
Abstract
Background:
Antenatal care is directed toward ensuring healthy pregnancy outcomes. Quality antenatal care increases the likelihood of receiving an effective intervention to maintain maternal, fetal, and neonatal well-being, while poor quality is linked to poor pregnancy outcomes. However, owing to the complex nature of quality, researchers have followed several approaches to systematically measure it. The evidence from these variable approaches appears inconsistence and poses challenges to programmers and policymakers. Hence, it is imperative to obtain a pooled estimate of the quality of antenatal care. Therefore, considering the scarcity of evidence on the quality of antenatal care, this study aimed to review, synthesize, and bring pooled estimates of accessible evidence.
Objective:
This study aimed to estimate the pooled magnitude and predictors of quality of antenatal care services and compare regional disparity.
Method:
We conducted a comprehensive systematic three-step approach search of published and unpublished sources from 2002 to 2022. The methodological quality of eligible studies was checked using Joanna Briggs Institute critical appraisal tool for cross-sectional studies. Meta-analysis was carried out using STATA version 16. Statistical heterogeneity was assessed using Cochran’s Q test. In the presence of moderate heterogeneity (I2 more than 50%), sensitivity and subgroup analyses were conducted and presented in a forest plot. Effect size was reported using standardized mean difference and its 95% confidence interval. Funnel plots and Egger’s regression test were used to measure publication bias at the 5% significance level. A trim-and-fill analysis was conducted to adjust for publication bias. Pooled estimates were computed using random-effects models and weighted using the inverse variance method in the presence of high heterogeneity among studies. A 95% CI and 5% significance level were considered to declare significance variables.
Results:
The global pooled poor-quality antenatal care was 64.28% (95% CI: 59.58%−68.98%) (I2 = 99.97%, p = 0.001). The identified pooled predictors of good-quality antenatal care service were: number of antenatal care visits (fourth and above antenatal care visit) (Adjusted odds ratio (AOR) = 2.6, 95% CI: 1.37–3.84), family wealth index (AOR = 2.72, 95% CI: 1.89–3.55), maternal education attainment (AOR = 3.03, 95% CI: 2.24–3.82), residence (urban dwellers) (AOR = 4.06, 95% CI: 0.95–7.17), and confidentiality antenatal care (AOR = 2.23, 95% CI: −0.36 to −4.82).
Conclusions:
The study found regional and country-level disparities in the quality of antenatal care services for pregnant women, where poor-quality antenatal care services were provided for more than two-thirds to three-fourths of antenatal care attendants. Therefore, policymakers and health planners should put a great deal of emphasis on addressing the quality of antenatal care services.
Plain language summary
This study aimed to estimate the magnitude, disparity, and predictors of the quality of antenatal care services. A comprehensive literature search was conducted from August 24/2022 to September 08/2022 found that a total of 76 studies with a sample size of 940,164 were included in the final analysis. The global pooled poor quality of antenatal care service utilization was 64.28%. The study found that nearly two-thirds of pregnant women worldwide received poor-quality antenatal care services, and nearly 3/4th of pregnant women in Ethiopia received poor-quality ANC. This study discovered continental, regional, and country-level disparities in the quality of antenatal care services, with pregnant women in the Asian, African, and South American continents using low-quality antenatal care services compared to those in North America and Europe. The authors strongly recommend providing high-quality antenatal care based on WHO recommendations globally for pregnant women in need of quality services at all levels to provide quality healthcare to the target population.
Background
Maternal and neonatal health remain a global agenda. 1 Despite tremendous advances in healthcare, over 295,000 women died during and after pregnancy and delivery in 2017, particularly in ‘low- and middle-income nations’. Additionally, 2 million stillbirths occur annually, one occurring every 16 s, a tragedy that can be averted with better quality care.2,3 In addition, nearly 2/3rd of ‘maternal and neonatal health burdens’ can be alleviated through optimum antenatal care (ANC).4–6
‘ANC’ is healthcare provided by skilled professionals to pregnant women and adolescent girls to ensure optimal health conditions during pregnancy. It reduces maternal and perinatal morbidity and mortality by detecting and treating pregnancy-related complications and identifying those at increased risk during labor and delivery.7–10
‘Globally, 85% of pregnant women attend at least one ANC’ visit with a skilled health professional, with 58% attending at least four ANC visits. However, utilization varies between countries, with 18% in Guatemala and 81% in Nicaragua. ‘Quality of care during ANC visits’ is crucial, especially in low-resource settings, where barriers exist to providing high-quality care. 11 Women in ‘developing countries’ receive higher quality ANC than ‘women in developed countries’. The range of quality ANC was reported to range from 2.5% in Uganda to 97.5% in Scotland.12,13
‘The World Health Organization’ has defined quality ANC as the degree to which maternal and newborn health services (for individuals and the population) increase the likelihood of timely and appropriate care to achieve desired outcomes that are both consistent with current professional knowledge and consider the preferences and aspirations of individual women and their families. 14 ANC is crucial for reproductive, maternal, newborn, and child health. Integrating ANC with other health services enhances its utilization, quality, and outcomes. Quality ANC allows for screening for chronic conditions and non-communicable diseases. However, ‘shortages of essential medicines, equipment, and trained staff hinder high-quality care in low-resource settings’. 15 ‘High-quality ANC’ is associated with improved maternal, fetal, and neonatal outcomes. Thus, close monitoring of ANC quality and delivery models is one of the key elements of successful programs that benefit the health and well-being of women, their newborns, and their families. 16 A full evaluation of care delivery models is required to establish the acceptability, accessibility, availability, and quality of ANC service delivery is very crucial. 16 Several studies have assessed the overall quality of global maternal neonatal health (MNH) services. Some studies have reported dissatisfaction with both clients and care providers regarding the existing Quality of Care. 17 Several authors have proposed various quality indicators for ANC. Some studies have proposed binary or categorical classifications considering the number of interventions received by pregnant women. In most studies, good ANC quality was defined as having received all or most of the components considered.18–21 However, quality ANC is difficult to define owing to the complex nature of the concept, and it is challenging to measure it directly. 22 Hence, researchers have followed several approaches to systematically measure the processes of different MNH services.18–21 These inconsistent approaches to measuring ANC quality pose challenges to programmers and policymakers. Hence, it is important to obtain a pooled estimate of the quality of ANC. However, to the best of our knowledge, no systematic review or meta-analysis has been conducted to estimate the pooled quality of ANC worldwide and across regions. Therefore, considering the scarcity of evidence on the quality of ANC, this study aimed to fill this knowledge gap. Hence, programmers and policymakers rely on the evidence from their businesses. Furthermore, researchers can gain insights into another research question to further study the quality of ANC. This systematic review and meta-analysis aimed to enable governments, policymakers, health professionals, and reproductive-age populations to inform themselves about the importance of high-quality ANC service utilization and delivery of high-quality essential components of ANC services and to evaluate changes and trends in quality ANC service utilization over time.
The objectives of this review were
To conduct a systematic review of poor-quality ANC service
To conduct meta-analysis of pooled estimate magnitude of poor-quality ANC service
To compare regional disparities of poor-quality ANC service
To identify pooled predictors of good-quality ANC service
Methods
Protocol and registration
The protocol was registered as PROSPERO Registration Number: CRD42022365349 in the International Prospective Register of Systematic Reviews (PROSPERO).
Information source and search strategies
We followed the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guideline 23 to prepare the whole document. National surveys and published and unpublished articles were obtained from different databases. In addition, the reference lists of the included articles were checked to identify those that were not assessed in the search strings. We sought for comprehensive literature research published on PubMed, CINAHL (EBSCOhost), Global Health (CABI), Medline (EBSCOhost) and other sources (Google Scholar and Google) since 2002 (date of launch of the WHO basic ANC model) to September 08/2022 that reported prevalence of quality of ANC, or ‘prenatal care’, or ‘focused ANC service delivery’ has been included in this systematic review and meta-analysis.
The appropriateness of the key terms was checked before conducting searches in each database. Examples of search strings in PubMed: ((((Antenatal Care) OR (“Prenatal Care” [Mesh])) OR (Focused Antenatal Care Service Delivery)) AND (“Quality of Health Care” [Mesh]) AND ((2002 [Filter]) AND (filter [Filter]) AND (humans [Filter]) AND (female [Filter]) AND (data[Filter]))). Boolean operators AND and OR were used (Supplemental File Appendix 1).
Predictors, determinates, associated factors, ANC, Quality, and Ethiopia, were used in the search process. The Boolean operators AND and OR were used accordingly. PubMed search strings were (((((((determinants) OR (Predictors)) OR (“associated factors” [Mesh])) AND (“Quality” [Mesh] OR “Antenatal Care” [Mesh])) OR (Prenatal Care)) AND (“Focused Antenatal Care” [Mesh])) OR (ANC) AND (“Ethiopia” [Mesh]) (Supplemental File Appendix1).
Eligibility criteria
Inclusion criteria
The question format for this meta-analysis was as follows: Condition, Context, and Population (CoCoPop). 24 The CoCoPop framework used for reviews addressing a question relevant to the prevalence Quality of ANC; (a) Condition (Quality of ANC, or ‘prenatal care’, or ‘focused ANC’); (b) Context global, regional and national, study design (cohort studies, cross-sectional studies, epidemiology, observational studies), study setting (community-based surveys, health institutions, web-based surveys) and (c) population pregnant women attended ANC. Data from each study were verified for eligibility using the study area, study setup, assessment methods, study designs, titles, abstracts, and full texts. Observational studies reporting the magnitude of quality of ANC among pregnant women and Journal Articles in the last 20 years, gray literature, English language, and study settings in any country across the globe were included.
Exclusion criteria: The same patients were enrolled in different articles, commentaries, editorials, case reports, letters, family-based studies, and short communication.
Nonetheless, studies with incomplete or unclear quality of ANC/service operational definitions and those without full text were excluded. Letters to the editors, conference proceedings, and qualitative studies were excluded. EndNote X8 reference manager was used to manage the articles.
Selection process of studies
The selection of studies (i.e., identification, screening, and ensuring eligibility) was carried out by the investigators. The research team member were involved in the identification and screening of studies independently. Studies selected for retrieval was again assessed for methodological quality prior to inclusion. The assessment was done using relevant standardized critical appraisal instruments from the Joanna Briggs Institute, JBI Critical appraisal checklist (Supplemental File Appendix 1).
Data extraction procedures
Data were extracted by two independent investigators (Dereje Bayissa Demissie and Firew Tiruneh) to assess the quality of the study, and a third author (Abebe Sorsa Badacho) resolved any inconsistencies.
Inter-rater agreement was computed by the author (DBD) before inclusion in this study was made. Inter-rater agreement was computed using Cohen’s kappa coefficient (κ). The findings revealed a substantial agreement 25 between the two raters (κ = 0.712, p < 0.01).
The extracted data included first author’s name, publication year, continent, study country, study period, study design, sample size, prevalence of poor antenatal quality, and number of poor antenatal quality. The data were summarized using a Microsoft Excel 2016 spreadsheet (Supplemental File Appendix 1).
Quality assessment
The quality of the study was assessed using the Joanna Briggs Institute (JBI) critical appraisal tools, 26 and the results were graded as low, medium, or high if the quality score was <60%, 60%–80%, or >80%, respectively. We inspected the funnel plot and conducted Egger’s regression tests to assess publication bias. 27
Publication bias and heterogeneity
Funnel plots and Egger’s regression test were used to measure publication bias at the 5% significance level. 28 In addition, heterogeneities among the studies used to compute the pooled estimates in this meta-analysis were explored using forest plots, I2 tests, and Cochrane Q statistics. 29 I2 values of 25%, 50% and 75% were interpreted as indicating low, medium and high heterogeneity, respectively. 30 The current meta-analysis considered significant heterogeneity when the I2 value was ⩾50%, with a p-value < 0.05. We inspected the funnel plot and conducted Egger’s regression tests to assess publication bias. 27 A trim-and-fill analysis was conducted to adjust for publication bias. 31 The possible sources of significant heterogeneity were addressed through subgroup and sensitivity analyses.
Outcome and summary measures
The primary outcome of this study was quality of ANC, or ‘prenatal care’ or ‘focused ANC service delivery’. The CoCoPop framework was used for reviews that addressed questions relevant to ANC quality. CoCoPop represents conditions, context, and population. 24 Condition refers to the quality of ANC, or ‘prenatal care’ or ‘focused ANC service delivery’ measured based on the world health organization. Quality ANC receipt of all essential components of ANC services, such as blood pressure measurements, blood tests, urine tests, information on possible complications, counseling on nutrition, and advice on birth preparedness plans during pregnancy.21,32,33
Context Global level, regional, and national pooled prevalence of poor-quality ANC services utilization and the population of pregnant women attending ANC services. 34
The primary objective of this study was to estimate the global quality of ANC services for pregnant women. The pooled prevalence of poor-quality ANC services was computed for global, developed, low- and middle-income, African, and Ethiopian countries.
Data synthesis and statistical analysis
Pooled estimates were calculated using the STATA version 16 software (STATA Corporation, College Station, TX, USA). Both random- and fixed-impact methods were used to measure the pooled estimates. The pooled estimates were computed using ‘metaprop’ using a sample size as a weight (wgt) variable with 95% CIs. Pooled estimates were computed using random-effects models and weighted using the inverse variance method in the presence of high heterogeneity among studies. Subgroup analyses were performed using different parameters (continent and country). We verified the appropriateness of each datum prior to analysis. Forest plots, summary tables, and text are used to present the findings of this study.
Results
Selection of studies
In the initial search, 9695 studies were obtained from databases and gray literature sources. First, 1840 studies were excluded because of duplication. Then, 7855 studies were screened using titles and abstracts, and 7716 were removed. Finally, the full texts of 138 studies were assessed for eligibility. Of the 138 studies, 63 were excluded due to inconsistent results.35–96 Eventually, 76 eligible studies were used in the final analysis of the current systematic review and meta-analysis12,13,18–21,32,97–162 (Figure 1).

