
Abstract
Introduction:
Cooking Online With a Chef (COWC) is a live, telemedicine module delivered by a health coach chef to participants who log in from their home kitchen. Our purpose is to identify health professionals’ perceptions on its educational value and to determine feasibility for clinical practice.
Method:
Sixty-four health care professionals participated in a 75-minute COWC module as active participants during a live remote Continuing Medical Education (CME) program that includes five 75-minute telemedicine sessions. Post-program questionnaire elicited feedback on the module educational value and relevance to clinical practice through Likert-type scale and open-ended questions. This report presents descriptive analysis of the Likert-type scale questions and thematic qualitative analysis of the open-ended question.
Results:
Seventy percent of health care professional participants rated the quality of the COWC module as either very good or excellent, and 73% rated its relevance to clinical practice as very good or excellent. Open-ended question feedback showed appreciation of the learning experience with specific suggestions about how to improve participants’ preparation for the module.
Conclusions:
The COWC telemedicine module was well received by self-selected health care professionals. Future studies are being planned to determine the efficacy of the module on patients’ nutrition.
Introduction
Suboptimal nutrition is a major public health threat. Hands-on home cooking interventions have been recently proposed as a strategy to improve adherence to nutritious diets. 1 Home cooking is defined as “the actions required for preparing hot or cold foods at home, including combining, mixing and often heating ingredients.” 2 Potential benefits of increased home cooking include healthier dietary patterns (e.g., family meals, eating breakfast), consuming fewer calories and smaller portions, and eating less fat, salt and sugar, and more fruits and vegetables. 3 Indeed, positive correlations have been demonstrated between frequency of home cooking and consumption of healthy food choices, weight status, and body fat.1,4 Unfortunately, during the last decade, both a decrease in home food preparation 5 and an increase in ultra-processed food (i.e., formulated from industrial ingredients that contain little or no intact foods) 6 consumption have occurred. 6 In this context, there is a growing interest in culinary interventions that focus on home cooking as a way to improve eating habits and adherence to nutritious diets.7,8
Most health-related culinary programs include “hands-on” modules in teaching kitchens—a model that presents challenges for scalability, including low accessibility and high costs. 9 To address these barriers, we leveraged the increasing interest in telemedicine-based solutions (i.e., telecommunications technologies to provide medical information and services) 10 and developed a low cost, scalable model named culinary coaching (CC) that combines culinary skills training with health coaching techniques as a unique 2-pronged telemedicine approach to improve nutrition.11,12 Phase 1 of this model includes culinary videos, combined with live, real-time coaching discussions using an off-the-shelf videoconference software (i.e., Zoom). Our preliminary results demonstrated that the CC telemedicine model is feasible,11,12 has potential to improve participants’ home cooking habits, 12 and metabolic outcomes, 12 and that providers can adopt CC principles in their practice. 13
Our next step in developing the CC telemedicine model is to improve the culinary training delivery (i.e., culinary videos), by developing a 60-minute module that provides live remote home cooking education to participants in their home kitchen. This report describes the Cooking Online with a Chef (COWC) module and presents health care professional perceptions on its educational value and potential use in clinical practice.
Methods
Setting
“Lifestyle Medicine: Tools for promoting healthy change” is a Continuing Medical Education (CME) course, which is offered through Harvard Medical School, Department of Physical Medicine and Rehabilitation. 14 The course includes professional training in nutrition which is focused on home cooking and delivered as a 9-hour onsite course followed by 5 optional 75-minute post-conference remote small group practice sessions, which are limited to 8 participants in each group. 12
Structure and content of the module
A 60-minute COWC module was designed around a standard home kitchen (e.g., a stove, an oven, and basic kitchen equipment) that was equipped with 2 streaming enabled devices aimed at streaming the session delivered by a health coach chef: (1) a smartphone mounted on the kitchen cabinet with its camera directed to the cutting board for visual streaming and (2) a laptop with an ear-set that was used to stream the audio and for monitoring. For the delivery of the session, the health coach chef logged in from the teaching station, and participants logged-in to a live-stream cooking class from their home kitchen using a streaming device (e.g., smartphone, iPad, laptop).
