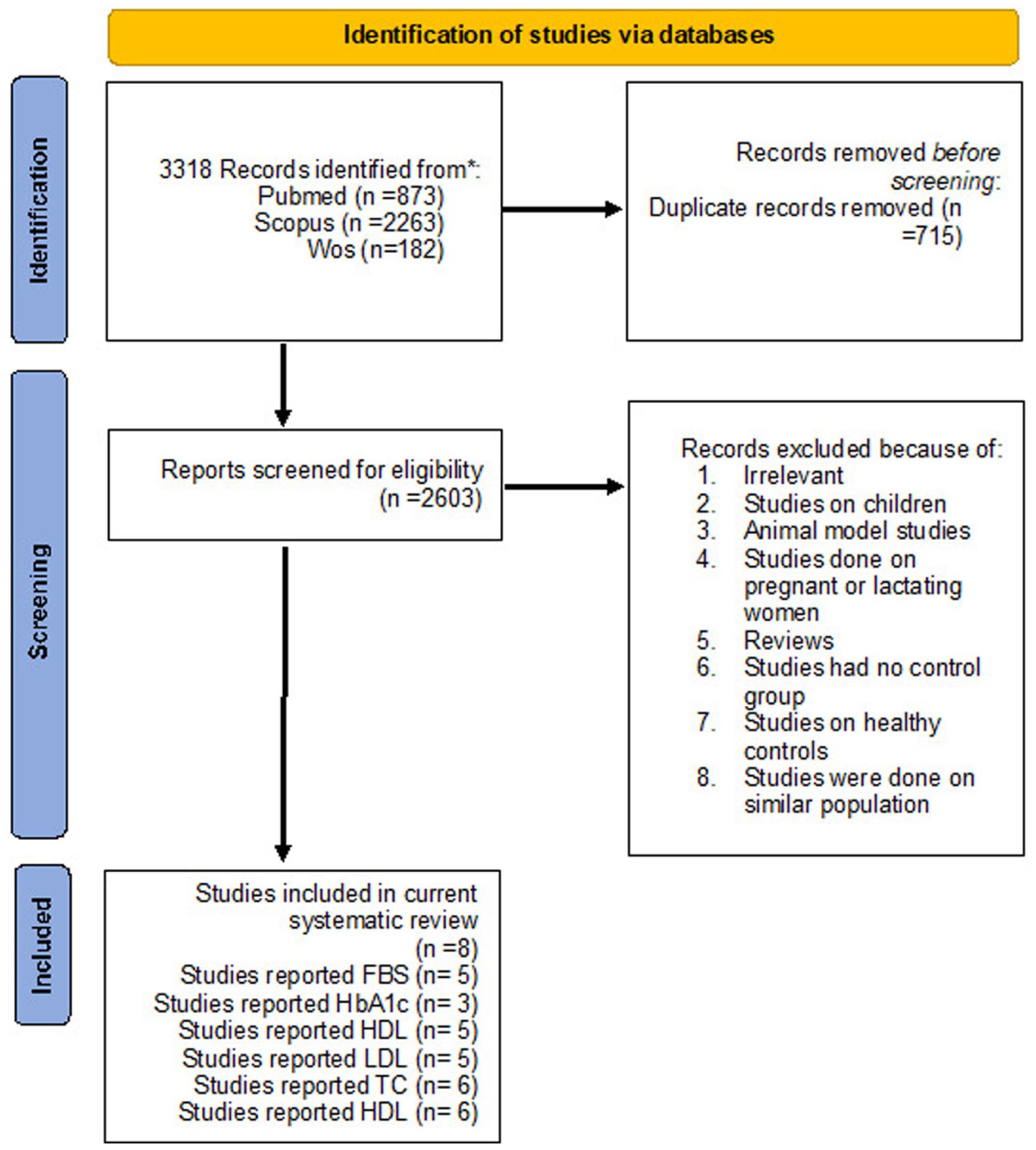
Literature search and review flowchart.
General Characteristics of Included Studies.
Risk of Assessment
Evaluation of the study quality using the predetermined tool revealed that one of the studies included in our meta-analysis was of high quality, while the remaining studies exhibited low methodological quality. Most studies demonstrated inadequate or poorly reported randomization processes. Few explicitly described the method of sequence generation, and in many cases, allocation concealment was either unclear or absent. Such deficiencies increase the risk of selection bias. Blinding was insufficiently applied across the majority of studies. Many failed to blind participants, personnel, and outcome assessors, which raises concerns. Selective outcome reporting and incomplete data presentation were common issues. Several studies did not report all outcomes or omitted negative results, limiting transparency. Additional information regarding the quality assessment of the included studies can be found in Table 3.