PRISMA flow chart showing the study selection process.
Study characteristics
A total of 76 studies with a sample size of 940,164 were included in the final analysis, and 70 studies were conducted in low- and middle-income countries.12,18–21,32,97,99–110,112–116,121–137,139–148,150,152–168 six in developed countries, and in Europe and North America.100,113,120,138,149,151 Of low and middle-income countries (LMIC), 15 studies were conducted in Ethiopia.102–104,118,122,135,140,143,145,146,148,152,157,161,163,168 Four of the 76 studies were multi-country, with a minimum of 25 countries.55,87,111,114,132 In summary, these studies were conducted in 36 countries and 5 continents. All studies were cross-sectional studies, and critical appraisal of cross-sectional studies revealed that approximately 95% of the studies scored high quality, and only 5% scored medium quality (Table 1).
Characteristics of the individual studies on quality ANC services among pregnant women included in the present systematic review and meta-analysis 2022.

Keynotes: Nine East African countries (Burundi, Zimbabwe, Zambia, Uganda, Tanzania, Rwanda, Malawi, Kenya.
The global pooled prevalence of poor-quality ANC services
A total of 76 studies with a sample size of 940,164 were included in the final analysis, with sample sizes ranging from 81 to 190,898.116,107,108,128
Data collected from 940,164 pregnant women of ANC attendants revealed that 630,453 pregnant women utilized poor-quality ANC services, with a highly diverse prevalence ranging from 2.5% in Scotland 151 to 97.47% in Uganda 114 as depicted in Figure 2, from 2008 to 2022.

