
Abstract
Although childhood “picky eating” or “fussy eating” or “food neophobia” is well established as a subject of research, commentary, and treatment guidelines, there is very little published research exploring the origins and basis of adult food neophobia, much less its treatment. Existing treatment guidelines for picky eating tend to focus on cognitive behavioral interventions. The consequences of picky eating, although not extensively researched, include inadequate nutrition and weight management difficulties—both significant contributors to the worldwide disease burden. Health coaching has a focus on personal choice, reflection on previous successes and current strengths, as well as identification of a personal health vision and achievable goals. As such, it may play a useful role in supporting behavioral change in adult picky eaters. A structured intervention, rooted in health coaching skills and culinary medicine aimed at supporting such change, is proposed.
‘. . . there is a pressing need to pursue treatment options for adults presenting with picky eating.’
Picky eating (also known as fussy eating or food neophobia) is generally understudied in adult populations.1,2 Research in the area is frustrated by lack of clear definition of the term. This therefore frustrates a more complete understanding of the health and disease risk consequences of picky eating. Despite this, picky eating may lead to poor nutrition as well as weight management difficulty. Preliminary evidence suggests that picky eating is frequently present with comorbid diabetes, hypercholesterolemia, hypertriglyceridemia, reflux, and sleep apnea. 3 The scarcity of research in the area is a constraining factor in the development of treatment options for picky eating. In general treatment, guidelines are limited in their scope. 4 Notwithstanding this context, there is a pressing need to pursue treatment options for adults presenting with picky eating. Overweight and obesity, in addition to diet-related noncommunicable diseases form part of the World Health Organization (WHO) definition of malnutrition. 5 Together, these outcomes are a significant component of disease burden for communities, states, and nations. 6 Health coaching, including supported approaches to dietary pattern change and culinary medicine, has been shown to improve outcomes 7 for clients presenting with overweight and obesity. Based on the evidence for its use with these populations, health coaching is proposed as a means to engage patients in supported behavioral change for picky eating.
What Is Picky Eating?
There is a great deal of discussion in the literature concerning “picky eating,” “fussy eating,” and “food neophobia”; yet the current literature can be difficult to parse usefully. This is due to the variability in terminology noted above and the general lack of definitional agreement about what “picky” and “fussy” eating actually are. 4 For simplicity, the term picky eating will be used here. Furthermore, the existing terminology encompasses everything from idiosyncratic eating behavior through to significant clinical disorder. The 2013 Diagnostic and Statistical Manual of Mental Disorders features the new diagnosis “Avoidant/Restrictive Food Intake Disorder” (ARFID). 8 The diagnostic criteria for ARFID require one or more of weight loss, tube or supplement feeding, nutritional deficiency, and psychosocial interference. These are not necessarily observed in people who engage in picky eating. In other words, all those meeting diagnostic criteria for ARFID are likely to be picky eaters, but not all picky eaters have ARFID. Consequently, the existence of such a diagnostic category may not be helpful in understanding the breadth of adult “picky eating”.
From the author’s practice experience, picky eating can take on a number of forms. It may relate to the texture, aroma, flavor, color, spiciness and/or liquidity of food. Anecdotally, picky eating often appears to have familial origins. Particular foods may be associated with unpleasant childhood experiences (eg, being forced to eat boiled brussels sprouts). Over time, this specific dislike may generalize into “green vegetables” or even “all vegetables.” By the time of adulthood, patients often have considerable picky eating experience and considerable anxiety about trying new and different foods. Picky eating may also develop situationally as an adult. For example, the fitting of dentures may leave adults overly cautious about foods previously eaten or new food experiences, for fear of difficulties with their dentures. 9
The current literature is mainly focused on childhood rather than adulthood picky eating. While some links have been made between childhood picky eating and adult picky eating, 10 these are relatively scarce and as a consequence, specific treatment protocols or responses to adult picky eating are not widely established. For example, a recent PubMed search revealed 151 results for the search string “child* AND picky AND eating NOT adult*” but only 14 results for the search “adult* AND picky AND eating NOT child*”. There is no clear picture of prevalence in adults and in general, adult picky eating from ontological, diagnostic and treatment perspectives, is understudied. Treatment options generally appear limited to cognitive behavioral therapy with a licensed psychologist in the case of ARFID, 11 or simply encouraging choice from a variety of foodstuffs.
The Consequences of Picky Eating
Picky eating may sometimes be dismissed in children as being of no great consequence—a quirky feature of personality that is essentially harmless. But is this the case? Poor dietary intake is currently the primary identified risk factor for premature death in the United States. 6 Additionally, 45% of cardiometabolic deaths are related to suboptimal nutrition. 12 Consequently, there is a strong move already to treat diet as a “vital sign” 13 in health care.
