
Abstract
Objectives:
This study aimed to explore Hispanic/Latinos’ sociocultural experiences of dealing with chronic diseases as first-generation immigrants.
Methods:
Through purposive sampling, 12 Hispanic/Latino adults with limited English proficiency participated in in-person, semi-structured interviews and provided in-depth insights on lived experiences regarding managing chronic diseases. Interviews were conducted between October 2023 and February 2024 in the Dallas-Fort Worth Metropolitan area, Texas. Interviews were analyzed using the thematic constant comparative method supported by Atlas.ti software to understand participants’ experiences with managing chronic diseases, employing the Sociocultural Health Belief Model as a theoretical lens.
Results:
Participants’ experiences reflected on how sociocultural factors, such as socioculturally-informed health norms and beliefs, cultural adaptation and health literacy, and family influence, contributed to disease management, sometimes as barriers or as resources. Seven themes identified from the responses included: (1) I do not trust the doctor’s treatment and efficacy, so I avoid or delay going to the doctor; (2) I only go to the doctor when I am symptomatic; (3) Structural barriers further complicate cultural health norms and beliefs; (4) I do not know how to change my traditional meals to include healthier food options; (5) Language is a crucial key to healthcare; (6) I rely on Spanish-language health resources, but I have concerns about reliability; and (7) Family is a major source of instrumental emotional and motivational support.
Conclusions:
The findings highlight the interconnectedness of these sociocultural factors and recognize the need for cultural competence in chronic disease management to enhance effective care and improve chronic health outcomes among Hispanic/Latino adults with limited English proficiency.
Keywords
Highlights
Sociocultural factors can hinder or support disease management.
Hispanic/Latino older adults shared barriers and resources within a cultural context.
Findings suggest the need for culturally competent chronic disease management.
Introduction
Of the nearly 20 million foreign-born Hispanic/Latinos in the United States (US) in 2021, 40% are 50 years of age or older, 1 and approximately 54% of immigrants report speaking English proficiently. 2 Immigrants are more likely to suffer from chronic diseases like diabetes, heart disease, arthritis, dementia, and many others compared to native-born individuals. 3 Although these diseases can often be managed by making healthy lifestyle changes, seeking treatment, and adhering to treatment plans, 4 many patients struggle with making long-lasting recommended changes.5,6 For first-generation aging adults, structural and system-level barriers like challenges navigating complex healthcare systems, limited insurance coverage, and financial burdens can make treatment adherence much harder.7-9 Language barriers and limited health literacy further exacerbate these difficulties, contributing to fewer preventative care visits, an increase in emergency room visits, and poorer health status.10-13
In addition to structural obstacles, understanding cultural values and beliefs among Hispanic/Latino older adult immigrants with limited English proficiency (LEP) is essential in patient-centered communication (eg, listening, showing respect, explaining things), an important aspect of care provision that ultimately affects health outcomes.14-17 According to the Sociocultural Health Belief Model (SHBM), 18 cultural values, beliefs, and acculturation can influence chronic disease management through patient-healthcare provider relationships, 19 wherein collectivistic cultures, family involvement, respect for authority figures (including healthcare providers), and shared decision-making can strongly influence the interactions. For example, confianza (trust) plays an integral part in developing meaningful relationships with healthcare providers. This can serve as the foundational element in facilitating communication to discuss symptoms and concerns and increasing patients’ willingness to follow their treatment. 20 Further, the cultural value of familismo (strong family bonds) can play a key role in healthcare processes, either promoting or complicating treatment adherence.21-24 Additionally, other cultural values, like fatalismo and machismo (beliefs reinforcing faith and masculinity), have been documented to influence substance use and reproductive behaviors among Hispanic populations.25-27 Despite vast literature on structural barriers that this demographic group faces, little is known regarding how cultural factors interconnect with structural barriers to shape chronic disease management among Hispanic/Latino older adult immigrants with LEP. 28
In order to inform the development and delivery of culturally competent healthcare, particularly for improving chronic disease management in underserved populations, this study uses the SHBM as a theoretical lens to examine how cultural beliefs and knowledge, along with structural barriers, facilitate or prevent effective chronic disease management among Hispanic/Latino older adult immigrants with LEP. 18 The HBM proposes that patients’ health care decision is made when their perceived benefits outweigh perceived barriers. Building upon the HBM, the SHBM focused more on culturally associated factors. It accounts for cultural norms, values, and beliefs about health and healthcare among patients from diverse cultural backgrounds and explains how these factors affect chronic disease care management. 29 Therefore, the SHBM was selected for this study because it can incorporate and adapt to culturally sensitive contexts while capturing the complexities of healthcare management.30-33
Although previous studies have explored the healthcare challenges experienced by Hispanic/Latino immigrants, their focus has largely remained on identifying immigrants’ structural barriers to care management. Even studies that consider culturally influenced barriers often limit their focus to language, health literacy, and acculturation. Few studies examining the care of Hispanic/Latino older adult immigrants have used qualitative methods to further examine culturally influenced barriers beyond the language, exploring how cultural norms and values shape patients’ perceptions of benefits and barriers to care and, in turn, guide their decisions to pursue chronic management. The findings of this study highlight the importance of examining culturally influenced barriers in conjunction with other barriers to address disparities in real world chronic care management of Hispanic/Latino older adult immigrants with LEP. Overall, the study investigated the following research questions to understand how culture is deeply involved in care management among Hispanic/Latino older adult immigrants with LEP: In what ways do (1) culturally informed health norms and beliefs, (2) cultural adaptation and health literacy, and (3) family influence facilitate or prevent effective chronic disease management among Hispanic/Latino adults with limited English proficiency?