Trend of poor-quality ANC services utilization globally from 2008 to 2022.
According to the random-effects model, the global pooled poor-quality ANC services was 64.28% (95% CI: 59.58%–68.98%) per 100 pregnant women who underwent ANC (Figure 3).
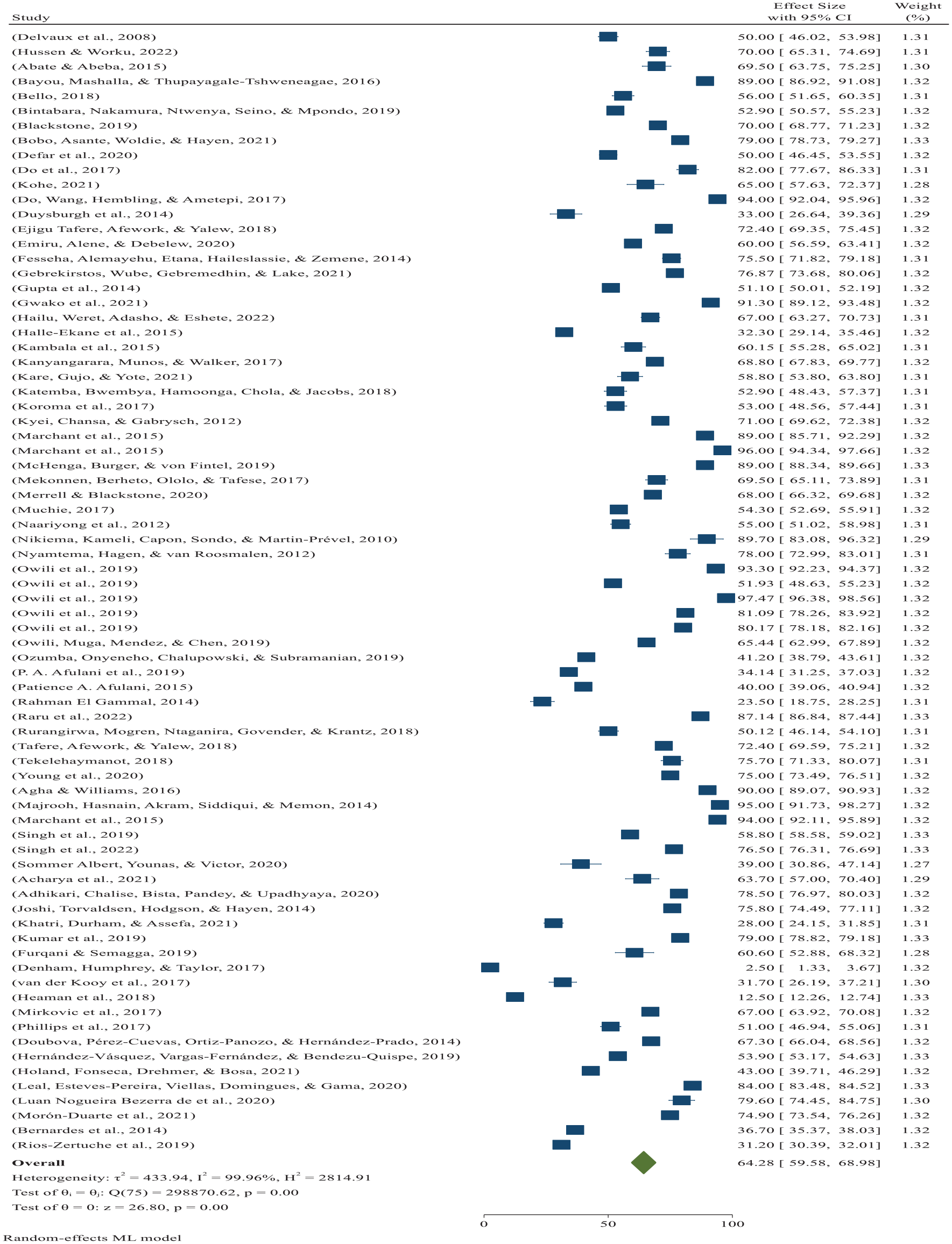
Forest plot showing the global pooled prevalence of poor-quality ANC services per 100 among pregnant women 2022.
There was high heterogeneity among studies (I2 = 99.96%, p = 0.001), and based on the trim-and-fill analysis, the learner estimator imputed 13 studies in the left (observed 76 + imputed 13 = 89 studies), with a global pooled estimate of 58.55% (95% CI: 53.61%–63.49%) after trim-and-fill analysis (Figure 3).
Publication bias was checked using a funnel plot and was objectively verified using Egger’s regression test. Hence, the funnel plot seemed asymmetric despite Egger’s regression test (p = 0.1233), which did not confirm the asymmetry of the funnel plot (Figure 4). Finally, the funnel plots appear asymmetric pinpointed to the right for global pooled poor-quality ANC (see Figure 4), which is confirmed by the Fisher fail safe-N-P (Chi-square test = 0.00) analysis finding warrants the acknowledgment of possible publication bias within the article, which revealed the existing body of literature.

Funnel plot showing the distribution of included studies global pooled prevalence of poor-quality ANC services per 100 pregnant women 2022.
Sensitivity analysis was also performed to identify the possible sources of heterogeneity among the included studies. However, no single study has shown a remarkable effect on the heterogeneity of the pooled estimates (Figure 5).
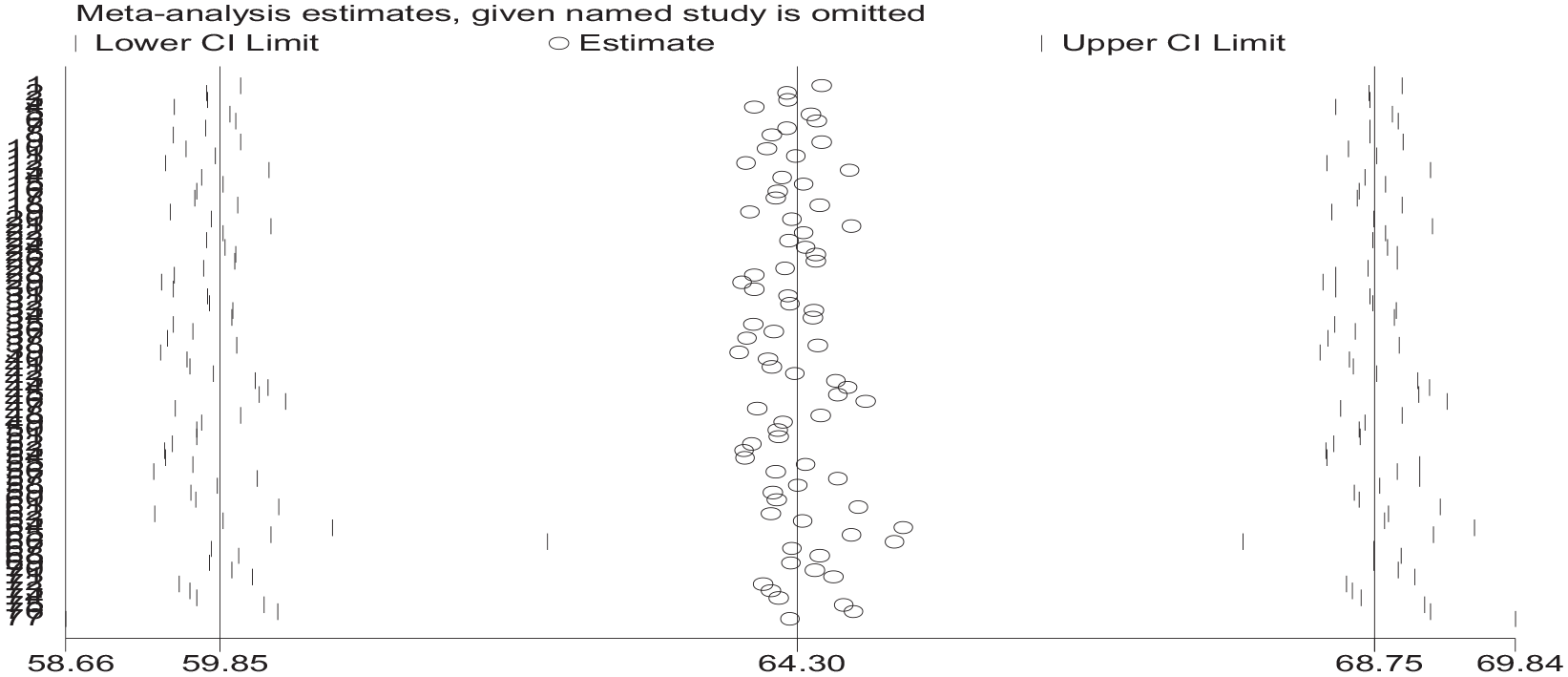
Sensitivity analysis to identify the possible source of heterogeneity 2022.
Based on nonparametric trim-and-fill analysis of the publication bias linear estimator imputed on the remaining 13 studies (observed 76 + imputed 13 = 89 studies) after trim-and-fill analysis, the global pooled estimate of poor-quality ANC services was 58.55% (95% CI: 53.61%–63.49%). As shown in Figure 6, the funnel plots appeared symmetric after trim-and-fill analysis of the linear estimator imputed 13 studies on the left global (see Figure 6).

