
Abstract
Background:
A poor dietary intake of key macronutrients and micronutrients adversely affects pregnancy outcomes and neonatal health. The occurrence of dietary inadequacy during pregnancy is higher compared to any other stage of the life cycle. Therefore, this study aimed to assess dietary practice and associated factors among pregnant women.
Methods:
A facility-based cross-sectional study design was conducted among 378 pregnant women from March to May 2021 at the public health institution of Mizan-Aman town, southwest Ethiopia. A systematic random sampling technique was used to reach the study participants. The short food-frequency questionnaires and nutrition-behaviors checklist measurement were used to assess the dietary practice. Nine questions were applied to assess the dietary attitudes of the respondents. After the summation of the score, the respondent was categorized as favorable attitude if their score was > the median and unfavorable attitude if their score was ⩽ to the median of the score. The data were entered into Epi Data 3.1 and exported to Statistical Package for Social Science (SPSS) version 21 software for analysis. Variables of P-value <.25 during bivariate logistic regression analysis were considered for multivariate analysis. Finally variables with an adjusted odds ratio of P-value <.05 along with a 95% Confidence interval (CI) were declared statistically significant.
Results:
The overall magnitude of good dietary practice among pregnant women was 25.1% (95% CI: 20.9, 29.71%). In multivariate logistic regression analysis, the variables having television/radio (AOR = 4.2, 95% CI: 1.8, 10.2), household food security (AOR = 3.1, 95% CI: 1.0, 9.9), good dietary knowledge(AOR = 4.1, 95% CI: 1.98, 8.6), favorable dietary attitude (AOR = 4.34, 95% CI: 1.2, 8.7), monthly income of 1000 to 2000 Ethiopian birr (AOR = 3.7, 95% CI: 1.3,11.2) and >2000 Ethiopian birr (AOR = 7.0;95% CI: 3.3,15.4) were significantly associated with good dietary practice.
Conclusion:
The dietary practice among pregnant women was very low. The factors like having television/radio, good dietary knowledge, household food security, favorable dietary attitude, and monthly income of 1000 to 200 and greater than 2000 Ethiopian birr were significantly associated with the good dietary practice of pregnant women.
Introduction
Maternal nutrient deficiency remains a significant public health problem in middle and low-income countries, with adverse maternal and child health outcomes due to the women living in resource-limited countries consume a monotonous diet.1-3 The recommended intake for most nutrients increased during pregnancy, 4 but the majority of pregnant women have inadequate nutrient intake when compared to the recommended standards by the world health organization (WHO).5,6 Physiological change during pregnancy such as formation and synthesis of new tissue, growth of maternal tissue, and the developing fetus increase energy and nutrients requirements of pregnant women,4,7 and to meet this extra demand, pregnant women have to consume an adequate and balanced diet which can provide an adequate amount of macronutrients and micronutrients. 8 Proper consumption of essential macronutrients and micronutrients during pregnancy has a positive impact on pregnancy outcomes and health of mothers and their infants 9 and also the promotion of women health and prevention of health care from womb to throughout the life process critically determine women health status and the cycle of malnutrition. 1 However, the frequency of poor dietary practice due to a poor dietary pattern is higher during pregnancy compared to any other stage of the life cycle, 10 and this low dietary practice increase risk of intrauterine growth restriction, low birth weight, preterm birth, anemia, increased infection, congenital disability, pre-eclampsia, prenatal, and infant mortality and morbidity. 11
Globally, an increasing number of women experience micronutrient deficiencies; almost half all pregnant women in the world are thought to have anemia and 9.8 million pregnant women have night blindness, and an estimated 19.1 million pregnant women have low serum retinol concentration. 9 Around 20 million babies are born of low birth weight each year globally, 12 and maternal undernutrition contributes to 800 000 neonatal deaths annually through small for gestational age birth. 13 Globally, micronutrients deficiency such as iron, zinc, vitamin A and iodine affect more than 2 billion people, and iron deficiency alone cause for 447 000 million maternal death.2,14 In low-income and middle-income countries, multiple-micronutrient deficiencies often coexist and can be further exacerbated in pregnancy with potentially adverse maternal outcomes. 