Assessment of Risk of Bias in the Included Studies Using Cochrane Criteria.

Effects of Garlic Supplementation on FBS and HbA1C
Our combined meta-analysis revealed that administering garlic at doses ranging from 50 to 1500 mg per day, over a period of 4 to 24 weeks, significantly reduced FBS levels in adult patients with diabetes compared to the control group (P < .05). This conclusion is based on data from 5 studies, including a total of 10 effect sizes (WMD: −12.41; 95% CI: [−15.13, −9.69], I² = 99.2%; Figure 2).
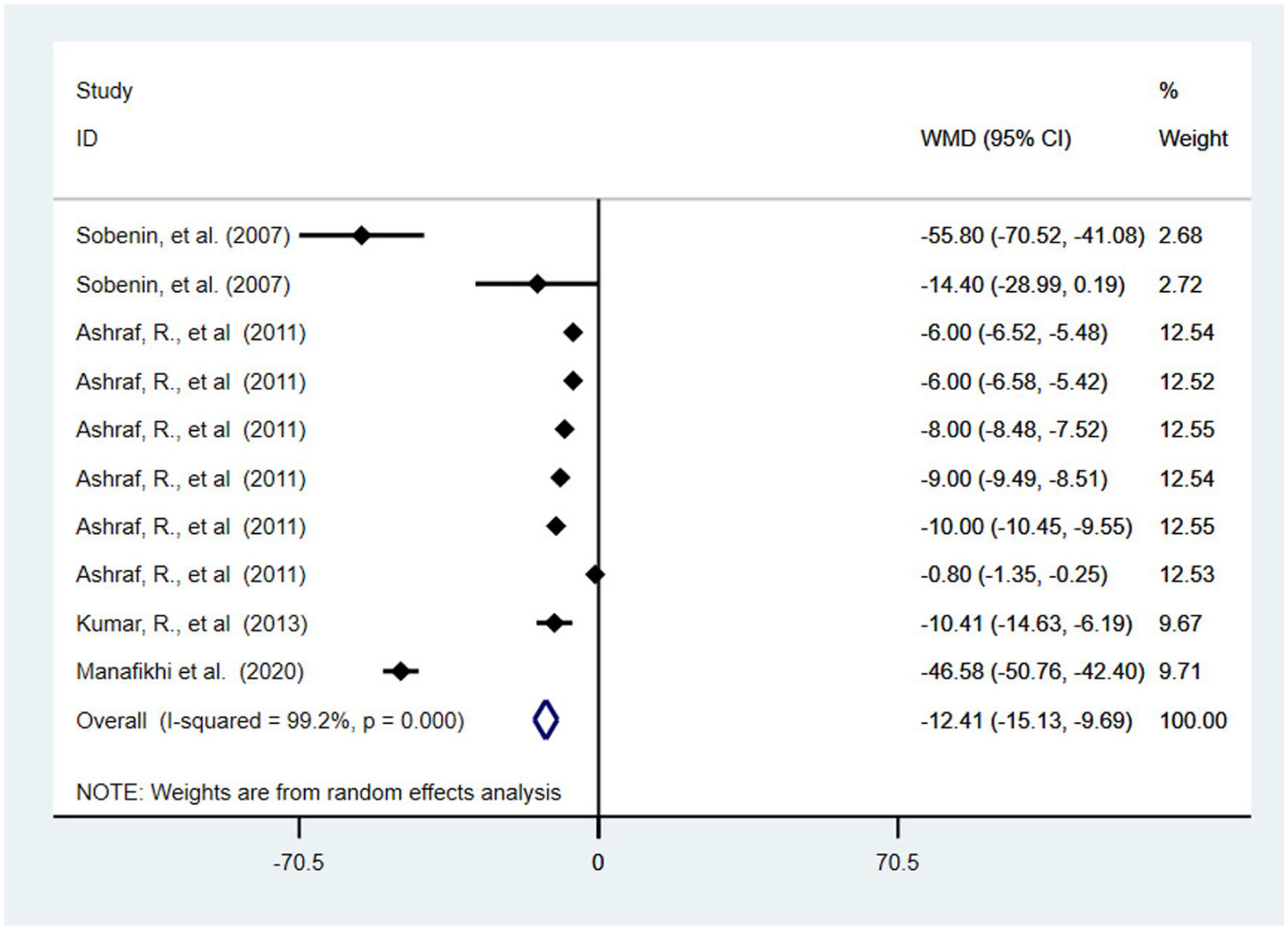
Forest plot for the effect of garlic therapy on FBS in T2DM patients; expressed as the mean differences between the intervention and the control. The area of each square is proportional to the inverse of the variance of the WMD. Horizontal lines represent 95% CIs. Diamonds represent pooled estimates from random-effects analysis.