Funnel plot showing the distribution of included studies of the global pooled prevalence of poor-quality ANC services per 100 pregnant women in 2022.
This study performed a subgroup analysis to estimate the pooled prevalence of poor ANC services per continent, WHO ANC implementation guidelines based on publication year, and country. 14
We conducted a continental subgroup analysis, which revealed that 12 studies were conducted in Asia, with a pooled prevalence of 70.07% (95% CI: 58.784%−81.364%) (I2 = 99.99%, p = 0.001), and 51studies were done in Africa, with a pooled prevalence of poor ANC services of 66.87% (95% CI: 61.908%−71.84%) (I2 = 99.86%, p = 0.001) Figure 7.

Subgroup analysis to estimate the pooled prevalence of poor ANC services based on continent pooled prevalence of poor-quality ANC services per 100 pregnant women 2022.
The prevalence of poor-quality ANC in developed countries (North America and Europe)
Subgroup analysis was computed based on the World Bank’s classification of countries; six studies were done in developed countries (North America and Europe) with a total sample size of 78,388 pregnant women of ANC attendants revealed that 13,422 pregnant women utilized poor-quality ANC services, with highly diverse poor-quality ANC services prevalence ranging from 2.5% in Scotland 151 to 67.3% in Mexico. 149 Based on the random-effects model, the pooled poor-quality ANC services in developed countries was 38.65% (95% CI: 18.42%−58.88%) per 100 pregnant women who attended ANC (Figure 8).
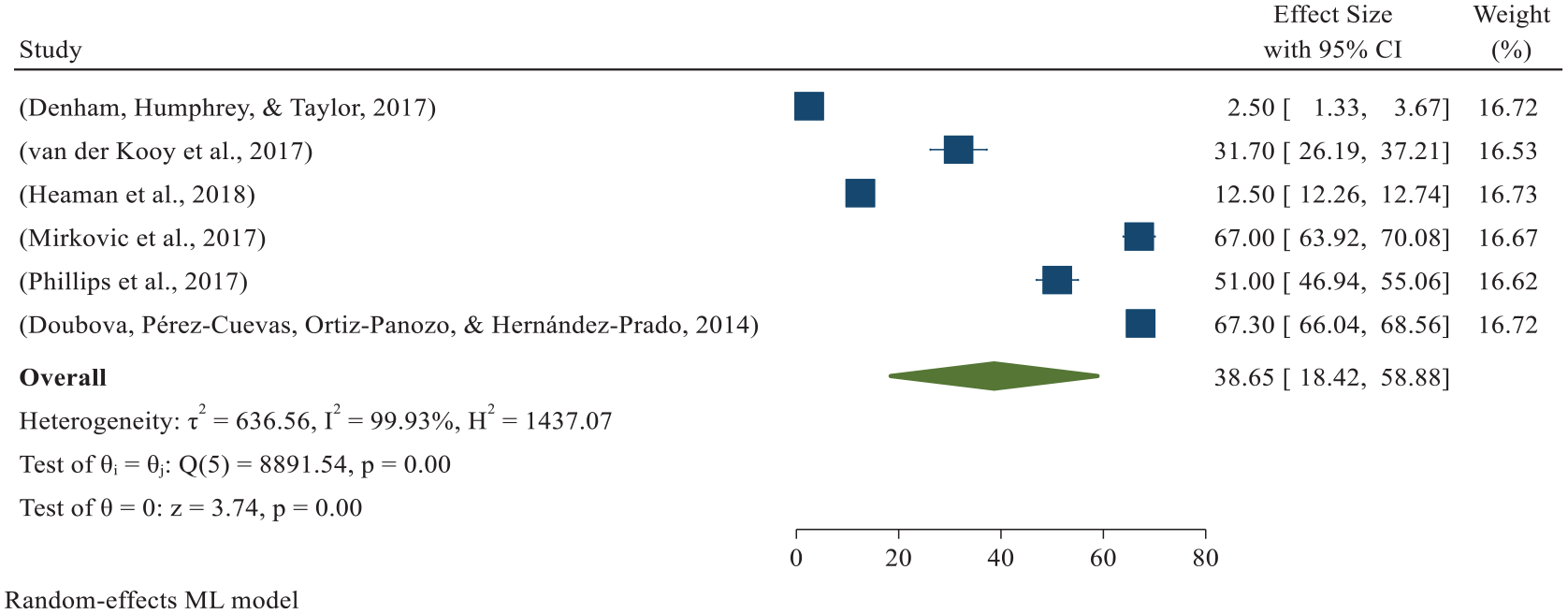
Forest plot showing the developed country (North America and Europe) pooled prevalence of poor-quality ANC services per 100 pregnant women in 2022.
There was high heterogeneity among studies (I2 = 99.93%, p = 0.001), and based on the trim-and-fill analysis, the learner estimator imputed zero studies (observed 6 + imputed 0 = 6 studies); the high-income countries pooled did not change after the trim-and-fill analysis.