Methods
Study Design and Setting
Guided by the SHBM and past literature, we employed the approach of generic qualitative inquiry18,34,35 to explore how socioculturally-informed health norms and beliefs, cultural adaptation and health literacy, and family influence affect chronic disease management among Hispanic/Latino older adult immigrants with LEP. This approach led to the development of 15 semi-structured open-ended questions as an interview guide. 36 The study was conducted in the Dallas-Fort Worth (DFW) metropolitan area in Texas, which has a high density of Hispanic/Latino individuals, the fastest-growing demographic group in both the area and the state. 37 Approximately one-third of the state speaks a language, mostly Spanish, other than English at home. 38 In Tarrant and Dallas counties, nearly 30% of adults reported not having a routine checkup with a primary care physician. 39 Collectively, these sociodemographic and healthcare access characteristics make the DFW area an appropriate setting to explore unmet needs, barriers, and facilitators to healthcare delivery and health management among Hispanic/Latino older adult immigrants with LEP.
Participant Recruitment and Procedures
Twelve community-dwelling, first-generation Hispanic/Latino adults aged 50 years and older were recruited through purposive sampling between October 2023 and February 2024. These participants were chosen based on their relevance to the research questions, with some insights about experiences of chronic disease management and its barriers and resilience as a Hispanic/Latino older adult immigrant with LEP. Interested participants were initially screened for eligibility. Inclusion criteria included (1) self-identifying as Hispanic/Latino, (2) nativity outside the U.S., (3) having been told by physician they were diagnosed at least 1 chronic disease, (4) being at least 50 years old, and (5) having LEP. All inclusion criteria were self-reported by participants, and LEP was determined through questions regarding participants’ primary language spoken at home, in workplaces, and in interpersonal interactions. Chronic disease was defined broadly as “a condition that lasts more than one year or more and requiring ongoing medical attention, limits activities of daily living, or both.” 40 Interested participants were asked to choose from a list of common chronic diseases, including hypertension, diabetes, cancers, arthritis, and a response option for “other diseases not listed.” Participants were excluded if they did not have a chronic disease diagnosis, had intellectual disabilities, or spoke English fluently at home or in the workplace. Recruitment was conducted through various outreach strategies, including leveraging established community networks, distributing flyers, and in-person contacts at local community organizations. Flyers included study information, including a short study summary, inclusion criteria, compensation, IRB approval, and contact information for study participation. The 2 bilingual researchers (CO & GV) served as the formal gatekeepers by leveraging existing connections with community networks. These connections included working with staff and volunteers from local nonprofit organizations, who provide social and medical services to individuals around DFW, involving them in study development, and identifying eligible participants.
Potential participants were informed that the interviews would explore their experiences with managing chronic diseases as ethnic minorities and first-generation immigrants. Informed consent was obtained from all participants before starting the interview process through written informed consent forms available in English and Spanish. In addition, we provided a verbal explanation of the study purpose, the voluntary nature of participation, and how their information would be protected. Specifically, participants were informed that their responses would be used solely for research purposes, securely stored in password-protected research files, and not shared for any non-research purposes without permission. We also explained that they could skip any question they preferred not to answer and stop the interview at any time. Although no physical risks were anticipated, some interviewees might have experienced mild emotional discomfort when recalling challenging experiences related to their health or immigration. The study was designed to maximize benefits while minimizing harm by providing Hispanic/Latino immigrant populations with a voice to address current gaps in chronic disease, care delivery, and its health equity. All documentation that contained personal health information was handled and managed by the Principal Investigator (PI) and kept in a locked cabinet that only the PI (YK) could access.
