
Abstract
Background:
Shared decision making (SDM) is associated with positive health outcomes and may be particularly relevant for patients with chronic disease.
Objectives:
To investigate whether (1) patients with chronic diseases, particularly those requiring self-management, are more likely to engage in SDM behaviors than patients without chronic diseases and (2) patients with chronic diseases are more likely to have their physicians engage them in SDM.
Design:
A cross-sectional study of patients who were enrolled in a randomized controlled trial to improve patient–physician communication.
Participants:
Adult patients with hypertension at community health clinics in Baltimore, Maryland.
Approach:
We used multivariable regression models to examine the associations of the following predictor variables: (1) chronic disease burden and (2) diseases requiring self-management with the following outcome variables measuring SDM components: (1) patient information sharing, (2) patient decision making, and (3) physician SDM facilitation.
Key Results:
Patients with greater chronic disease burden and more diseases requiring self-management reported more information sharing (β = .07, P = .03 and β = .12, P = .046, respectively) and decision making (β = .06, P = .02 and β = .21, P < .001) as did patients who reported poor general health. Physician facilitation of SDM was not associated with chronic disease burden or with diseases requiring self-management but was associated with higher patient income.
Conclusions:
Patients with chronic diseases, particularly those requiring self-management, may be more likely to engage in SDM behaviors, but physicians may not be more likely to engage such patients in SDM. Targeting patients with chronic disease for SDM may improve health outcomes among the chronically ill, particularly among vulnerable patients (eg, minorities, low-income patients) who suffer disproportionately from such conditions.
Introduction
Current models of chronic disease management have empowered and activated patients at their core 1 –5 and include a recognition of the lifestyle changes, symptom monitoring, and treatment adherence such persons must do as part of their self-management regimens. A central part of patient empowerment involves encouraging patients to participate as equal partners in decisions about the health care they receive. 3,4 That is, patient empowerment in chronic disease management involves both active self-management at home and shared decision making (SDM) within the clinical setting. 5 Shared decision making has been conceptualized with 3 domains: information sharing between patients and physicians, deliberation about the pros and cons of treatment options, and decision making about a treatment plan that is agreed upon by both the patient and the physician. 6,7
Both SDM and patient/provider communication have been associated with chronic disease self-management and positive health outcomes across several illnesses, including diabetes, cardiovascular disease, and asthma. 8 –13 For example, when patients and physicians set diabetes self-care agendas together, patients are more able to make the lifestyle changes needed to manage their diabetes. 8 Similarly, when patients with asthma have shared goals with their health care providers, they are more likely to adhere to medication regimens and have better control of their asthma. 9 Shared decision making is also associated with better control of diabetes and hypertension, higher ratings of self-reported health, shorter hospitalizations, and increased use of preventive care. 11 –13
Thus, there is evidence that SDM is an important and effective part of chronic disease management. Yet several important questions remain. First, it is currently not known whether patients with chronic diseases are more likely to engage in SDM behaviors than patients without chronic disease states. It is possible that patients who are empowered to manage their chronic diseases at home may be more active in clinical encounters and in SDM with their health care providers, particularly because patient activation and self-efficacy are known predictors of patient participation in care. 14,15 However, it is also possible that patients with chronic diseases, in comparison to those without such conditions, are less empowered and less active in managing their health (since a lack of health promoting behaviors may have led to the development of their medical conditions in the first place) and are consequently less active in clinical encounters and in SDM.
Second, it is not currently known whether patients with chronic diseases, particularly with those illnesses requiring self-management, are more likely to have their physicians engage them in SDM than patients without chronic disease. It is plausible that physicians are either more likely to engage such patients (recognizing the important role of SDM in chronic disease outcomes) or less likely to do so (if they have lowered expectations about these patients’ motivation and ability to actively comanage their health). Understanding physician SDM behaviors among different patient populations is important because prioritizing time and resources in outpatient settings is essential to delivering efficient health care.
We used a multiethnic sample of patients to explore these issues between SDM and chronic disease self-management. We hypothesized that having an increased chronic disease burden, and having a chronic disease requiring active self-management, would be positively associated with 2 important patient SDM behaviors—information seeking and decision making. We also hypothesized that having an increased chronic disease burden, and having a chronic disease requiring active self-management, would be positively associated with physician behaviors that facilitate SDM.
Methods
Study Design
This was a cross-sectional study of enrollment visits between patients and physicians who participated in a randomized controlled trial (RCT) evaluating patient–physician communication and patient adherence to recommended treatment for hypertension. Eligible patients included adults, aged 18 and older, diagnosed with hypertension, who received care in 1 of the 15 community health clinics in Baltimore, Maryland, that primarily served African American and low socioeconomic status patients. Eligible physicians included primary care physicians who practiced at a participating site for at least 20 hours/ week and intended to remain at the site for at least 12 months following enrollment. Participating physicians’ panels were used to recruit eligible patients. In all, 50 physicians and 279 patients were recruited into the RCT, and 273 patients completed the baseline questionnaire and were included in this study. The study was approved by the Institutional Review Board of the Johns Hopkins Medical Institutions. Details of the study protocol are described in detail elsewhere. 16
Study Measures
All of the measured variables for this study were obtained from patient surveys (ie, not physician surveys) conducted at the baseline time period of the RCT, from 2005 to 2006.