Publication bias was checked using a funnel plot, which was objectively verified using Egger’s regression test (p = 0.517) to confirm that there was no publication bias, and funnel plots appeared symmetric for the developed countries pooled with poor-quality ANC services (see Figure 9).
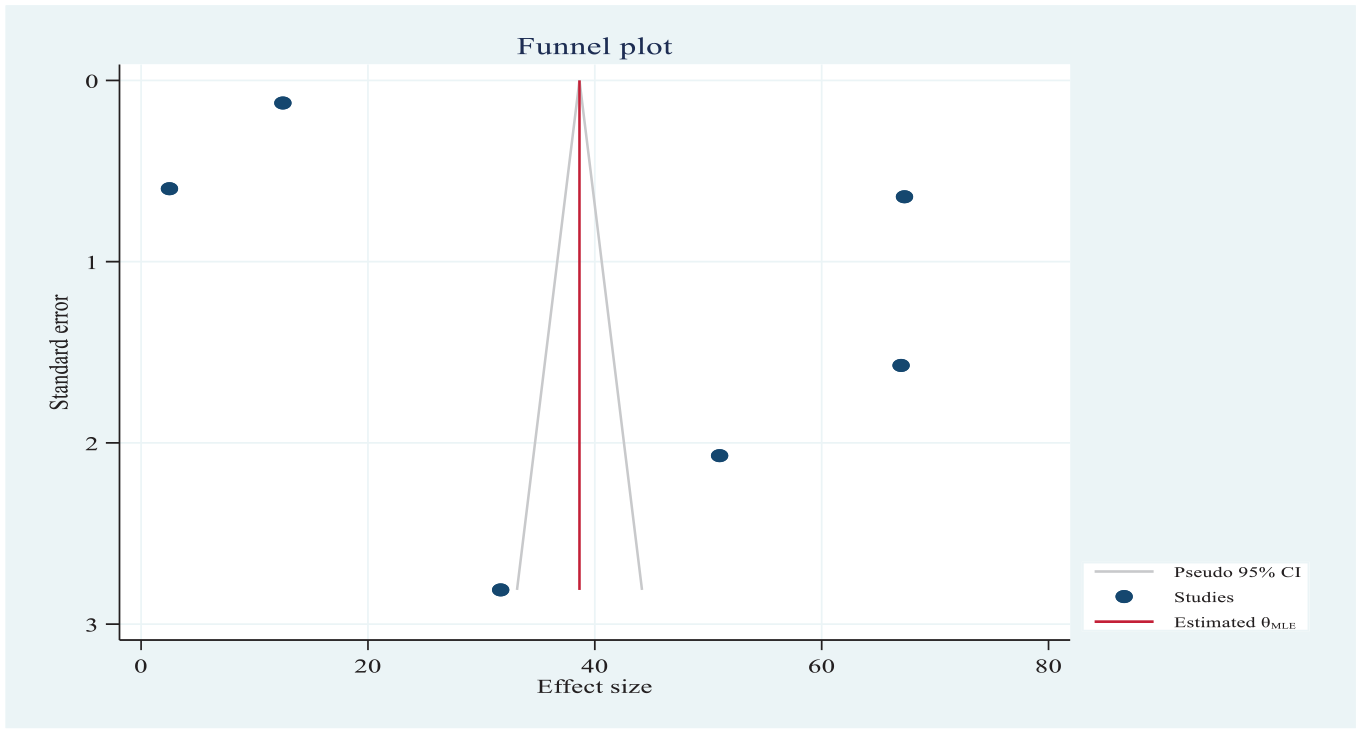
Funnel plot showing the distribution of included studies of the global pooled prevalence of poor-quality ANC services per 100 pregnant women in 2022.
Pooled estimates of poor-quality ANC in low and middle-income countries
Of total, 76 studies were included in the meta-analysis. The majority (70 studies) of the 76 studies included in the meta-analysis were conducted in low- and middle-income countries with a weighted sample size of 861,776 pregnant women of ANC attendants and revealed that 617,031 pregnant women utilized poor-quality ANC services. The prevalence of highly diverse, poor-quality ANC services ranges from 23.5% in Egypt 112 to 97.47% in Uganda. 114
Based on the random-effects model, the low- and middle-income countries pooled poor-quality ANC services at 66.26% (95% CI: 61.81%–70.71%) with I2 = 99.95% (p = 0.001) per 100 pregnant women ANC attended (Figure 10). There was significant heterogeneity among studies (I2 = 99.95%, p = 0.001), and based on the trim-and-fill analysis, the learner estimator imputed 13 studies on the left (70 + imputed 1 = 71 studies), and the low and middle-income countries (LMICs) pooled estimate was 66.019% (95% CI: 61.563%–70.475%) after trim-and-fill analysis.
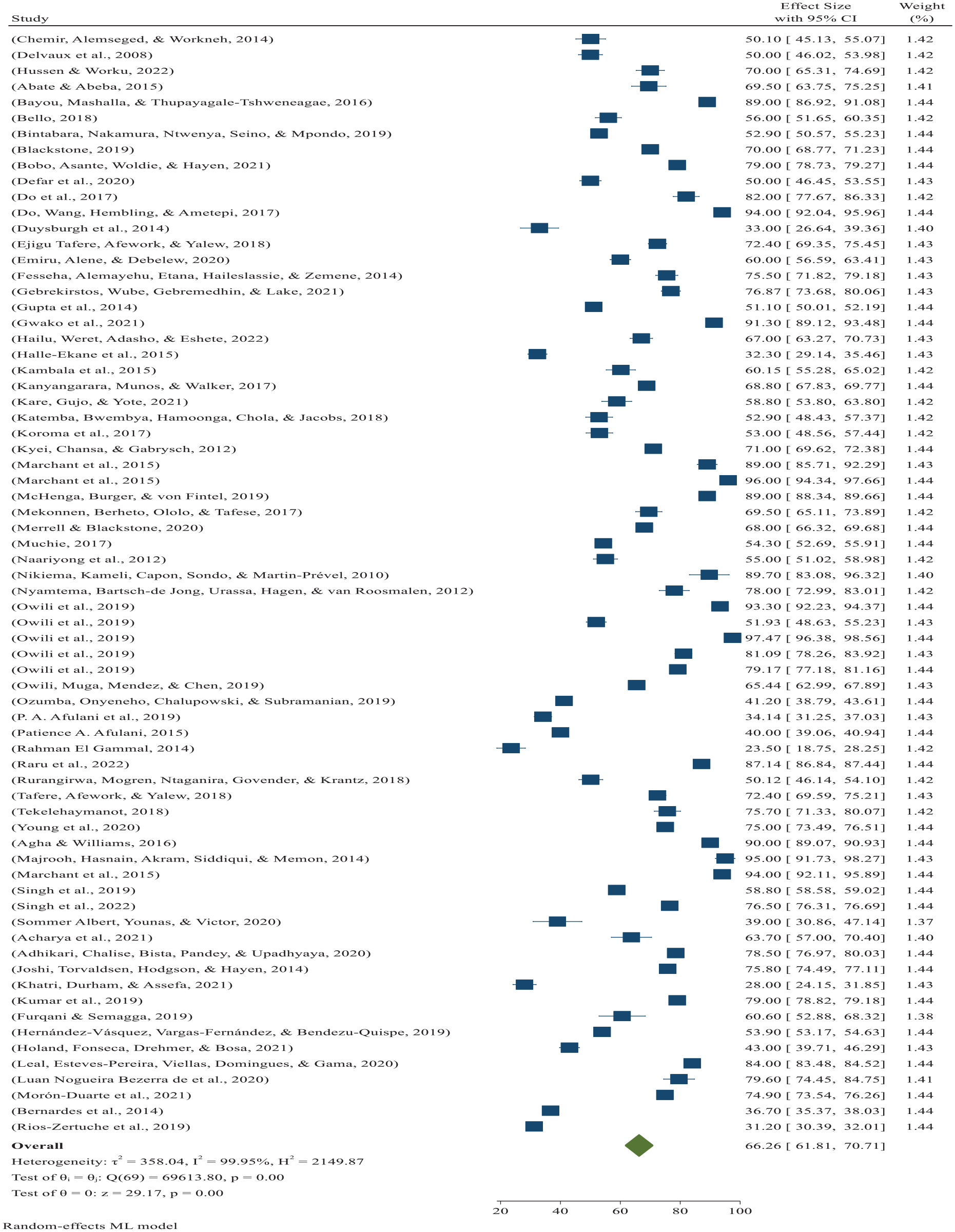
Forest plot showing LMICs pooled prevalence of poor-quality ANC services per 100 pregnant women 2022.
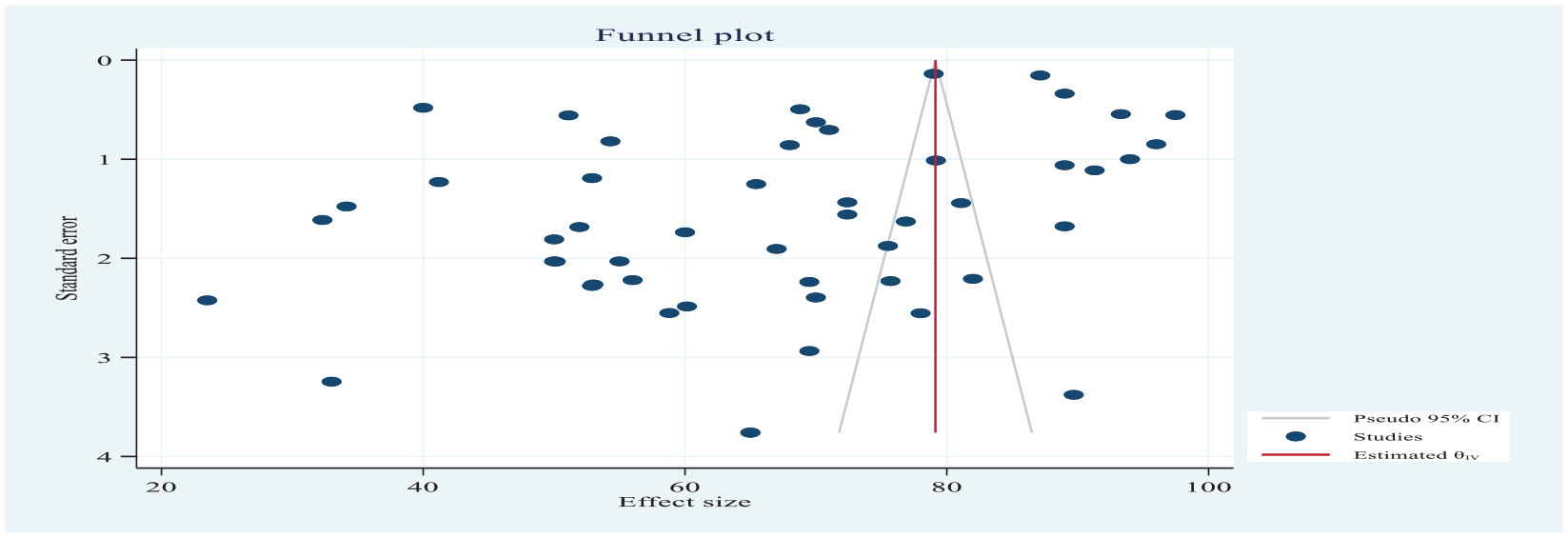
Publication bias was checked using funnel plots looking asymmetrically pinpointed to the right and was objectively verified using Egger’s regression test to confirm publication bias (p = 0.0209), which revealed that the current body of literature is detailed in Figure 11.