The reduction in HbA1c (WMD: −0.5; 95% CI [−0.66, −0.33], I² = 96.4%) was also significant, based on 7 effect sizes from 3 studies (Figure 3). Due to substantial heterogeneity between studies, we conducted subgroup analyses based on factors such as participants’ age (<50 years and ⩾50 years), presence or absence of concomitant glucose-lowering medications, garlic dosage (<600 and ⩾600 mg), study duration, and publication year (<2011 and ⩾2011). Significant changes were observed in all FBS and HbA1c measurements; however, no differences were found in the subgroup analysis results for FBS and HbA1c (Table 4). Sensitivity analysis for FBS and HbA1C confirmed the stability of these results. Although, Egger’s test indicated the presence of publication bias for FBS and HbA1c (P ˂ .05).

Forest plot for the effect of garlic therapy on HbA1C in T2DM patients; expressed as the mean differences between the intervention and the control. The area of each square is proportional to the inverse of the variance of the WMD. Horizontal lines represent 95% CIs. Diamonds represent pooled estimates from random-effects analysis.
Subgroup Analyses for the Effects of Garlic Supplementation on FBS, HbA1C, and Lipid Profile in Patients with T2DM.

Effects of Garlic Supplementation on Lipid Profile
The reduction in TC (WMD = −8.26; 95% CI = −14.65 to −1.88; I² = 90.9%) was statistically significant based on 6 studies including 7 effect sizes (Figure 4). Changes in other lipid profiles, including HDL-C (WMD −0.74; 95% CI –0.15 to 1.63; I² = 42.2%), TG (WMD −6.21; 95% CI −14.7 to 2.29; I² = 92.0%), and LDL-C (WMD −8.86; 95% CI −18.61 to 0.88; I² = 93.3%), were not statistically significant (Figures 5-7). However, the subgroup analysis indicated that when garlic was used alongside oral hypoglycemic medications, a significant reduction in LDL-C [WMD −8.64; 95% CI (−10.54, −6.78), I² = 95.6%] was seen compared to using garlic alone.

Forest plot for the effect of garlic therapy on TC in T2DM patients; expressed as the mean differences between the intervention and the control. The area of each square is proportional to the inverse of the variance of the WMD. Horizontal lines represent 95% CIs. Diamonds represent pooled estimates from random-effects analysis.

Forest plot for the effect of garlic therapy on HDL-C in T2DM patients; expressed as the mean differences between the intervention and the control. The area of each square is proportional to the inverse of the variance of the WMD. Horizontal lines represent 95% CIs. Diamonds represent pooled estimates from fixed-effects analysis.