6 Moreover, during pregnancy, the most common diet feature was imbalanced macronutrients, inadequate micronutrient intakes, and predominantly plant-based. 6 The prevalence of micronutrient deficiency of iron, vitamin A, iodine, zinc, calcium, and foliate among pregnant women in Ethiopia, Kenya, Nigeria, and South Africa ranges 19% to 61%, 21% to 48%, 87%, 46% to 76%, and 3% to 12% respectively. 15 In Ethiopia, macronutrients and micronutrient deficiency are the most common public health problems of pregnant women. Around 13%, 50%, and 82% of women in Ethiopia had inadequate consumption of iron, Zink, and vitamin A, while in the south nation, nationality and peoples region (SNNPR), 32.6%, 75.1%, and 41.3% of women had inadequate intake of iron, Zink, and vitamin A respectively. 16
Generally, poor dietary practices and undernutrition of women arise from complex biological, physiological, psychological, economic, social, cultural beliefs, food taboo, and environmental factors.17-19 On the other hand, food insecurity, poverty, female illiteracy, communicable disease burden, heavy workload, inadequate access to health care, and poor sanitation and hygiene are the major factors influencing women’s nutrition in middle and low-income countries. 20 To improve maternal nutritional status during pregnancy, different organizations and scholars recommend the context-based nutritional intervention strategies that a pregnant woman should follow during every stage of her pregnancy live.2,8,14,21 Currently, the Ethiopian government developed a national nutrition program II (NNPII) 2016 22 intervention strategy focused on 100 critical days aimed to end undernutrition. However, the prevalence of good dietary practice of pregnant women in Ethiopia remains low, ranging from 19.9% to 40.1%.23,24 Besides, previous studies in Ethiopia mainly focus on pregnant women’s nutritional status, and there is no consistent evidence about pregnant women’s dietary practices in Ethiopia. 23 Moreover, no previous studies in the study area. For that reason, this study was aimed to identify the magnitude of dietary practice and associated factors among pregnant women attending antenatal care (ANC) at public health institutions in Mizan-Aman Town, southwest Ethiopia.
Methods
Study area
Mizan-Aman town is the capital of Bench- Sheko zone of SNNPR. The town is located 582 km far from the capital city of Addis Ababa. According to Zonal annual reports of 2020, the town has a total population of 62 689 (33 364 are men and 29 325 women). Maize and taro are the main staple foods, and while coffee and spices are the main cash crops in the area, the town has one teaching hospital and one public health center.
Study design and period
A facility-based cross-sectional study design was employed from March to May 2021.
Source population
All pregnant women attended ANC at public health institutions in Mizan-Aman town, southwest Ethiopia.
Sample size determination
The sample size was determined using a single population proportion formula, considering the following assumption: the prevalence of good dietary practice among pregnant women 33.9%, 25 5% marginal error, 95% Confidence Interval (CI), and none response rate of 10%. Based on this, the actual calculated sample size was:
Sampling technique
A systematic random sampling technique was used to select the study units using the client’s registration books for 3-months before the data collection period. Then every Kth person, as they registered, was included in the study until the desired sample size was attained.
Data collection procedures
The data were collected through the structured and semi-structured interviewer-administered questionnaire by Midwifery and Nursing health professionals. The data on socio-demographic and socio-economic, obstetric and pregnancy-related factors, household food security status, dietary knowledge, dietary attitude, and dietary practices of pregnant women were assessed. The tool used to assess dietary practices of pregnant women was adapted from FAO 25 and other different kinds of literature.10,23,26,27 Dietary practices of pregnant women were assessed using the retrospective dietary assessment methods of short-frequency questioners and nutrition-behaviors checklists measurements. 25 The score of dietary practices was obtained by summation of responses to each question. Each question was given 1 mark if the answer was correct, favorable, or healthy for dietary practices. Zero scores were given if the responses were wrong, unfavorable, or unhealthy for dietary practices.10,23,24,26 The study participants were classified as poor dietary practices if they correctly answered <75% of dietary practice questions and while good dietary practices if they correctly answered ⩾75%.27,28