Funnel plot showing the distribution of included studies LMICs pooled prevalence of poor-quality ANC services per 100 pregnant women 2022.
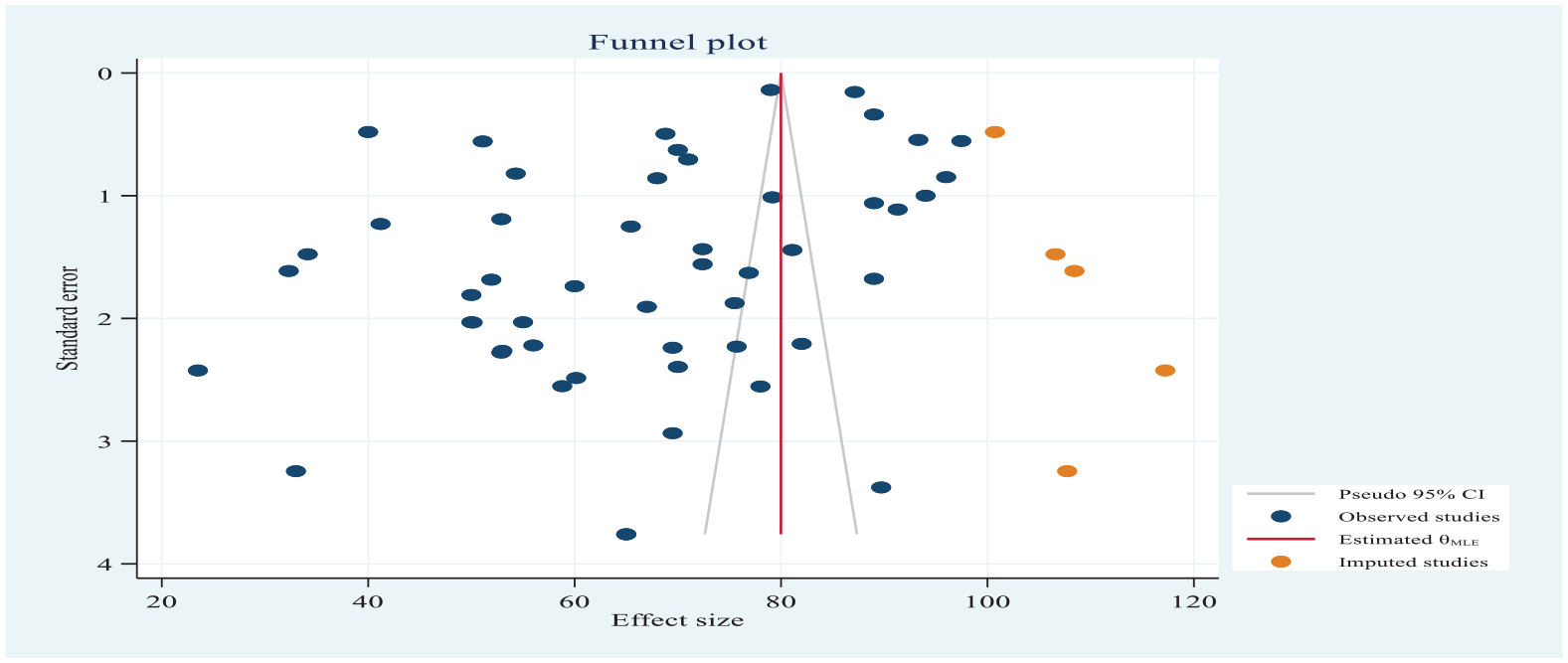
There was high heterogeneity among studies (I2 = 99.95%, p = 0.001), and based on the trim-and-fill analysis, the learner estimator imputed 13 studies on the left (70 + imputed 1 = 71 studies); the LMICs pooled estimate became 66.019% (95% CI: 61.563%–70.475%) after trim-and-fill analysis.
As in Figure 10 belows, the funnel plots appeared symmetric after trim-and-fill analysis of the linear estimator imputed one study on the left global pooled prevalence of quality ANC (Figure 12).

Funnel plot after trim-and-fill analysis of linear estimator in LMICs pooled prevalence of poor-quality ANC services per 100 pregnant women 2022.
Africa continent pooled poor-quality ANC
Of a total of 70 studies from LMICs, 51 studies conducted in Africa with a weighted sample size of 213,409 pregnant women of ANC attendants revealed that 160,496 pregnant women utilized poor-quality ANC services, with highly diverse poor-quality ANC service prevalence ranging from 23.5% Egypt 112 to 97.47%. 114
Based on the random-effects model, the African continent pooled poor-quality ANC services at 66.66% (95% CI: 61.70%–71.62%) with I2 = 99.96% (p = 0.001) per 100 pregnant women ANC attended (Figure 13).

Forest plot showing Africa continent pooled prevalence of poor-quality ANC services per 100 among pregnant women 2022.
Publication bias was checked using funnel plots looking asymmetrically pinpointed to the left and objectively verified using Egger’s regression test. Publication bias was detected (p < 0.0432), which revealed the current body of literature (Figure 14).
Forest plot showing the pooled prevalence of poor-quality ANC per 100 among pregnant women in Africa.
The nonparametric trim-and-fill analysis of the publication bias learner estimator imputed six studies on the right (observed 52 + imputed 6 = 58 studies), and the African continent pooled estimate was 79.985% (95% CI: 79.825%–80.146%) after trim-and-fill analysis.
As shown in Figure 15, the funnel plots appeared symmetric after trim-and-fill analysis of the linear estimator, imputing six studies on the right African continent pooled prevalence of quality ANC (Figure 15).
The pooled proportion of poor-quality ANC services in Ethiopia 2022.
Of the 51 studies conducted in Africa, 15 studies were conducted in Ethiopia with a weighted sample size of 120,31 pregnant women of ANC attendants, revealed that 7989 pregnant women utilized poor-quality ANC services, with highly diverse poor-quality ANC services ranging from 50% 153 to 96%. 124 The pooled prevalence of poor ANC services in Ethiopia was 70.52% (95% CI: 64.55%–76.48%), with significant heterogeneity between studies (I2 = 98.37%, p = 0.001) (Figure 16).