Many of the patients I see have come to eat only highly processed food that is bland in color, flavor, and texture—for example, potato crisps and chips, white bread, chicken, sweet biscuits, and ice cream. They can often trace such fussiness about food back to adolescence. There is some evidence to suggest that childhood picky eating is a prequel to adult picky eating. 10 In any event, such a dietary pattern is both “picky” and nutritionally inadequate.
Furthermore, it may be that picky eating generally is associated with greater risk of developing so-called “lifestyle” diseases or noncommunicable chronic disease such as diabetes, hypertension, and hypercholesterolemia among others.2,14
Assessing Picky Eating in Patients
Formal methods for assessing picky eating appear to be relatively recently developed. 15 It is therefore likely that adult picky eating behaviors are not currently being widely recognized and assessed in clinical settings. The fundamental sign of picky eating is resistance to eating a variety of foods and a consumption of a narrow, nutritionally restricted diet. This may be a primary driver of cardiometabolic disease risk, inadequate nutrition, and poor body weight control. Consequently, an assessment and understanding of the extent to which picky eating is present in a patient is a vital precursor to the treatment of these health problems.
Picky eating can be assessed initially either by the use of a questionnaire15,16 combined with interview or simply by interview alone. Making straightforward open inquiry about dietary patterns is the most effective means of accomplishing this. Inquiries could include
What does a typical dinner/breakfast/lunch look like for you?
What do you eat between main meals?
What new foods have you tried this year?
What vegetables do you routinely eat?
Having established that a pattern of picky eating behavior exists, asking additional questions to understand the patient perspective of this is useful. Such questions could include
How long do you recall this pattern being present in your life?
What is your understanding of how this pattern of eating developed?
What have been the benefits/consequences of this pattern of eating for you?
What would it mean for you to broaden the range of foods you eat?
On a scale from 0 to 10, where 10 is the most, how much would you like to see a change in this for yourself?
Note the neutrality of the questions above—judgment is neither overt nor implied. At this point, the practitioner is not aiming to provide “expert” knowledge of the consequences of this pattern of eating. The goal here is to understand more fully the patient experience in order to learn more about the picky eating behavior. Aspects may include whether it is longstanding, has elements of comorbid anxiety, what specific prequelae it may have, how the patient sees it as useful to him to her currently and what consequences may have been experienced as a result of it. Notwithstanding this neutrality, it is also appropriate to engage in a curious examination of the role that picky eating may be currently playing in the person’s health status. An example inquiry may be:
What has been the impact of this eating pattern on your overall health, in your view?
This approach to understanding the prequelae, context, impact, behavioral and social consequences of picky eating provides a strong foundation for the health professional seeking to partner with a patient to support health behavior change. Drawing on this detailed individual information, the health coach can work with the patient as he or she develops a personal vision for health and well-being. Furthermore, the health coach can support the patient to identify strategies and goals to fulfill this vision that are personally meaningful and relevant.
The Potential for Health Coaching to Support Eating Behavior Change
Evidence-based health coaching is the practice of partnering “with clients seeking self-directed, lasting changes, aligned with their values, which promote health and wellness and, thereby, enhance well-being.” 17
The role of health and wellness coaching in chronic disease management and early intervention is increasingly the focus of study 18 and the results point consistently to some key factors to explain its efficacy. One of those key factors is the promotion of autonomy and self-direction in health care—engaging patients in a way that seeks to educate and inform where required—and focusses mainly on the development of enduring supported behavioral change that aligns with the values and lifestyle of the patient.
The use of health coaching strategies in improving diet has already been the focus of some investigation18,19,20; however, there does not appear to be any published work on the use of health coaching strategies for assisting adult patients to modify picky eating behaviors. Additionally, there is scant published research about effective interventions for the consequences of adult picky eating (which themselves are poorly understood beyond nutritional inadequacy and weight management difficulties). Notwithstanding this, health coaching provides a framework for addressing the picky eating behavior itself. The relatively recently established field of culinary medicine 21 and education has begun to provide some insight and direction.