The dietary knowledge was assessed using 10 open-ended questions adapted from the previous different kinds of literature.10,27,29,30,31 Nutrition knowledge questions aimed to assess pregnant women’s nutrition knowledge on the aspects of nutrition required during pregnancy. 29 Partially categorized questions were open-ended questions that require respondents to provide short answers in their own words, accompanied by a list of correct answers plus the options “Other” and “Do not know.” Predefined options make analysis easier by listing expected responses. After the surveyor has asked the question, he/she should write down the response provided and then categorize it according to the predefined response options. The pregnant women were considered to be knowledgeable if they correctly answered greater than or equal to 70% of the total knowledge assessing questions and not knowledgeable if respondents score <70% (out of 100%) on the knowledge questions.29,31
The attitude of pregnant women on their dietary practice during pregnancy was assessed by adapting the questioners from different literature and conceptualized it to local situations.31,32 Nine questions were applied in this study to assess maternal dietary attitudes that had 3 response options questions 1 positive; a middle option that captures the attitude that was uncertain and 1 negative. The pregnant women were given 1 mark if the answers were favorable for good dietary practices during pregnancy, and 0 scores were given if the responses were unfavorable for dietary practices.27,31 After the summation of the score, the respondent was categorized as favorable attitude if the respondent’s attitude score was > median and unfavorable attitude if the respondents ‘attitude score was ⩽ to the median of the score. 31
The household food insecurity level was measured with Household Food Insecurity Access Scale (HFIAS).33,34 The scale has been a valid tool in measuring household food insecurity among rural and urban areas of Ethiopia. 35 The tool consists of 9 questions representing a generally increasing severity of food insecurity (access). Based on the answer given to the 9 questions and frequency of occurrence over the past 30 days, participants are assigned a score that ranges from 0 to 27. A higher HFIAS score indicates more inadequate access to food and greater household food insecurity, while a score of 0 indicates secure access to food. 33
Data quality assurance
To ensure the quality of data, a pretest was done among 5% of the study sample. The final version of the questionnaire prepared in English was translated into the local language of the respondents and again translated back to English. Two days of training were given for collectors and supervisors on the instruments, data collection method, ethical issues, and the purpose of the study. Supervisors have checked the collected data for its completeness, accuracy, and consistency throughout the data collection period, and the principal investigator did the overall supervision. Data double entry was used to make comparisons of 2 data cells.
Data analysis methods
After all the data were checked for completeness and internal consistency, the data were coded and entered into Epi Data 3.1 computer software package and exported to Statistical package for social science (SPSS) version 21 software for further analysis. Bivariate logistic regression analyses were conducted to examine the association between dependent and independent variables. Variables with a P-value <.25 during bivariate logistic regression analysis were considered for multivariate logistic regression models to control all possible confounders and identify factors independently associated with the dietary practice of pregnant women. Crude Odd Ratio (COR) and Adjusted Odd Ratio (AOR) with 95% Confidence interval (CI) were calculated to measure the strength and direction of association between dependent and independent variables. Finally, the variable with (P-value <.05) in the multivariate logistic regression analysis were considered statistically significant. Multicollinearity between independent variables was checked Hosmer tested the model fitness—Lemeshow for the goodness of fit, and model fitted was considered at Hosmer-Lemeshow P-value >.05.
Results
A total of 374 pregnant women were participated in this study, making the response rate of 99%. The mean (±Standard deviation) age of the study participants was 26.4 (±4.9) years. Almost all, 364 (97.3%) participants were married and about 154 (41.2%), 277 (74.1%), and 192 (51.3%) of the study participants had no formal education, had family size <5, and their average monthly family income <1000, respectively (Table 1).
Socio-demographic and socio-economic characteristics of the study participants in Mizan-Aman town, southwest Ethiopia, 2021 (N = 374).
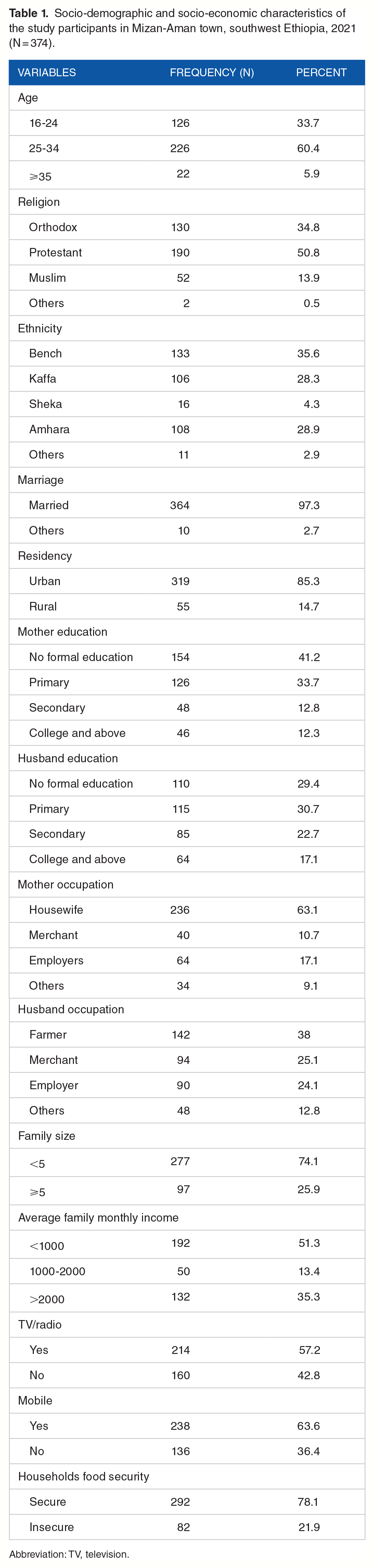
Abbreviation: TV, television.