Forest plot showing Ethiopia pooled prevalence of poor-quality ANC services per 100 among pregnant women 2022.
Publication bias was checked using funnel plots looking at the asymmetric pin pointed to the left, and it was objectively verified using Egger’s regression test and was not able to detect publication bias (p < 0.237); however, this was confirmed by Fisher fail safe-N-P (Chi-square test = 0.00) analysis findings warrant the acknowledgment of possible publication bias within the article, which revealed the current body of literature (Figure 17).

Forest plot showing the pooled prevalence of poor-quality ANC per 100 among pregnant women in Africa 2022.
The nonparametric trim-and-fill analysis of the publication bias learner estimator imputed six studies to the right (16 + imputed 0 = 16 studies), and the Ethiopian pooled estimate became 73.52% (95% CI: 72.784%–74.257%) after trim-and-fill analysis.
Predictors of good-quality ANC service in Ethiopia
As shown below in Table 2, identified predictors of good-quality ANC service
The summary of the pooled estimates of the AOR per predictors of good-quality antenatal care service in Ethiopia 2022.

As the table depicted, the identified pooled predictors of good-quality ANC service were the number of ANC visits (fourth and above), family wealth index, maternal education attainment, residence (urban dwellers), and confidentiality maintained during ANC follow-up.
Women who attended the fourth and above ANC visits were identified in five articles,169–173 with a pooled predictor of 2.6 times more likely to receive good-quality ANC services AOR = 2.6 and (95% CI: 1.37–3.84).
Maternal educational attainment was identified as a factor recorded in five articles,39,143,169,171,172 with an overall predicting 3times higher in primary education and more attained women than their counterparts (OR = 3.03; 95% CI: 2.24–3.82). High family wealth index status was identified as a predictor reported in four articles,143,169–171 which predicted 2.72 times higher in the high family wealth index than in women with a low index (OR = 2.72 and 95% CI: 1.89–3.55). Another factor that predicted good-quality ANC service utilization was residence (urban dwellers) reported in three original articles,39,169,172 with an overall prediction 4 times more likely to utilize good-quality ANC services among urban dwellers than rural dwellers (OR = 4.06, 95% CI: 0.95–7.17). The last factor associated with the pooled prevalence of good-quality ANC service utilization was maintained confidentiality, as stated in two articles,140,173 which revealed that 2.23 times more likely to predict good-quality ANC service utilization as compared to perceived not maintained confidentiality during the provision of ANC services (Table 2).
Women who attended the fourth and higher ANC visit were identified in five articles.169–173 Women who had attended the fourth and above ANC visit were 2.6 times more likely to receive good-quality ANC services AOR = 2.6 and (95% CI: 1.37–3.84) (Figure 15) (I2 = 99.947%, p = 0.00). To identify factors associated with the source of heterogeneity of pooled predictors of fourth and above ANC visits, meta-regression showed a significant association with sample size, study year, and frequency of good-quality ANC.
Of the studies identified, fourth and above ANC visits were positively associated with good-quality ANC services, except for one study, 172 which again negatively predicted good-quality ANC services 0. 5 times more likely to predict a poor-quality ANC services AOR = 0.5 (95% CI: 0.47–0.53) (see details in Figure 18).

The pooled odds ratio of forth and above ANC visit with good-quality ANC services in Ethiopia 2022.
Maternal educational attainment was identified as a factor recorded in five articles.39,143,169,171,172
The odds of good-quality ANC service utilization were three times higher in attained primary education and more women than their counterparts (OR = 3.03 (95% CI: 2.24–3.82) (Figure 18) (I2 = 99.85%, p = 0.00). Of the studies identified forth and higher ANC visits were positively associated with the quality of ANC services.
To identify factors associated with the source of heterogeneity of pooled predictors of maternal education, meta-regression showed that it was significantly associated with sample size, study year, and frequency of good-quality ANC (Figure 19).

The pooled odds ratio of maternal education with good-quality ANC services in Ethiopia 2022.
High family wealth index status was identified as a predictor, which was reported in four articles.143,169–171 The likelihood of utilizing good-quality ANC services in women with moderate to high family wealth indexes was 2.72 times higher than that in women with low family wealth indexes (OR = 2.72; 95% CI: 1.89–3.55) (Figure 17) with (I2 = 99.89%, p = 0.00). To identify factors associated with the source of heterogeneity of pooled predictors of high family wealth index, meta-regression showed a significant association with sample size, study year, and frequency of good-quality ANC (Figure 20).
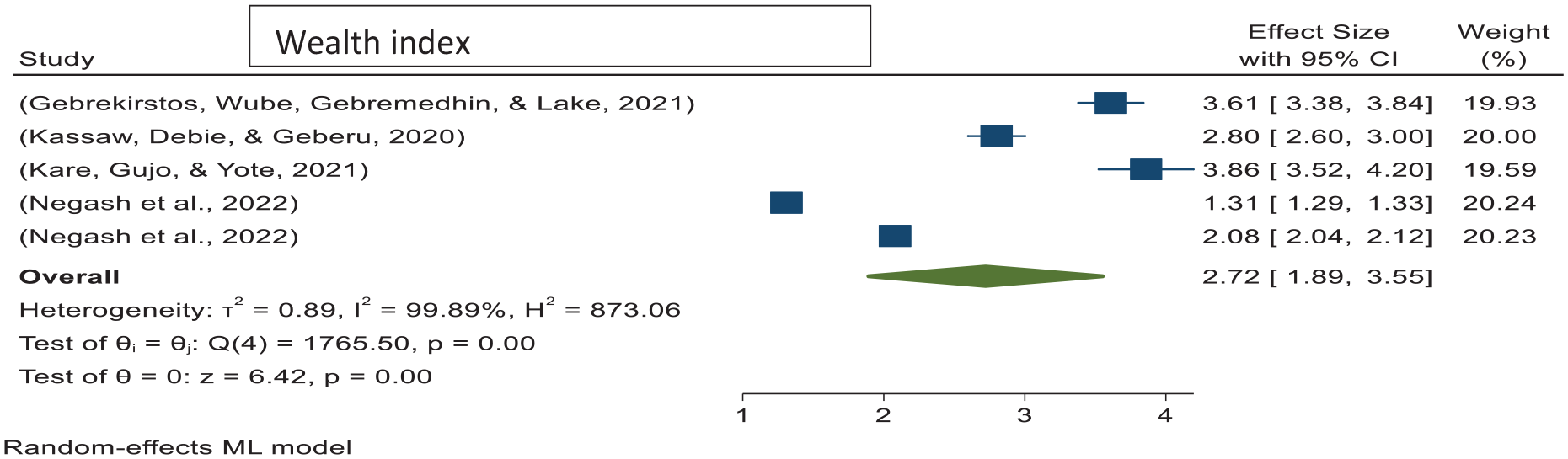
The pooled odds ratio of family wealth indexes with good-quality ANC services in Ethiopia 2022.
Another factor that predicted good-quality ANC service utilization was residence (urban dwellers), which was reported in three original articles.39,169,172 Urban dwellers women were 4times more likely to utilize good-quality ANC services than rural dwellers (OR = 4.06; 95% CI: 0.95–7.17) (Figure 18) (I2 = 99.89%, p = 0.00). To identify factors associated with the source of heterogeneity of pooled predictors of maternal residence, meta-regression showed a significant association with sample size and frequency of good-quality ANC (Figure 21).

The pooled odds ratio of residences with good-quality ANC services in Ethiopia 2022.
The last factor associated with the pooled prevalence of good-quality ANC service utilization was confidentiality, as stated in two articles.140,173 Women who maintained confidentiality were 2.23 times more likely to utilize good-quality ANC services than those who did not maintain confidentiality during ANC service provision (Figure 21). To identify factors associated with the source of heterogeneity of pooled predictors of maintained confidentiality, meta-regression showed a significant association with sample size and frequency of good-quality ANC (Figure 22).