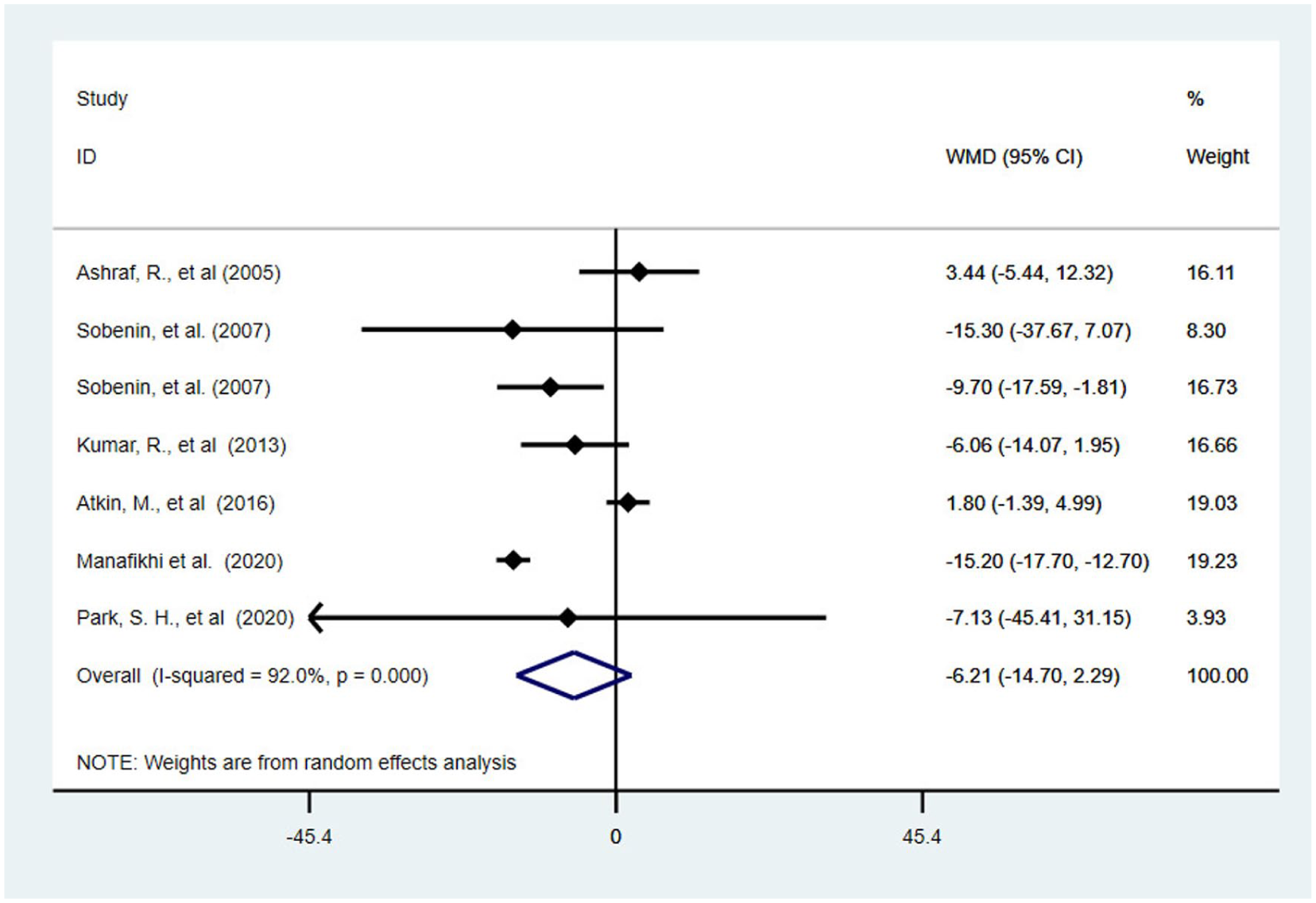
Forest plot for the effect of garlic therapy on TG in T2DM patients; expressed as the mean differences between the intervention and the control. The area of each square is proportional to the inverse of the variance of the WMD. Horizontal lines represent 95% CIs. Diamonds represent pooled estimates from random-effects analysis.

Forest plot for the effect of garlic therapy on LDL-C in T2DM patients; expressed as the mean differences between the intervention and the control. The area of each square is proportional to the inverse of the variance of the WMD. Horizontal lines represent 95% CIs. Diamonds represent pooled estimates from random-effects analysis.
According to the subgroup analysis, improvements in all lipid profiles were significantly greater with longer durations of garlic supplementation (more than 12 weeks). Additionally, HDL-C, LDL-C, and TC levels showed significant improvements in older patients (over 50 years). In contrast, a significant improvement in TG was observed only in younger diabetic patients (under 50 years) and not in older ones. Furthermore, significant improvements in HDL-C and TG levels were seen with doses below 600 mg per day (Table 4).
A sensitivity analysis was conducted to assess the robustness of the findings regarding the lipid profile. Notably, removing the studies by Ashraf et al (2005), Kumar et al (2013), and Manafikhi et al (2015) notably impacted the overall effect of garlic supplementation on total cholesterol (TC), changing the effect to a non-significant level. Removing the studies by Park et al (2020) and Sobnin et al (2007) significantly altered the overall effect of garlic supplementation on LDL making the effect statistically significant. Also, results of the sensitivity analysis showed that removing the Atkin et al (2016) study significantly affects the results for HDL and TG levels. Publication bias was assessed using Begg’s test, which showed no significant evidence of publication bias for any of the lipid profile (P ˃ .05).