Obstetric and pregnancy-related characteristics of the study participants
Out of the total study participants, 174 (46.5%) and 169 (45.25%) were in the third and second trimesters. Nearly half, 185 (49.5%) of study participants had <2 pregnancies, and about 264 (70.6%) had <2 number of live birth. Only 56 (15%) of study participants had ⩾4 ANC visits. The majority, 272 (72.7%) of study participants, had nutrition information (Table 2).
Obstetric and pregnancy-related characteristics of the study participants in Mizan-Aman town, southwest Ethiopia 2021 (N = 374).

Dietary knowledge of study participants
More than two-third, 258 (69%) of study participants had poor dietary knowledge, and 266 (71.1%) of the study participants did not know a balanced diet. Regarding knowledge about micronutrients source, about 218 (58.3%), 252 (67.5%), 174 (46.5%), and 254 (67.9%) of the study participants did not know vitamin A, calcium, iron, and iodine source of foods respectively.
The dietary attitude of study participants
The magnitude of favorable attitude for the dietary practice among participants was 172 (46.5%). Less than one-third, 104 (27.8%) of study participants had a good attitude toward eating more foods during pregnancy. Around 278 (73.8%) and 206 (55.1%) of study participants had a good attitude for the taste of meat and iron-rich foods and for preparing meals with iodized salt, respectively (Table 3).
Dietary attitude of the study participants in Mizan-Aman town, southwest Ethiopia, 2021 (N = 374).

The dietary practice of study participants
The mean (±SD) score of dietary practice among pregnant women was 9.15 (±2.9). Only a quarter, 94 (25.1%), of pregnant women have good dietary practice. Regarding specific practices, about half, 180 (48.1%) and 180 (48.1%) of study participants had additional meals and ⩾4 meals per day, respectively. About 124 (33.2%) of study participants skip their usual meals, and while 100 (26.7%) had the habit of craving foods, 51% were due to food odor reasons (Table 4).
Dietary practice of the study participants in Mizan-Aman town, southwest Ethiopia, 2021 (N = 374).

Factors associated with the dietary practice of pregnant women
In multivariate logistic regression analysis, the variables like having TV/radio, household food security, good dietary knowledge, favorable dietary attitude, and average monthly income of the family of 1000 to 2000 ETB and >2000 ETB showed significant association with the dietary practice of pregnant women (P < .05) (Table 5).
Factors associated with the dietary practice of the study participants in Mizan-Aman town, southwest Ethiopia, 2021 (N = 374).

Abbreviation: ETB, Ethiopians birr.
P value <.05. **P value <.001.
Discussion
Good dietary practice during pregnancy is one of the most determinant factors for the mothers and their long-term fetus health and nutritional status. Therefore, this study aimed to assess dietary practice and associated factors among pregnant women at public health institutions in Mizan-Aman town, southwest Ethiopia. According to this study found, only 25.1% of pregnant women had good dietary practice. It is in line with the study finding from Ambo district West Shoa zone, Oromia region, which revealed that around 26.9% of pregnant women had good dietary practice. 28 It is also slightly in line with the study finding from the Gedo zone, Guto Gida woreda and Misha woreda, which showed about 32.2%, 33.2%, and 29.5% of pregnant women have good dietary practice during pregnancy, respectively.29,32,36 However, this study finding is higher than the study finding from the West Gojjam Zone, Northwest Ethiopia, which showed only 19.9 % of pregnant women had good dietary practice. 24 This could be due to the study setting difference, where the study in the west Gojjam zone was conducted among rural residents while this study is conducted in urban settings that could have good nutrition information and counseling service.