Audio recordings, transcripts, screening, and demographic surveys were deidentified, given unique study identifications, and kept in a password-protected server to ensure privacy and protect confidentiality. The study protocol was approved by the University of Texas at Arlington Institutional Review Board (#2023-0409), and no competing financial conflicts of interest exist for researchers.
In-person, semi-structured interviews were conducted individually in Spanish by 2 bilingual researchers (CO & GV) fluent in both English and Spanish, and interviews averaged 60 minutes in length. To ensure confidentiality and privacy, interviews were conducted in a private setting of participants’ choosing. Participants reflected on their chronic disease(s), discussed their chronic disease management strategies, challenges, and the support or resources they relied on. Questions highlighted how sociocultural factors—socioculturally-informed health norms and beliefs, structural and cultural barriers, and family, interpersonal, and community resources—shaped their approach to disease management. Specifically, open-ended questions (Supplemental File 1) covered 3 key domains: (1) chronic disease experiences (e.g., how has your lifestyle, family support, medical care, and cultural beliefs influenced your health status over the years?), (2) chronic disease management journeys (e.g., what challenges have you faced in making lifestyle changes or managing your condition?; how do your cultural traditions, values, or beliefs effect chronic disease management?; what strategies, motivational factors, or social support help you manage your condition more effectively?), (3) knowledge of health disease and management (e.g., how did you first learn about your condition, and has this helped you understand it better?; what challenges have you faced or currently face in learning about your health condition and its management?; how do you find your health information?). While these core domains remained consistent across all interviews, follow-up probes and the sequence of questions evolved naturally based on participants’ responses to allow deeper exploration of emerging themes. The sampling was believed to have reached saturation when enough data samples had been gathered, and recurring themes consistently emerged during the interview. Participants received a gift card as compensation after completion.
Analytic Strategy
The interviews were audio-recorded, then auto-transcribed and manually reviewed for accuracy by 2 bilingual interviewers (CO & GV). Both interviewers compared transcripts with the original recordings to ensure transcript accuracy and data integrity. Any discrepancies were discussed and corrected together before analysis. The interviewers analyzed the transcripts in Spanish using the thematic constant comparative method, 41 a post-positivist approach, to identify key themes. An a priori coding scheme, based on the domains of the SHBM, 18 the research team’s knowledge in health disparities, and the interviewer’s positionality, guided the analysis, as shown in Figure 1. Interview questions and coding scheme were developed by researchers who share Hispanic/Latino immigrant backgrounds. Their shared experiences navigating healthcare as immigrants enriched the analysis by providing deeper insight into cultural beliefs and values, culturally rooted barriers, and multilevel resources relevant to chronic disease management. Two interviewers independently transcribed, read, and coded each transcript line by line in Spanish to generate initial codes. Three researchers (CO, GV, & YK) then met to review and compare the codes for each transcript. During these consensus meetings, the team discussed whether to add, merge, or refine codes, facilitating openness in the development of emerging themes and ensuring consistency. This process, coding one transcript, reviewing it together, and refining the coding scheme, was repeated across all 12 interviews.

The Sociocultural Health Belief Model (SHBM).
After completing these iterative rounds, all transcripts were re-coded independently utilizing the finalized coding scheme on Atlas.ti, aligning with the inductive and iterative process of thematic constant comparative analysis rooted in grounded theory.41,42 Then, the 3 researchers (CO, GV, & YK) conducted additional reviews to ensure that the finalized themes represented participants’ narratives accurately and enhanced the understanding of the findings. These themes began to evolve into detailed stories and provided lived experiences of participants, depth and background, portraying how cultural beliefs factored into their chronic disease management journeys. To ensure consistency, inter-rater reliability (IRR) was calculated between the 2 researchers (IRR score of 0.87), utilizing Cohen’s kappa coefficient, which is automatically calculated in Atlas.ti. 43
For the trustworthiness of the research, this study employed various qualitative research strategies through regular triangulation, debriefings, cross-coding, and record-keeping. 44 Triangulation was used by incorporating various data sources, including interviews and field notes, which provide insight into observation and non-verbal communication cues during the interviews.45,46 In addition, after interviewing 1 or 2 participants, our research team collectively shared insights from the interviews while engaging in reflection. Additionally, after independently coding each interview transcript, the interviewers discussed their findings together to enhance validity and reliability. All decisions and discussions were documented in meeting notes. The interviewers’ Hispanic/Latino cultural backgrounds and community ties enabled them to build rapport and trust with participants and allowed researchers to have a better and deeper understanding and interpretation of the findings.45,46 Further, the Standards for Reporting Qualitative Research (SRQR) reporting checklist was utilized to ensure the transparency and integrity of the qualitative study design (Supplemental File 2).