During the COWC module, the health coach chef cooked 3 recipes while (1) demonstrating key steps on the cutting board and (2) providing explanations about both the cooking process and how to apply it to the participants daily cooking. Content areas included (1) healthy cooking skills (e.g., grilling vs frying, cooking legumes, increase the use of vegetables, cooking with plant-based fats), (2) techniques to decrease cooking time (e.g., batch cooking, leftovers, repurposing, staple ingredients), and (3) principles in ingredient substitutions (in case of different food preferences or food allergies)
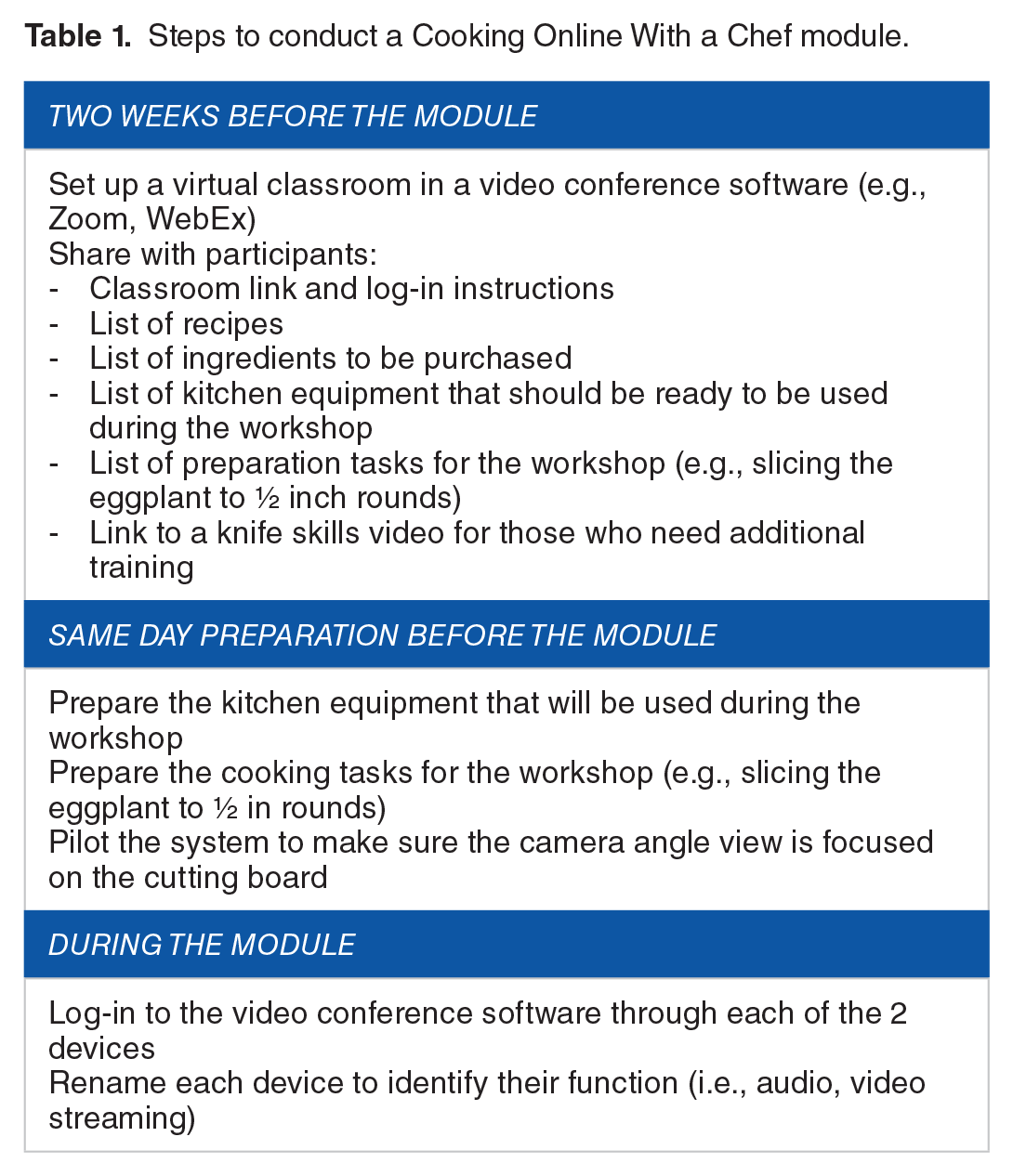
Few weeks prior to the delivery of the module, participants received preparation instructions (e.g., recipes, shopping and kitchen utensils lists, ingredient preparation instructions). During the module, participants followed the health coach chef’s cooking instructions from their own home kitchen and made the same 3 recipes. Although participants were able to view the streamed image of the health coach chef cutting board (Figure 1 provides example that depicts what participants see) and to ask questions through a chat box, the health coach chef could not see participants cooking. A teaching assistant logged in from her desk remotely, to collect questions from the chat box and to present them to the health coach chef throughout the session (Table 1 provides a detailed description on setting and operating a COWC module).