Discussion
This study aimed to investigate the effects of garlic supplementation on lipid profiles, FBS, and HbA1c in patients with T2DM. Additionally, the current systematic review and meta-analysis examined the impact of garlic supplementation alongside antidiabetic medications compared to garlic supplementation without these modern drugs.
Our meta-analysis revealed a significant decrease in FBS and HbA1c levels in patients with T2DM following garlic supplementation. The observed reduction in HbA1c of 0.5% is not only statistically significant but also clinically meaningful. In patients with T2DM, reductions ⩾0.5% are associated with measurable improvements in long-term glycemic control and decreased risk of microvascular complications, indicating that the magnitude of effect observed in our analysis is relevant in clinical practice.34,35 A study conducted in 2013 reported that garlic at a dose of 250 mg twice daily, combined with metformin tablets, significantly reduced FBS levels in patients with diabetes. However, the change in HbA1c levels was not statistically significant. 31 In line with the current study, a meta-analysis by Wang et al found that garlic supplementation significantly reduced both FBS and HbA1c levels compared to placebo in patients with T2DM. 36 The results of the present meta-analysis are consistent with previous studies by Ashraf et al and Khan et al , which showed that garlic supplementation significantly reduced FBS and HbA1c over 24 weeks compared to the control group.37,38 Although Manafikhi et al reported a decrease in FBS levels over 12 weeks with garlic supplementation in patients with T2DM treated with metformin and glyburide, it did not show significant changes in HbA1c levels. 39 This partially contrasts with our findings, as we observed significant reductions in both FBS and HbA1c. These differences could be attributed to the shorter intervention durations in their studies compared to the longer durations in the studies included in our analysis. Additionally, Manafikhi et al used low-dose garlic capsules (25 mg twice daily), whereas the studies in our analysis often employed higher doses or different forms of garlic, such as raw garlic or more potent supplements, which may enhance therapeutic effects. Furthermore, a previous systematic review and meta-analysis by Emami et al concluded that garlic consumption did not significantly reduce HbA1c levels, likely because many of the included studies had short durations, typically less than 8 weeks. 40 Since HbA1c reflects the average blood glucose over approximately 8 to 12 weeks, 41 studies with shorter durations likely could not capture meaningful changes in this marker. Additionally, variations in participant characteristics may have influenced the outcomes, which contrasts with our findings.
In addition, our study indicated a significant change in TC after garlic therapy in patients with T2DM, but not in TG, LDL-C, or HDL-C levels. Despite not reaching statistical significance, the observed reductions in TG (–6 mg/dl) and LDL-C (–9 mg/dl) may still carry clinical relevance. Even modest improvements in these lipid parameters have been associated with incremental reductions in long-term cardiovascular risk, particularly in patients with T2DM who are already at elevated baseline risk. Therefore, although the confidence intervals include the null, the direction and magnitude of change suggest a potentially beneficial clinical effect that warrants confirmation in larger, high-quality trials.42,43 Also, subgroup analysis showed that garlic alongside oral hypoglycemic medications could significantly improve TG levels compared to garlic alone. This highlights the value of garlic as an adjunctive treatment that complements modern therapies to improve cardiovascular health in patients with T2DM. In line with our study, a previous study reported a significant decrease in TC levels in T2DM patients following garlic therapy (23). Another systematic review and meta-analysis conducted by Shabani et al reported that garlic significantly reduced lipid parameters, including TC, TG, LDL-C, and HDL-C. 29 While this partially aligns with our findings, it differs in showing significant changes in TG, LDL-C, and HDL-C levels. A possible reason for this discrepancy is the difference in garlic dosage used in their study. Their meta-analysis included variable dosing regimens (500-20 000 mg/day), which were higher than the garlic dosage used in the present study. Another systematic review indicated reductions in TC, LDL, and TG, along with an increase in HDL, following garlic supplementation. 44 It was partially consistent with our study in the reduction of TC, but our study did not show significant changes in LDL-C, TG, or HDL-C levels. Possibly, shorter intervention durations contributed to this discrepancy. Another study conducted by Chattwal et al demonstrated that garlic, particularly when combined with metformin, significantly reduced TC, TG, and LDL-C, and increased HDL-C. While our study supports a reduction in TC, it contrasts with their findings for TG, LDL-C, and HDL-C, which remained insignificant in our study (30). Variations in garlic dosage, form, and supplementation duration may explain the differences in outcomes compared to our study.