On the contrary, this study finding was lower than studies finding from Addis Abeba city, Bahir Dar town, Mettu referral hospital, Horo Guduru Wolega zone, and Gondar town were found around 34.5%, 39.3%,78%, 74.6%, and 40.1% of pregnant women had good dietary practice respectively.10,23,31,37,38 This discrepancy might be due to socio-demographic and economic factors, seasonal variation of food production and consumption, measurement variation, and study setting difference. For example, most of the studies were used different types of measurement tools to assess dietary practice; this might be a reason for this finding variation.
According to this study, the study participants who owned television/radios were 4.2 times more likely to have good dietary practice than those who did not own television/radio in their house. The possible explanation for this could be that having TV/radio would help the participants disseminate the most important nutrition-related information about good dietary practice and its importance during pregnancy. This study finding is consistent with the study finding from Bahir Dar city, which showed pregnant women who owned Tv/radio were 3.17 times more likely to have good dietary practice than their counterparts. 10 Those who had good dietary knowledge were 4.12 times more likely to have good dietary practice than poor dietary knowledge. This is consistent with the study finding from Gondar town, Bahir Dar city, Gedo zone, and Misha woreda, revealing that the women who have good dietary knowledge were more likely to have good dietary practice during pregnancy.10,23,32,36 This means that as pregnant women dietary knowledge increased, the likelihood of good dietary practice of pregnant women could be increased. The participants who have a positive attitude for dietary practice during pregnancy were 4.53 times more likely to have good dietary practice than those who have a negative attitude. This study finding is similar to a study from Gedo zone, south Ethiopia which showed that the participants with a positive attitude had 1.9 times more likely to have good dietary practice than participants with a negative attitude. 32 It is also consistent with a study from the west Gojjam zone, which showed that participants with favorable attitudes were 1.69 times more likely to have good dietary practice than unfavorable attitudes. 24 This might be because women who have a positive attitude toward maternal nutrition are more likely to have the intention to follow specific dietary counseling during pregnancy.
The study participants of household food security were 3.2 times more likely to have good dietary practices than household food insecure. It is consistent with the study finding from the West Gojjam zone being food secure were 2.3 times more likely to have good dietary practice 24 and from Mettu Karl referral hospital being food insecure were 3.66 times more likely to have poor dietary practice than being secure food mothers. 37 The study participants with an average monthly income of 1000 to 2000 ETB and >2000 ETB were 3.7 and 7 times more likely to have good dietary practice than those who get <1000 ETB per month. This study finding is consistent with the study finding from Bahir Dar city, Gondar town, Ambo district, and Gedo zone.10,23,28,32 The explanation for this might be, the high earned women could easily afford and consume different food items. Moreover, most of the family from low-income countries spends most of their income for food expenditure.
Limitation of the study
One of the main limitations of this study was the lack of a standardized measurement tool at the national level in Ethiopia.
Conclusion
Generally, dietary practice during pregnancy was very low compared with others study findings. The factors like having television/radio, good dietary knowledge, household food security, favorable dietary attitude, and monthly income of 1000 to 200 and greater than 2000 Ethiopian birr were significantly associated with the good dietary practice of pregnant women.
Therefore, health professionals and any concerning body should work more on improving dietary practice among pregnant women.
Footnotes
Acknowledgements
First of all, we would like to thank Mizan-Tepi University for funding this study. Secondly, we would like to thank Mizan-Aman town health office management for their cooperation in giving valuable information. Finally, we would like to thanks our data collectors and supervisors for their unlimited efforts during data collection
Author Contributions
AGT wrote the proposal, participated in data collection, conception, study design, execution, acquisition of data, analysis, and interpretation, and was a major contributor in preparing the manuscript. AMK approved the proposal with some revisions, participated in data analysis, revised subsequent paper drafts, and commented on the final paper and manuscript. AGE participated in the data analysis, revised subsequent paper drafts, and commented on the final manuscript. All authors were read and approved the final manuscript.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Mizan Tepi University provided financial support for this research.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
First, ethical clearance was obtained from Mizan-Tepi University research and community support offices. Before this study, a formal letter was submitted to the administrator of the Mizan-Aman town health offices and the selected health facilities. The study objective, benefit, confidentiality, and risks were explained to the participants before data collection was done, and written informed consent was obtained from all respondents. The study participants have assured of their confidentiality, and the information they give us will not be used for any purpose other than the study.