Results
Descriptive Characteristics of Participants
Twelve first-generation Hispanic/Latino adults were interviewed, as shown in Table 1. Their mean age was 56.7 years (SD = 5.59). The study sample primarily consisted of females, with a quarter of the sample consisting of males (25%). Six participants completed primary education (50%), and 5 completed secondary education (42%). All participants noted that the primary language spoken was Spanish with LEP, and they have all been residing in the U.S. at least for 10 years. A majority of the study sample had been living with hypertension, and half of the sample reported living with more than 1 chronic disease.
Descriptive Characteristics of Study Participants.
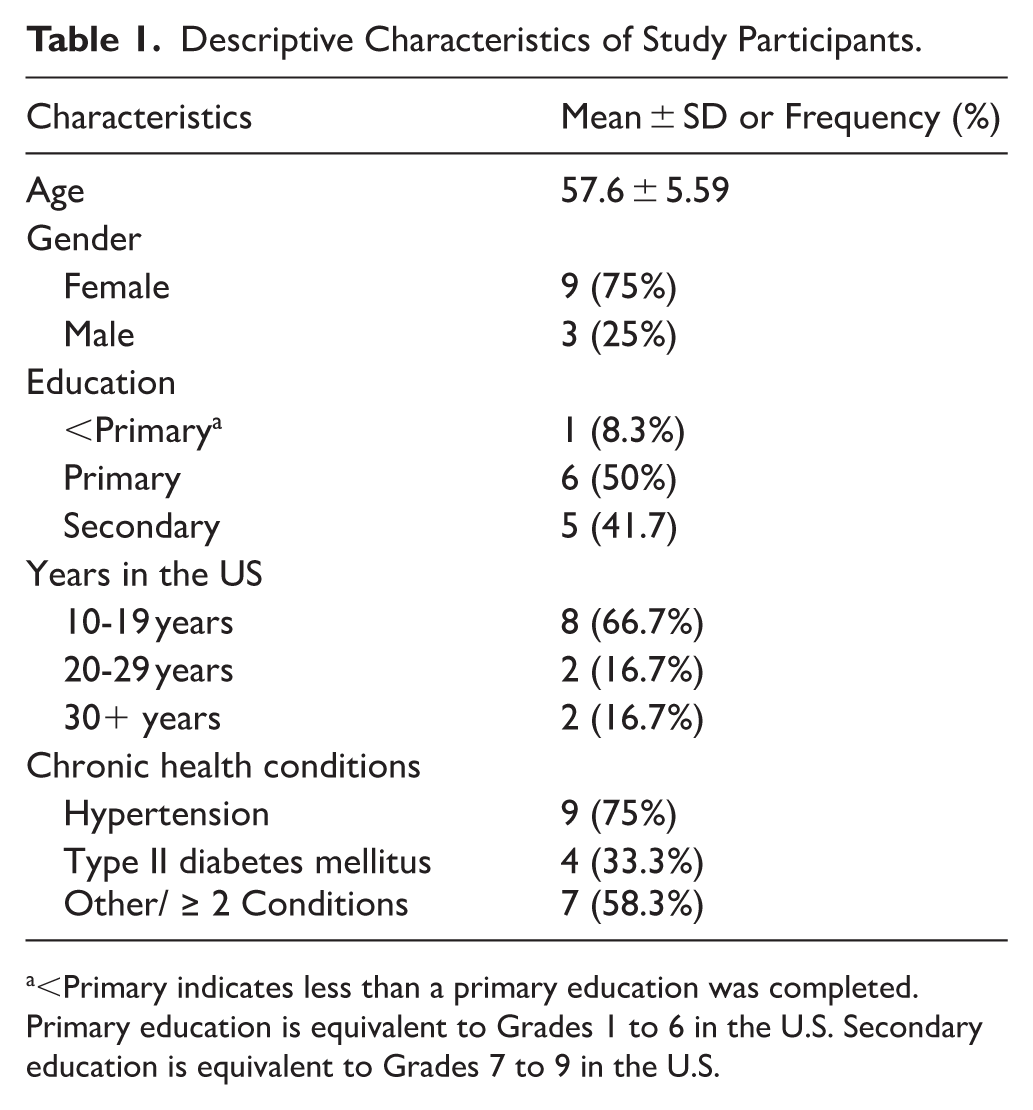
<Primary indicates less than a primary education was completed.
Primary education is equivalent to Grades 1 to 6 in the U.S. Secondary education is equivalent to Grades 7 to 9 in the U.S.