A systematic review and meta-analysis conducted by Zhao et al found that garlic significantly reduced total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C), and increased high-density lipoprotein cholesterol (HDL-C), but did not significantly affect triglyceride (TG) levels. This partially aligns with our findings, as we also observed a significant reduction in TC but did not find significant changes in TG, LDL-C, or HDL-C. 45 Possible reasons for the differences with the current results may be due to longer supplementation periods and higher doses of garlic used in their study. Additionally, their study included various populations such as patients with hyperlipidemia, hemodialysis, T2DM, myocardial infarction, coronary artery disease, non-alcoholic fatty liver disease, obesity, hypertension, polycystic ovary syndrome, and healthy adults, whereas we included only patients with T2DM.
The exact mechanisms by which garlic supplementation influences blood glucose and lipid profiles are not fully understood; however, some hypotheses have been proposed. The hypoglycemic effect of garlic oil is mainly attributed to diallyl trisulfide, a key constituent of garlic. Additionally, Scanga discovered that alliin acts as a substrate for the L-Type Amino Acid Transporter 1 (LAT1), a cellular membrane transporter that interacts with alliin and plays a significant role in human metabolism, diabetes, and cancer. 46 Alliin also influenced the composition of intestinal microbes, generally decreasing Lachnospiraceae and increasing Ruminococcaceae in mice with diet-induced obesity. Therefore, Liu et al inferred that garlic plays a nutritional or therapeutic role in diabetes prevention. 47 In another study, Parham et al described a herbal medicine containing garlic that has the potential to enhance insulin secretion, improve insulin sensitivity, and reduce insulin resistance.48,49
One of the primary functions of garlic-derived products is cardiovascular protection, as evidenced by their various beneficial effects. Numerous studies have highlighted the essential role of organosulfur compounds (OSCs) in garlic in reducing the risk of cardiovascular diseases (CVDs). OSCs exhibit significant pharmacological activities, including antihyperlipidemic, antiatherosclerotic, antihypertensive, antiplatelet aggregation, and antithrombotic effects, which can effectively contribute to the prevention of CVDs. 50 Research suggests that molecular docking studies have revealed the potential of organosulfur compounds found in garlic, including Alliin, Allicin, Eajoene, and Z-ajoene, as inhibitors of FAS (fatty acid synthase). 51 FAS, a protein primarily associated with lipid synthesis for energy storage in the liver, has recently been identified as playing a role in signaling processes, including the activation of Peroxisome Proliferator-Activated Receptor (PPARα). 52 The activation of PPARα triggers an adaptive response, facilitating the transcription of genes responsible for fatty acid uptake and catabolism. Therefore, garlic consumption may be beneficial for the treatment of hyperlipidemia. 50
The combination of alliin with standard antidiabetic drugs such as glibenclamide and insulin demonstrates moderate efficacy in managing hyperglycemia. 53 Black solo garlic extract significantly reduces pro-inflammatory cytokines (Interleukin 1 beta, Interleukin 6, Tumor Necrosis Factor Alpha) while increasing Interferon gamma levels in streptozotocin-induced diabetic rats, outperforming glibenclamide. 46 Allium species contribute to diabetes treatment by upregulating caspase-3 and caspase-9 gene expression. 54 Alliin also modulates gut microbiota, decreasing Lachnospiraceae and increasing Ruminococcaceae, which supports its therapeutic role in diabetes prevention. 55 Allicin acts as a transient receptor potential ankyrin 1 agonist, and when combined with a high-fat diet, it helps prevent Glucagon-like peptide-1dysregulation and maintains glucose homeostasis. 56 The hypoglycemic effects of garlic are attributed to sulfur-containing compounds such as allylpropyl disulfide and diallyl disulfide, which influence purine metabolism.57 -59 Additionally, treatment with garlic oil and diallyl trisulfide enhances glucose-to-glycogen conversion.57,60 The blood glucose-regulating effects of garlic are also linked to its sulfur compounds and flavonoids. 61 Furthermore, garlic may prevent the rise of corticosterone and adrenal hypertrophy, thereby mitigating hyperglycemia in diabetic models. 62
This systematic review and meta-analysis is among the first studies to investigate the effects of garlic in conjunction with blood glucose-lowering medications in patients with diabetes, evaluating the synergistic impact of garlic supplementation alongside conventional antidiabetic drugs, and providing novel insights into holistic diabetes management. Furthermore, according to the results of subgroup analysis, this study may offer improved recommendations for the clinical management of T2DM.