The pooled odds ratio of maintained confidentiality with good-quality ANC services in Ethiopia 2022.
Discussion
Quality ANC has been stipulated as a means of achieving the targets of the SDGs 3.1 and 1.2. Poor-quality ANC is linked to significant maternal and infant mortalities.174,175 There is evidence that quality ANC can avert 2/3 of the maternal and neonatal health burdens. Inconsistent with evidence showing the benefit of quality ANC, the current study revealed gravely concerning findings. 175 This study estimated the global and regional pooled prevalence of poor-quality ANC services among pregnant women based on global and regional data. The results revealed that the global pooled poor-quality ANC services was 64.28% (95% CI:59.58%–68.98%), with heterogeneity among studies (I2 = 99.96%, p = 0.001). Based on the trim-and-fill analysis learner estimator, 13 studies were imputed and the global pooled estimate was 58.55% (95% CI: 53.61%–63.49%). All studies based on the WHO have defined quality ANC as a major component. This definition has received little attention in the measurement of ANC quality.14,176 As a result, except for a few empirical investigations, authors considered studies with little variation in the method and approach of quality ANC measures,32–34,177 findings, supported by review evidence, revealed that poor-quality facility-based care is one of the major contributing factors to the elevated rates of morbidity and mortality among women and newborns in LMIC. Women who perceive the quality of facility-based healthcare to be poor may choose to avoid facilities-based deliveries, which could save their lives. 178
This study revealed regional and country-level disparities, where pregnant women who resided in Asia, Africa, and South America had the highest prevalence of poor-quality ANC services; subgroup analysis revealed that the pooled prevalence of poor-quality ANC was 70.07%, 66.87%, 57.7%, and 38.6% for Asia, Africa, South America, and Europe and North America, respectively. This regional variation revealed that pregnant women from Asia, Africa, and South America received 74% poorer quality ANC than those from Europe and North America. This evidence is strongly supported by a Lancet Commission study that reported 8.6 million deaths from treatable conditions in LMICs, 60% due to poor-quality care. 179 This finding is comparable with other studies that reported that poor-quality ANC is associated with the economy and literacy level of countries. 180 Other studies have also indicated that pregnant women in low- and middle-income countries receive the lowest quality of ANC. This great regional variation due to perinatal regionalization based on leaving no one behind in European member states was implemented by ‘rationalizing existing healthcare services to ensure that each pregnant woman and newborn infant are cared for in an appropriate facility’. The main goal of regionalization is to minimize differences in outcomes attributable to geographic location while helping to contain rising healthcare costs (through economies of scale). 180 The success of health workers cost depends on rapid policy transition, increased funding, effective use of technology, community engagement, referral linkages, public health services, and sustained political will. India’s experience can guide other low and middle-income countries in achieving universal health coverage. 181 Scientific evidence has proven that high-quality ANC is essential to ensure a healthy pregnancy for the mother and baby and an effective transition to positive labor and childbirth.175,180
‘The World Health Organization (WHO)’ has established a framework containing eight quality domains that should be assessed, improved, and monitored within the health system to ‘improve the quality of maternal and newborn care’. This will be applied across the world’s health systems and should provide a ‘structure for access to high-quality care in the two crucial, interlinked dimensions of provision and experience by focusing on six prioritized areas’: ‘clinical guidelines, standards of care, effective interventions, measures of quality, relevant research, and capacity-building to maintain high-quality services’. 14 The quality of ANC in ‘low- and middle-income countries’ is extremely poor. The pooled estimate was far below the planned value. Therefore, progress has been made with expanding coverage of essential interventions in reproductive, maternal, neonatal, child, and adolescent health worldwide. However, a task shift from coverage to quality care is urgently needed to save millions of lives global mothers. 180 Healthcare providers should prioritize culturally appropriate care for women to optimize reproductive health and improve pregnancy outcomes. Prioritizing pre-conception and prenatal care can reduce costs, improve maternal and fetal outcomes, and promote lifelong health. 182 Studies have revelealed that burden of various chronic conditions include hypertension, diabetes, asthma, heart diseases and thyroid disorder have been associated with limited access to quality of care and poor health infrastractures. The authors also highlighted that strengthening primary health systems to enhance clinical condition-related service quality and delivery is imperative.183,184
Of total, 51 studies done in Africa continent, 15 studies were conducted in Ethiopia with a weighted sample size of 120,31 pregnant women of ANC attendants revealed that 7989 pregnant women utilized poor-quality ANC services, with highly diverse poor-quality ANC services prevalence ranges from 50% 153 to 96%. 124 The pooled prevalence of poor ANC services in Ethiopia was 70.52% (95% CI: 64.55%–76.48%). This evidence is supported by a national health survey of five African countries, which revealed that more than 40% scored poorly in basic measures of maternal care. 185 The promising goal of Ethiopia’s Ministry of Health is to achieve three zeros from 2021 to 2025, and zero preventable maternal deaths and morbidities are planned to address this problem by enhancing the quality of ANC in Ethiopia. 186
This meta-analysis identified that the overall pooled predictors of good-quality ANC services were number of ANC visits (fourth and above ANC visits), family wealth index, maternal educational attainment, residence (urban dwellers), and maintained confidentiality during ANC follow-up. These results are supported by the Health Sector Transformation Plan, while other breakthrough studies revealed that health indicators vary significantly by region, place of residence, gender, disability status, education, and socioeconomic status. In general, health benefits are higher for urban dwellers, literates, and wealthier groups.187,188
Strength and limitation
This study was based on individual studies published in English, which may have affected true estimates. The higher heterogeneity observed among the studies might have also affected the estimates.
We attempted to address the high publication bias that may have affected the true estimates in the current study using trim-and-fill analysis. However, the authors were unsure whether the high publication bias was due to the presence of substantial heterogeneity among the studies or unresearched/unpublished studies. Finally, this study should be interpreted with caution, considering the limitations of the data available at the time of publication. These findings should be considered when interpreting the results of this meta-analysis. Although this does not necessarily invalidate our conclusions, publication bias and heterogeneity of the studies are inevitable, regardless of how we try to treat them statistically. Authors would like our readers to consider that the studies included in this meta-analysis are heterogeneous.
Conclusions
The pooled estimate revealed that nearly two-thirds of pregnant women worldwide received poor-quality ANC services. The study found regional and country-level disparities in the quality of ANC services for pregnant women. Ethiopia, Asia, Africa, and South America, where poor-quality ANC services were provided for more than two-thirds to three-fourths of the ANC attendants. Thus, policymakers and health planners should prioritize the quality of ANC services as current international and national public health agendas to reduce maternal and neonatal mortality and morbidities as per the sustainable development goals plan.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241248275 – Supplemental material for Magnitude, disparity, and predictors of poor-quality antenatal care service: A systematic review and meta-analysis
Supplemental material, sj-docx-1-smo-10.1177_20503121241248275 for Magnitude, disparity, and predictors of poor-quality antenatal care service: A systematic review and meta-analysis by Dereje Bayissa Demissie, Gebeyaw Molla, Firew Tiruneh Tiyare, Abebe Sorsa Badacho and Ashenif Tadele in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121241248275 – Supplemental material for Magnitude, disparity, and predictors of poor-quality antenatal care service: A systematic review and meta-analysis
Supplemental material, sj-docx-2-smo-10.1177_20503121241248275 for Magnitude, disparity, and predictors of poor-quality antenatal care service: A systematic review and meta-analysis by Dereje Bayissa Demissie, Gebeyaw Molla, Firew Tiruneh Tiyare, Abebe Sorsa Badacho and Ashenif Tadele in SAGE Open Medicine
Footnotes
Acknowledgements
Our acknowledgement goes to the authors of the primary studies included in this study.
Author contributions
DBD conceptualized, designed, and drafted the manuscript. DBD and FTT performed article search, data extraction, and quality assessment. DBD and FTT conducted data analysis and wrote the manuscript. ASB. AT and GM have reviewed the manuscript. All authors read, reviewed, and approved the final manuscript.
Availability of data and materials
All data generated or analyzed during this study are included in this article and its supplemental information files.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.