Qualitative Findings
Seven themes were separated into 3 categories representing socioculturally-informed health norms and beliefs, cultural adaptation and health literacy, and family influence (Table 2). Table 2 presents how initial codes were grouped to form themes, along with relevant verbatim evidence such as participant quotes and field notes were interpreted to create final themes. The identified themes were: Category 1- (1) I do not trust the doctor’s treatment and efficacy, so I avoid or delay going to the doctor; (2) I only go to the doctor when I am symptomatic; (3) Structural barriers further complicate cultural health norms and beliefs; Category 2- (4) I do not know how to change my traditional meals to include healthier food options; (5) language is a crucial key to healthcare; (6) I rely on Spanish-language health resources, but I have concerns about reliability; and Category 3- (7) Family is a major source of instrumental emotional and motivational support.
Emerging Themes From Interviewing and Coding.

Category 1: Socioculturally-Informed Health Norms and Beliefs
Theme 1.1 I Do Not Trust the Doctor’s Treatment and Efficacy, So I Avoid or Delay Going to the Doctor
Mistrust in healthcare treatments was found to be a significant barrier to care. Participants frequently shared their uncertainty about the efficacy of medical treatments, making them hesitant to seek healthcare services. One participant (S01) stated, “We never know if they are going to help. Sometimes, they just charge us and give us medication, and if we’re lucky, it works; if not, we just get worse.” Another participant (S02) mentioned, “Being Hispanic, we always wonder why you have to take so much medication. We cannot control ourselves more when we start medicines and stop taking them when we feel better. It’s like sometimes we think that we know more than our doctor, which is not true.” Mistrust in the healthcare system was particularly pronounced among Hispanic/Latino immigrants with LEP. Participants emphasized the importance of trust in building the patient-provider connection, highlighting cultural values such as confianza (trust) and personalismo (importance of personal relationships). When participants felt a lack of trust, they were less likely to seek care and either stop treatment, switch providers, or explore alternative therapies. As one participant (S01) further explained, “I felt discouraged and lost faith in healthcare people. Without faith, we can’t do anything. So, I stopped the care and didn’t know where to go.”
Theme 1.2 I Only Go to the Doctor When I Am Symptomatic
Participants demonstrated a more reactive approach to healthcare by delaying medical visits until they experienced extreme symptoms, hindering preventive care and early chronic disease management. One participant (S14) lived with daily muscle pain for 6 months, hoping it would resolve on its own, and only sought medical attention when the pain became extreme. The participant (S14) described, “There was a moment that I could not deal with the pain anymore. I went to the doctor. . . The doctor told me that they did not know how to put up with that pain for six months without seeing someone with pain this strong.” Many participants relied on self-control or self-management rather than accessing healthcare. This pattern of delayed health-seeking behavior was often linked to a lack of recognition of symptoms as indicators of more serious health conditions. A participant (S05) had daily headaches but did not initially recognize her type II diabetes symptoms. She (S05) noted, “Once they gave me the diabetes medication, my headaches started to go away. After a few days, I realized that the medication was the reason.”
Theme 1.3 Structural Barriers Further Complicate Cultural Health Norms and Beliefs
Participants reported that a combination of socioculturally-informed health beliefs and structural barriers, such as immigration status and financial constraints, significantly affected their ability to manage their health. Immigration status made healthcare access more complex, as some participants reported feelings of exclusion and fear when seeking services. One participant (S17) described, “We struggle more because we are not from this country. . .We do not have the same privileges as those born here.” The feeling of being undervalued or alienated as an immigrant in healthcare systems made it even challenging for participants to actively engage in trustful relationships with providers and access the care they needed. The same participant (S17) continued stating, emphasizing the self-perceived notion they feel as an immigrant navigating the healthcare system. Furthermore, many participants described making difficult choices between paying for healthcare and meeting their family’s financial needs, often prioritizing their family over their own health. Field notes excerpts highlight verbal cues of disappointment, especially in a participant (S11) when he explained the sacrifice his family made to save for the cost of follow-up appointments which was exacerbated due to loss of faith. So, when considering treatment, they feel powerless and frustrated, as if seeking care meant sacrificing their family’s well-being.
Category 2: Cultural Adaptation and Health Literacy
Theme 2.1 I Do Not Know How to Change My Traditional Meals to Include Healthier Food Options
Twelve participants mentioned dietary adaptation as their major challenge in chronic disease management. Participants struggled with modifying their traditional meals to incorporate healthier options. One participant (S05) stated, “I was one of the people that would say that it is impossible to stop eating tortillas.” Cultural identity played a key role in these dietary habits, and social and familial expectations made changes even more difficult. A participant (S02) reflected: “We get out of control sometimes, truthfully. As Hispanics, we know what tamales taste like, beans, carnitas, everything. When you have health conditions, we should be stopping these things to be more controlled.” Social pressures to continue eating traditional foods often led to setbacks in managing chronic diseases. Participant (S11) shared that food plays a vital role in Hispanic/Latino culture, especially during gatherings and holidays, promoting family cohesion, making it harder for them to implement long-term dietary changes. The person (S11) stated that “I try to not drink soda anymore, but you know it always at parties or gatherings that you end up drinking one.” As a result, many participants still struggle to establish healthier eating habits, even after years of managing their chronic diseases.