There are several limitations to the current systematic review and meta-analysis that must be considered when interpreting the final results. First, the inclusion of only 8 studies may introduce a degree of selection bias, which may limit the generalizability of our findings across different populations and clinical settings. Garlic dosage varied widely among the included trials, ranging from low to high amounts, which could influence bioavailability and physiological responses and consequently contribute to inconsistent outcomes. Intervention duration also differed substantially; shorter trials may not fully capture the long-term metabolic effects of garlic supplementation, whereas longer studies may demonstrate more pronounced benefits but are more susceptible to adherence issues.
Furthermore, participant characteristics such as age, baseline metabolic status, comorbidities, lifestyle behaviors, and genetic factors play an important role in shaping individual metabolic responses and may partly explain differences in reported effects. Different forms of garlic supplementation, each with distinct bioavailability profiles, were also used across studies, potentially affecting the final outcomes. In addition, most included studies had relatively low methodological quality, increasing the risk of bias. Some trials lacked detailed information regarding participants’ dietary intake, which could significantly influence glycemic and lipid outcomes in patients with T2DM. These variations collectively underscore the need for more standardized protocols in future trials.
Beyond these limitations, the substantial heterogeneity observed in our meta-analysis further highlights the methodological inconsistency across studies. One important source of variability was the difference in study designs and blinding procedures, as trials ranged from randomized single-blind to randomized double-blind designs. Inadequate blinding and insufficient randomization may influence outcome assessment, thereby affecting effect size estimates. Additionally, variations in concomitant medications, including the use of metformin, sulfonylureas, or statins alongside garlic, complicate the interpretation of garlic’s independent effects and may contribute to heterogeneity. Differences in population characteristics and wide variability in intervention duration from 4 to 24 weeks, also play a role. Together, these methodological and clinical differences explain much of the observed heterogeneity. Although subgroup analyses were conducted to address some sources of variability, residual heterogeneity remained. Future research would benefit from more rigorous trial designs, standardized garlic formulations and dosing regimens, and consistent outcome reporting to reduce heterogeneity and strengthen pooled estimates.
In conclusion, our findings suggest that garlic supplementation has beneficial effects on FBS, HbA1c, and TC in patients with T2DM. Also, when garlic is used alongside oral antidiabetic agents, it can reduce LDL-C in patients with T2DM compared to using garlic alone. However, further randomized controlled trials with larger sample sizes are needed to confirm the results of the current systematic review and meta-analysis.
Supplemental Material
sj-docx-1-nmi-10.1177_11786388251413660 – Supplemental material for The Therapeutic Effect of Garlic Supplements on the Metabolic Profile of Patients With Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Clinical Trials
Supplemental material, sj-docx-1-nmi-10.1177_11786388251413660 for The Therapeutic Effect of Garlic Supplements on the Metabolic Profile of Patients With Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Clinical Trials by Anahita Ebrahimzadeh, Mohammad Safargar, Milad Rajabzadeh-Dehkordi, Faezeh Nematolahi, Mahsa Samadani, Laya Saeid, Abbas Mohtashamian, Mohammad Ali Izadi, Armin Ebrahimzadeh and Ali Reza Safarpour in Nutrition and Metabolic Insights
Footnotes
Author Contributions
Armin Ebrahimzadeh, Ali Reza Safarpour and Anahita Ebrahimzadeh conceived and designed the study. Anahita Ebrahimzadeh, Mohammad Safargar, Milad Rajabzadeh-Dehkordi, Faezeh Nematolahi, Mahsa Samadani, Laya Saeid, Abbas Mohtashamian, Mohammad Ali Izadi and Armin Ebrahimzadeh performed the data collection. Armin Ebrahimzadeh and Anahita Ebrahimzadeh conducted the data analysis and interpretation of data. Armin Ebrahimzadeh, Mohammad Safargar and Mahsa Samadani drafted manuscript. Armin Ebrahimzadeh, Ali Reza Safarpour and Anahita Ebrahimzadeh conducted a review of the manuscript and finalized the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is provided within the manuscript.
Registration and Protocol
The protocol of our study was registered in PROSPERO (No. CRD42024628780).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.