Example that depicts what participants see during the Cooking Online With a Chef module.
Steps to conduct a Cooking Online With a Chef module.
Procedure
At Lifestyle Medicine: Tools for promoting healthy change 2018 conference, one of the 75-minute post-conference remote small group practice sessions was devised to introduce health care professionals to the COWC module and its potential use. Therefore, this practice session was designed to include a 60-minute COWC module, in which health care professionals were experiencing the module as active participants, followed by a 15-minute discussion, facilitated by the health coach chef, focusing on how the module can be implemented in clinical practice. This project was undertaken as a quality improvement initiative at Spaulding Rehabilitation Hospital and as such was not formally supervised by the institutional review board per their policies.
Measure
Following the course, participants completed a generic questionnaire, which was developed by the Department of Postgraduate Medical Education, Harvard Medical School, and is being used with several other CME programs. It included 2 Likert-type scale questions to elicit feedback on the quality of the COWC tele-training module and its relevance to clinical practice (1 = poor; 5 = excellent); and 1 open-ended question to collect general comments about the COWC module.
Analysis
Likert-type scale and open-ended answers were collected and entered into an Excel spreadsheet (Excel 2010; Microsoft Corp., Seattle, Washington). Then, Likert-type scale answers were analyzed using descriptive analysis, and open-ended answers were analyzed by hand using thematic, qualitative content analysis principles 15 by 2 researchers including one who is a professional qualitative researcher. First, following the investigator triangulation guidelines, 16 each researcher marked key phrases through all open answers separately and compiled a list of meaning units (codes) that were abstracted into categories. Then, categories were compared and discussed until agreement was reached and a list of common categories was compiled. Finally, the categories were formulated into 2 main themes: food preparation and educational experience. We summed up the content from the categories in each theme and added appropriate quotes.
Results
Sixty-four health care professionals (8 groups of 8 participants; the program capacity) joined the optional 75-minute post-conference remote practice sessions and 36 (58%) completed the evaluation form. Of these, 23 (64%) were physicians, and the rest were allied health care professionals. Six (17%) had been in practice for more than 30 years, 7 (19%) for 20 to 30 years, 15 (42%) for 10 to 20 years, and 8 (22%) for less than 10 years. Attitudes distribution regarding the COWC module educational quality and relevance to clinical practice are presented in Figure 2. Seventy percent of health care professionals rated the educational quality of the COWC module as either very good or excellent, and 73% rated its relevance to their clinical practice as very good or excellent.

Attitude about the Cooking Online With a Chef module.
Thirteen participants (39% of responders) provided answers to the open-ended question. Overall, health care professional participants perceptions about their learning experience were positive “The camera on top of the dish/cooking counter idea was AWESOME,” including interest to implement the module in practice “I would love for my patients to have that uninterrupted and clear view during the coaching lessons.”
Health care professional participants’ impressions were focused on 2 main themes: food preparation and educational experience.
Food preparation
Health care professional participants praised the detailed instructions that were provided before the workshop to help prepare the food items for the session; however, few stated that more details including pictures could have been helpful: “it would be helpful to give an estimate of the prep time before the class. Photos to show how things should look like after done would help too.”
Educational experience
Health care professional participants appreciated both the learning experience of cooking and asking questions in real time, and the visual learning opportunity that the COWC module provides “Viewing and following was a breeze.” However, a few reported discomforts from the requirement to cook at the faculty pace and from perceived gaps between their and the health coach chef cooking skills. “The demonstration moved along very quickly . . . . As we were cooking at the same time it was a challenge to observe the computer screen and watch the cooking ingredients at times.” Suggestions about how to improve the COWC module included providing more culinary and nutritional information both prior and during the session.