Theme 2.2 Language is a Crucial Key to Healthcare
Language barriers and limited access to reliable health information further contributed to the underutilization of appropriate care. Some participants shared that their difficulty communicating in English prevented them from forming trusting relationships (confianza) they valued in healthcare interactions, ultimately linking to mistrust and underuse of medicine. For example, one participant (S02) mentioned an instance of decreased confianza in her provider after a language barrier caused miscommunication of her mammogram results, leading her to believe that she may have cancer. She further expressed her confusion and the undue stress this caused her, explaining “a lot of the time, I am left thinking what they [my doctor] told me, or I want to tell them something but can’t,” which can ultimately strain the patient-provider relationship. Other participants had similar stories, including participant (S13) who shared, “First off, there’s a fear to communicate with someone in a different language since you don’t know how to explain your problems in the short amount of time you have with them [the doctor],” which ultimately led to them not understanding the doctor’s treatment plan or taking medications incorrectly.
Theme 2.3 I Rely on Spanish-Language Health Resources, But I Have Concerns About Reliability
Due to their LEP, many participants expressed relying on Spanish-language health resources and educational materials to better understand their conditions. But they also shared concerns about the trustworthiness of these resources, stating “I feel somewhat informed about my condition, but I know I should know more. So, I get on the internet. . . But I don’t know if it [information] is true, it’s difficult to know if what the internet says is true or false, but I still read it.” While online resources in Spanish were helpful, the limited number of reliable resources in Spanish specifically about their symptoms and treatment posed a barrier. Participants expressed hesitation in seeking further information due to doubts about the accuracy of available resources and the complexity of written materials.
Category 3: Family Influence
Theme 3.1 Family is a Major Source of Instrumental, Emotional, and Motivational Support
Participants consistently described their families as a source of motivation and accountability, significantly influencing their adherence to treatment plans. The described family support came in various forms, including encouraging positive behavior changes, reminders to take medication, financial assistance for medical expenses, and accompaniment to doctor’s appointments. One participant (S06) mentioned that “My children take care of me and my spouse. . . . They provide for us, whether its food, medications, living expenses, anything they can.” The fear of experiencing severe health complications, similar to those seen in family members, also acted as a cue to action, and motivated participants to engage in better health management. One participant (S05) explained: “My mother had diabetes too, and I don’t want to get to the point she’s gotten to because of negligence or missing a doctor’s appointment.” Another participant (S01) expressed: “Who is going to take care of me? I’ve seen how difficult it is for my family to care for a sick person who cannot live independently. That is why I am going to take care of myself.” These personal experiences and family dynamics reinforced their commitment to managing their health conditions.
Discussion
This study investigated how sociocultural experiences and barriers intersect to shape chronic disease management patterns among Hispanic/Latino older adult immigrants with LEP. Although prior research has explored healthcare management among Hispanic/Latino immigrants, only a few qualitative studies have focused specifically on those with limited language proficiency. Consistent with past relevant Hispanic/Latino immigrant literature,11,47-52 participants in this study reported not only structural barriers (e.g., financial burden, immigrant status) and language-related challenges (e.g., difficulty communicating with providers) in accessing care, but also their resources (e.g., family) in managing chronic diseases. However, our findings highlight how barriers and resources operate within sociocultural contexts in ways not captured at the surface level, offering a more nuanced, complex, and deeper understanding of the ways culturally constructed values and norms affect the overall health management among Hispanic/Latino older adult immigrants with LEP.