A Proposed Health Coaching Approach to Support Behavior Change in Picky Eaters
Once assessment has occurred and some pattern of picky eating has been established, the practitioner should discuss with the patient referral to a health coach (if unable to provide the health coaching intervention personally). Health coaching uses a supportive relational framework to encourage the development of autonomous choice, strength, confidence, readiness, and motivation to change.22,23 The coaching skills employed in such a framework include the principles of positive psychology and positivity, 24 practices of gratitude, recognition of small steps and small change, appreciative inquiry, 25 mindfulness, “SMART” (specific, measurable, attainable, relevant, and timely) goal setting, 26 and the use of “desire to change” and “confidence to change” scales. 27 When required to manage ambivalence—motivational interviewing and decisional balance interventions may be used. 28 Further research is needed to determine the optimal number of health coaching sessions. 19 There does appear to be a dose-response relationship between number of sessions and health outcomes using a schedule of 4 to 18 sessions dependent on patient need. 19
The coaching intervention may be provided either by a suitably trained primary care physician or trained allied health personnel. In the case of picky eating, it is recommended that coaching focus on 2 aspects of diet and nutrition: the range of foods the patient may be prepared to try and the use of culinary medicine—the skills of preparing and cooking food. Culinary medicine is described elsewhere29,30 and is not specifically detailed here. This systems focused approach on person and environment ensures that the patient as well as the systems in which the patient operates are coached. 31
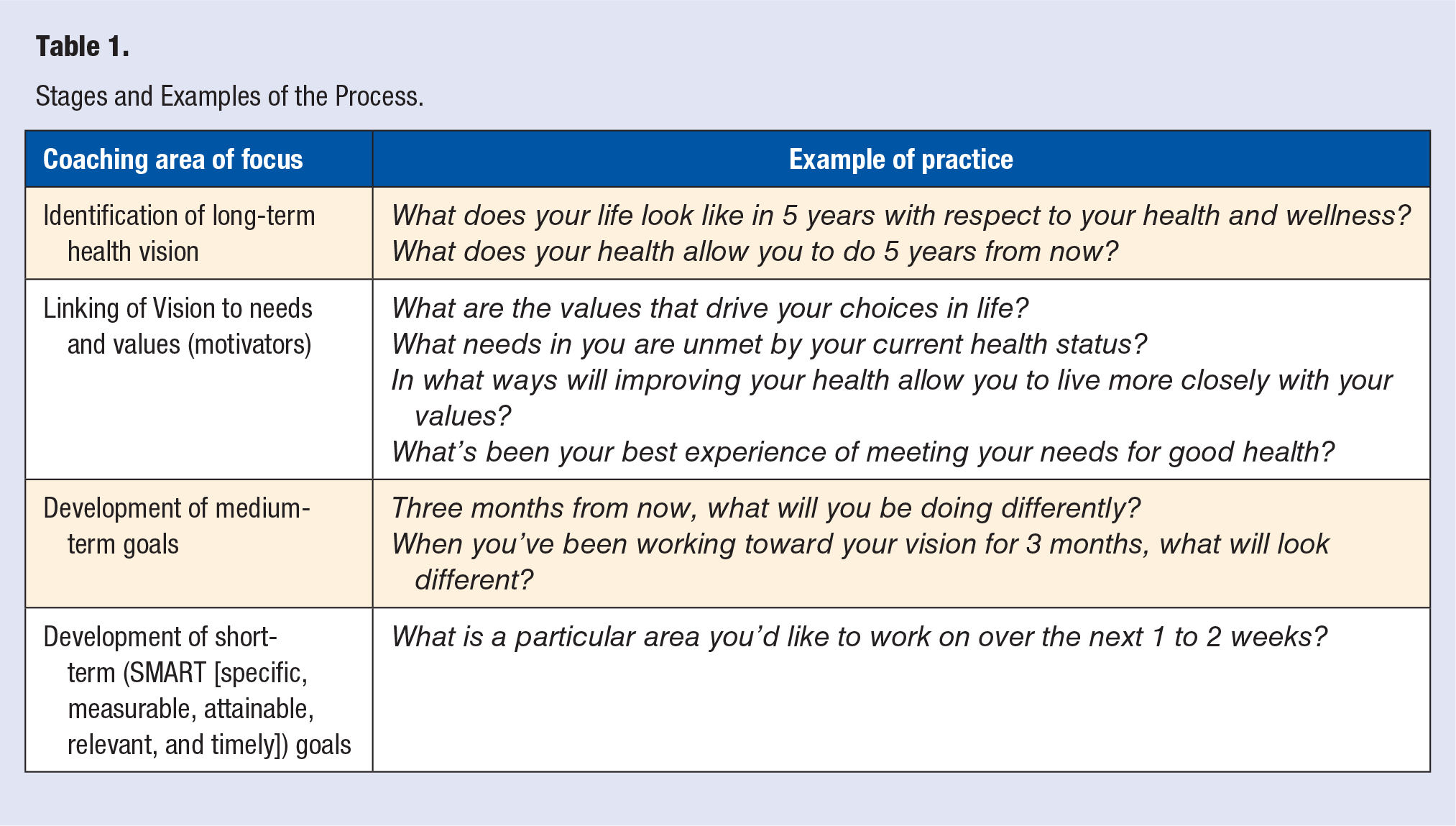
The initial creation of an overarching health and wellness vision 16 is central to the coaching process and gives the patient a clear picture of what to move toward (rather than what to move away from). Questions which can assist in the development of vision include
What does your life look like in 5 years with respect to your health and wellness?
What does your health allow you to do then?