Discussion
This report presents a novel approach for the delivery of live, remote, “hands-on” culinary education to participants at their home. It appears that the delivery of real-time “hands-on” cooking through standard, off-the-shelf devices and software is feasible, brings educational value to participants, and is relevant to clinical practice.
Participants’ positive perception about their learning experience is consistent with several previous publications that described both the educational and nutritional benefits of live “hands-on” culinary education delivered by chefs.7-9 Although these publications questioned the scalability of “hands-on” cooking education delivered in a teaching kitchen in a real-world setting, this study participants were positive about adopting the COWC module to their clinical practice. Telemedicine solutions are already known for improving scalability and reducing costs. In addition, a recent report that described the educational experience from culinary videos identified the advantages of using participant home kitchens (i.e., where real-life home cooking is made) as their learning environment. 17 Further research is needed to evaluate whether the COWC has the potential of combining all these benefits to an impactful nutrition education module.
With the completion of this pilot, a COWC module was implemented in both Spaulding Rehabilitation Hospital and Harvard Medical School CME programs; thus, these telemedicine programs are currently including a combination of live video discussions, culinary videos, and live online cooking with a chef. The perceived challenge of following the provider cooking pace was overcome by providing participants with a more detailed preparation description including images and a prerecorded video to review before class, as well as by decreasing the number of servings that were prepared from each of the recipes. Our future plans include adaptation of the COWC modules to address specific health conditions such as breast cancer and spinal cord injury.
It is our intent to also explore whether the COWC module can be adopted by health care professionals who would like to role model home cooking. Walk With a Doc is an initiative that enables health care professionals to role model exercising through walking with patients. 18 This initiative started in 2005 and expanded to more than 400 chapters worldwide. 19 Although evidence suggests that patients may be more likely to adopt healthy eating behaviors if their health care professionals have a nutritious diet,20-22 a similar effort to role model home cooking is lacking. Although the COWC module was designed to be implemented in remote lifestyle medicine and nutrition interventions, it might also be used by health care professionals to model healthy cooking from their home kitchen. Further research is needed to evaluate whether the COWC is a feasible model for health care professionals to share their own recipes and shopping lists before cooking and to model home cooking to their patients.
The COWC module has potential limitations that might affect viability such as individuals without access and/or skills to use internet-enabled devices. Furthermore, compared with videos, the COWC is a time-consuming module that might affect scalability. Although health care professionals showed high acceptance of the module as participants in a medical education setting, the acceptance of the COWC module by patients is unknown. Therefore, adaptations might be needed while implementing the module to clinical settings. This is a small-scale evaluation with a limited number of questions and response rate of 36% to the open-ended question. Further research is required to determine the ideal group size for a COWC module, what is a beneficial mix of COWC modules and culinary videos that can affect a significant nutritional change and whether a prerecorded COWC session followed by a live discussion can substitute a live COWC module.
Calls to promote culinary education are emerging by both professional and health organizations (e.g., Academy of Nutrition and Dietetics, 23 World Health Organization 24 ). However, leaders in the field report on the high costs of maintaining onsite “hands-on” teaching kitchens. Live video tele-conferencing has been shown to improve accessibility and adherence to treatment and to be effective in improving weight management and reducing health care expenses. 25 Further research is needed to evaluate whether the COWC module can be a sustainable solution to these calls to promote culinary education.
Conclusions
This report presents a feasible module for a “hands-on” telemedicine health-related culinary program. Overall, health care professionals found value in this module, and future studies are needed to determine whether this may be a scalable and sustainable telemedicine model to improve nutrition. We hope that this report will help expanding the use of remote live culinary education for the improvement of home cooking and overall health.
Footnotes
Acknowledgements
We would like to thank Harvard Medical School, Department of Postgraduate Medical Education, for their strong collaboration to expand the culinary coaching model. Further we would like to thank our education team, Jane Barg NBC-HWC and Shirley Garrett NBC-HWC, for their ongoing dedication to home cooking education.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Institutions of R.P., S.P., R.W., and J.K.S. offer culinary coaching training programs as a service.
Author Contributions
RP participated in the design of the Cooking online with a chef module, collection and analysing of data, and drafting the manuscript. AF lead the analyzing of the qualitative data and significantly contributed to the revision of the manuscript. SP significantly contributed to the revision of the manuscript. RW significantly contributed to the revision of the manuscript. JKS significantly contributed to the revision of the manuscript. All authors red and reviewed the final manuscript.