Understanding barriers through the lens of participants’ sociocultural values showed how chronic disease management is embedded in sociocultural contexts—not merely the result of individual behaviors. Participants often indicated that delayed care and non-adherence to treatment plans need to be understood as outcomes shaped by some shared culture within the Hispanic/Latino population. The central value of confianza was described not only as essential for initiating healthcare but also for sustaining follow-up and treatment adherence. Additionally, a reactive approach to healthcare was also evident: initial reaction to symptoms often involved self-management or even endurance, reflecting a cultural philosophy of stoicism that values self-control and resilience. 53 Furthermore, structural barriers (e.g., financial burden) were often interpreted through the value of familismo. Because of the value, participants described prioritizing their family’s needs over their personal health needs, which hindered seeking medical care and engaging in preventive care.54,55
Our study used a sociocultural grounded interpretation of acculturation, an extensively discussed factor in chronic disease management among immigrant populations.56,57 Our findings showed that acculturation operates through deeper cultural values that shape everyday health decisions. For example, making lasting dietary changes was a common challenge for Hispanic/Latino older adult immigrants with LEP. Shifting from traditional diets to medically recommended healthier options was not simply a matter of nutritional knowledge, but one that relates to cultural identity and family cohesion. For example, tortillas, a staple food in Mexican-origin culture, were described as a symbol of tradition and family connection. Moreover, the daily routine of sharing evening meals with family, central to familismo, reinforced the cultural importance of togetherness and personalismo. As a result, participants expressed emotional difficulty, stress, and resistance when attempting to adopt lasting dietary changes that might disrupt these routines. Additionally, language proficiency further complicates chronic disease management. Participants with LEP described difficulties understanding medical information, communicating with providers, and accessing reliable health resources. Some participants with LEP relied on Spanish-language health resources available, but questioned the credibility of the sources, highlighting a need for accessible, evidence-based, culturally relevant health communication.
Secondary findings also highlighted how informal networks act as culturally grounded mechanisms in chronic disease self-management. The role of informal networks—especially family—needs to be understood through the sociocultural value of familismo. While familismo can sometimes discourage patients from seeking healthcare services due to financial obligations,54,55 many times, participants in our study described family as central to their ability to cope with and manage chronic conditions, which is consistent with past literature.21,24 Family members’ roles as health advocates, appointment companions, translators, and emotional supporters are shaped by the deeply held cultural belief that caregiving and mutual support are core family responsibilities. Rather than viewing chronic disease management solely as an individual task, participants often experienced it as a shared family endeavor. In this way, informal networks functioned as culturally meaningful systems of care embedded within the everyday lives of Hispanic/Latino older adult immigrants with LEP.
Limitations
This study has limitations. First, participants were recruited from the Dallas-Fort Worth Metropolitan area in Texas, where the number of Hispanic/Latino immigrants is larger than in other metroplexes. Their experiences may differ from those in metroplexes with a lower percentage of Hispanic/Latino immigrants and in rural areas. Second, the study sample primarily consisted of a relatively small number of first-generation aging adults of Mexican origin, which may not be accurately generalizable to the vast geographical nature of the Hispanic/Latino ethnicity. Third, it is important to note that the interview guide and survey questionnaires were not validated study instruments and were not pilot tested in this population, as they drew more on the experiences of the research team and were guided by the SHBM, which may limit validity. Lastly, because the majority of participants were living with hypertension, the findings may reflect disease management experiences specific to this clinical profile. Experiences of chronic disease management may differ for individuals with other primary conditions. Future research is needed to explore these experiences across different locations, chronic diseases, and include participants from various Hispanic/Latino ethnic groups to provide a broader contextual understanding. A deeper understanding of the cultural nuances surrounding chronic disease management and lifestyle modification may help inform healthcare providers and public health practitioners in developing more culturally responsive approaches. Additionally, we employed a deductive approach guided by the SHBM, which may limit the exploration of themes beyond the model’s framework. Future research may benefit from an inductive approach to identify additional themes.
Conclusion
This qualitative study provided a sociocultural understanding of chronic disease management among Hispanic/Latino older adult immigrants with LEP. By using the constant comparative method in qualitative analysis, this study explored how culture shapes participants’ experience in chronic disease management. The findings underscore the need that healthcare providers to consider cultural values, such as personalismo and confianza, and structural barriers to enhance patients’ timely care. The study also reinforces how cultural adaptation and health literacy influence not just healthcare access but also long-term health behaviors. Given the heterogeneity within the Hispanic/Latino community, more disaggregated studies are warranted to understand how acculturation levels on culture, language, and health literacy shape chronic disease management. Lastly, the study emphasizes the importance of family-centered care, which is paramount for improved individual-level health and healthcare outcomes. Overall, based on the influence of culture on patients’ experiences, cultural competence is highlighted for improving effective chronic disease management.