What are the values that drive your choices in life?
What will your strengths and successes be in 5 years?
What will you be able to say about yourself?
Open inquiry and reflection are also used to clarify needs and values. These needs and values, as identified by the patient, become the personalized motivators which they will then draw upon to work toward the desired health behavior change. Medium-term outcome or action goals (approximately 3 months ahead) are identified to form a bridge between the longer-term vision and the formation of shorter-term health behavior change goals. Beyond this, a recursive process of short-term goal identification, planning and progress tracking is employed. It is vital that the goals (in this case eating behavior goals and therefore food preparation/cooking goals) are set by the client, not the coach. It is also imperative that the coach does not find him or herself in the position of suggesting or bargaining with the patient (What if you were to eat leafy greens twice a week?). This leads to a reduction in autonomy, confidence and motivation and impairs the coaching approach. Instead, the identification of specific goals for behavioral change should be patient-initiated and driven.
An overview of how the various stages of the health coaching process might be applied in this context is illustrated in Table 1.
Stages and Examples of the Process.
Conclusion
While currently not well understood or studied, adult picky eating appears to correlate with inadequate nutrition, overweight/obesity, and other chronic noncommunicable diseases. It therefore presents as a lifestyle behavior and a health risk which warrants intervention to support change. Health coaching provided by a trained health and wellness coach is a useful support strategy to assist patients to make behavioral changes to problematic picky eating.
A Recipe
Here is a recipe I developed while coaching one of my postsurgical bariatric patients. She wanted to try some nonmeat sources of protein and wanted to learn how to prepare and cook more nutritious food. She had been a very picky eater prior to this (mostly white bread, mashed potato, and chicken); however, she had come to the point of wanting to be adventurous in trying new foods, recognizing that her prior eating patterns were problematic for her.
This recipe consists of some things that she already enjoyed eating—tomatoes and mushrooms (even though she rarely ate them), and added in eggplant, lentils, and a nutritious leafy brassica—kale. There is a small amount of straightforward cooking (oven roasting and boiling/simmering).
Summer Kale Salad

Ingredients
1 bunch kale
2 whole leeks, white part only
6 whole tomatoes
1 eggplant
200 g button mushrooms
1 cup uncooked French lentils
2 tablespoons pepitas
2 tsp extra virgin olive oil
Juice of 1 lemon
Balsamic vinegar
1 tsp vegetable stock powder
Extra-virgin olive oil spray
For the Dressing
1 tablespoon extra-virgin olive oil
3 tablespoons apple cider vinegar
4 cloves crushed garlic
1 tablespoon maple syrup
1 tablespoon Dijon mustard
Salt, pepper, paprika, and dried oregano to taste
Recipe
The great thing about this recipe is that the various parts can be made ahead of time and kept in the refrigerator—up to 48 hours if you want. A note about the lentils—I use French lentils because they hold their form after cooking much better than red or green lentils.
Rinse the kale well under cold running water—don’t worry about being rough with it. Give it a really good scrub to get rid of dust and dirt. Dry it on paper towel, then tear it off the stems into small pieces—think of pieces that would fit on a tablespoon. Put these in a bowl and drizzle over the 2 tsp olive oil and the lemon juice. Massage this into the leaves for a minute or so—this helps to soften the kale and gives it a lovely tang. The oil simply helps the lemon juice to adhere to the leaves otherwise it would run right off. Set aside till you need it.
Slice the tomatoes in two horizontally. Place in a bowl and lightly spray with olive oil spray (you get a good coating for much less oil this way). Sprinkle with salt, pepper and paprika to taste then toss well so that the halves are well coated. Arrange on a rack in a roasting dish and slow roast at 150 °C for 2 hours or more – you want to get them partially dehydrated but still soft and moist. When done, remove, set aside, and allow to cool.
Dice the eggplant and mushroom and toss in a bowl with paprika, salt and pepper and a little olive oil spray if you like. Tip into a roasting dish. Slice the leeks lengthwise and place in the same lightly oiled roasting dish. Sprinkle liberally with balsamic vinegar and roast in a 220 °C oven for 25 to 30 minutes, turning the eggplant and mushroom once halfway. Cover with foil at this time. Once cooked, slice the leeks crosswise into 1cm lengths and set aside.
Prepare the lentils by adding to 3 cups cold water, adding 1 tsp vegetable stock powder to the water. Bring to the boil for 25 minutes. Remove, drain, and set aside.
Make the dressing by combining all ingredients in a tightly sealed jar and shaking vigorously.
Combine the kale, tomatoes, mushrooms, eggplant, leeks, pepitas, and lentils in a bowl and toss lightly and well (make sure the lentils don’t all end up on the bottom).
Dress, toss lightly again, and serve!
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The author is the CEO of Wellcoaches Australia–School of Health Coaching
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.