Practice Implications
The current findings support the pragmatic approach of using the SHBM as a framework for engaging underserved patient populations. 18 When paired with patient-centered communication practices (e.g., listening, showing respect, explaining things, etc.), health practitioners can more closely align themselves as active ally to Hispanic/Latino patients. Given that patient-provider trust was culturally constructed and enacted, this suggests that healthcare providers need to recognize the cultural importance of building relationships with Hispanic/Latino older adult immigrants with LEP —especially through non-verbal communication (e.g., healthcare providers’ tone of voice, facial expression, and degree of eye contact).58,59
Additionally, as noted in the findings, it is important for all providers and care teams (e.g., physicians, nurses, dieticians, counselors, patient navigators) to understand Hispanic/Latino patients’ cultural backgrounds and acknowledge the cultural differences. One of the major barriers that may be out of the control of providers is the ability to speak Spanish.60,61 There are times when non-verbal communication is not enough, meaning that they may have to use a translator; however, providers can still be knowledgeable enough to understand Hispanic/Latino preferences for certain areas, such as diet or medication use, to be able to ask the right questions via the translator. Further, understanding the cultural backgrounds, values, and barriers faced by Hispanic/Latino patients can allow healthcare providers like registered dieticians to develop culturally sensitive and diagnosis specific meal plans. Given that previous literature shows Spanish-language speaking diabetes patients ask fewer questions than their English-language speaking counterparts, healthcare providers should be prepared to elicit questions or provide their patients a list of frequently asked questions as discussion starters. 60 Similarly, healthcare providers can prepare information available in Spanish or be aware of websites that offer vetted Spanish-language content, and healthcare organizations should prioritize developing readable and accurate Spanish language health education materials.
Another aspect of potential best practice would be to ensure that healthcare providers understand strong family obligations, ties, and informal support, and the care team equips patients and their families to positively impact patients’ chronic disease management.62-64 Also, it is important to ensure a trusted family member is available to provide support in the hospital or clinic setting so they do not feel alone in the process and once they return to their home. Lastly, healthcare providers can encourage patients to engage in preventive care, emphasizing that they are not a burden on their family and caregivers can be there for their family longer if they take time to focus on their health in addition to their family caretaking responsibilities.
Supplemental Material
sj-docx-1-his-10.1177_11786329261445200 – Supplemental material for Sociocultural Factors Affecting Chronic Disease Management Among the Hispanic/Latino Ethnic Group in Texas: A Qualitative Study
Supplemental material, sj-docx-1-his-10.1177_11786329261445200 for Sociocultural Factors Affecting Chronic Disease Management Among the Hispanic/Latino Ethnic Group in Texas: A Qualitative Study by Camilla Ortega, Yong Ju Cho, Gabriel Vidal, Grace E. Brannon, Christian E. Vazquez and Yeonwoo Kim in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329261445200 – Supplemental material for Sociocultural Factors Affecting Chronic Disease Management Among the Hispanic/Latino Ethnic Group in Texas: A Qualitative Study
Supplemental material, sj-docx-2-his-10.1177_11786329261445200 for Sociocultural Factors Affecting Chronic Disease Management Among the Hispanic/Latino Ethnic Group in Texas: A Qualitative Study by Camilla Ortega, Yong Ju Cho, Gabriel Vidal, Grace E. Brannon, Christian E. Vazquez and Yeonwoo Kim in Health Services Insights
Supplemental Material
sj-docx-3-his-10.1177_11786329261445200 – Supplemental material for Sociocultural Factors Affecting Chronic Disease Management Among the Hispanic/Latino Ethnic Group in Texas: A Qualitative Study
Supplemental material, sj-docx-3-his-10.1177_11786329261445200 for Sociocultural Factors Affecting Chronic Disease Management Among the Hispanic/Latino Ethnic Group in Texas: A Qualitative Study by Camilla Ortega, Yong Ju Cho, Gabriel Vidal, Grace E. Brannon, Christian E. Vazquez and Yeonwoo Kim in Health Services Insights
Footnotes
Acknowledgements
We would like to thank all the individuals who participated in the projects and provided their insights, lived experiences, and perspectives. We also thank and appreciate the community organizations that assisted in the study.
Ethical Considerations
The study protocol was approved by the University of Texas at Arlington Institutional Review Board (#2023-0409). Participants gave written and verbal consent for review before starting interviews. All study procedures were in alignment with key principles outlined with the Declaration of Helsinki.
Consent to Participate
Written consent was obtained from all participants prior to interviews. In addition, verbal explanations regarding the study objectives and rights were provided to all participants.
Author Contributions
CO and YK were responsible for conceptualization, data collection, analysis/interpretation, manuscript writing, review, and editing. YJC was responsible for manuscript writing, review, and editing. GV was responsible for data collection and analysis. GEB and CEV were responsible for manuscript writing, review, and editing. YK was responsible for supervision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Network on Life Course Health Dynamics and Disparities in 21st Century America (NLCHDD) via grant # R24AG045061 from the National Institute on Aging.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data from the study may be made available on request from the corresponding author. The study data are not publicly available due to ethical and confidentiality reasons.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.