Outcome variables
Patient and provider SDM behaviors were assessed through the Perception of Involvement in Care Scale (PICS), a self-reported patient questionnaire divided into 3 subscales: doctor facilitation, patient information exchange, and patient decision making. 17 Information sharing and decision making have been identified as 2 key areas of SDM as has provider facilitation of SDM (eg, eliciting preferences for treatment options). 6,7 The PICS has sufficient reliability (Cronbach α: .73) and validity, and its components are associated with patient satisfaction, patient understanding, perceived control, and expected improvement in functional capacity. 17 The PICS has been used to measure constructs of SDM in several disease states, including heart failure and depression, and a modified version has been validated among patients with chronic pain. 18 –20 Responses are close coded in a 5-point Likert-type scale format. Subscale scores are averages of responses to individual items in the scale, with potential range from 1 to 5.
Predictor variables
“Chronic disease burden” was measured as a count of the 15 conditions included in an instrument assessing health status previously cited in the literature. 16 This instrument covers a broad array of clinical conditions, including both physical and mental/psychological disorders, and includes commonly cited medical conditions in clinical practice. 21,22 The 15 chronic diseases included diabetes, asthma/chronic obstructive pulmonary disease (COPD)/chronic lung disease, coronary artery disease (CAD)/angina, heart failure/congestive heart failure (CHF), arthritis, stroke/major paralysis, back problems, irritable bowel syndrome/colitis, thyroid disorder, neurological disorder, cancer, renal failure, eye disease, alcohol/substance abuse, and depression. The variable “chronic diseases requiring self-management” was created as a count of 4 conditions identified as requiring self-management (diabetes, asthma/COPD/chronic lung disease, CAD/angina, and heart failure/CHF). While all diseases require some degree of patient awareness and management (eg, medication adherence), a continuum exists upon which some conditions require more frequent and more comprehensive self-management strategies. We selected these 4 conditions because they are at the “intensive” end of the self-management spectrum and because guidelines exist for patient self-management (eg, asthma action plans, daily weights, self-glucose monitoring), thus underscoring the active role of patients required for management of these conditions. 23 –25 The variable chronic diseases without self-management was defined as a count of the 11 remaining chronic conditions. These 3 predictor variables (chronic disease burden, chronic diseases requiring self-management, and chronic diseases without self-management) were treated as continuous variables in our analysis. We utilized counts of chronic diseases (ie, continuous variables) to allow the examination of the effect of an increasing burden of chronic diseases (vs dichotomous variables). This is particularly important because all research participants had at least 1 chronic disease (hypertension).
Covariates
The variable “How well known by physician” was measured using the physician postvisit survey and was defined based on the physician’s response to the query, “How well do you know this patient?” (With responses ranging from 1 = not at all to 5 = very well). In prior studies, physician familiarity with patients has been associated with patient preferences for SDM roles and physician-reported respect for individual patients. 26 –28 Health literacy was measured by the Rapid Estimate of Adult Literacy in Medicine (REALM), 29 a validated instrument that has been associated with important health outcomes such as glycemic control. 30 Race/ethnicity was assessed by self-report, the generally accepted approach to identifying patient race/ethnicity and one that has been recommended by the Institute of Medicine. 31 Other demographic variables included gender, age, education, and annual household income. Self-reported health status was measured by a single item from the Medical Outcomes Study 36-item Short Form that has been used in diverse patient populations (including diabetes patients) and settings and has been validated to predict mortality. 32,33 Health insurance information was also based on self-report. Cut points for covariates that were categorized were based on their observed frequencies.
Data Analysis
We first conducted descriptive analyses of the patient encounters. We then used multivariable mixed linear and logistic regression to examine separately the associations of the following predictor variables (1) chronic disease burden (count of 15 diseases), (2) diseases requiring self-management (count of 4 diseases: diabetes, asthma/COPD, coronary artery disease, and heart failure), and (3) diseases not requiring self-management (count of 11 diseases) with our outcome variables, which included 3 subscales of the Patient Involvement in Care Scale (1) patient information sharing, (2) patient decision making, and (3) physician facilitation of SDM. Physician facilitation of SDM was dichotomized at the median for analysis because it was markedly skewed (with higher values predominating) and thus, linear models (which require normally distributed data) could not be used. For this reason, we utilized logistic regression models (ie, binary/dichotomous outcome variables) for the physician facilitation data, which are able to effectively handle skewed data. We adjusted for sociodemographic variables (ie, race, gender, education, and income), health-related variables (ie, health insurance status, self-reported health status, and health literacy), and a patient/provider relationship variable (ie, how well the physician knows the patient). Physician was included as a random effect in all models to account for clustering of patients within physicians. We used STATA 9.0 (STATA Corp, College Station, Texas) for all analyses and defined statistical significance as P < .05.
Results
Two-thirds (66.1%) of the patients were women, and the mean age was 58.3 years (Table 1). Approximately one-third (36.9%) of the patients were African American and two-thirds (63.1%) were non-Hispanic white. Approximately three-quarters (72.9%) of the patients had a high school degree or less. One-quarter (25.6%) of the patients were insured by Medicaid (either alone or in combination with Medicare). Three-quarters (75.7%) of the patients had 2 or more chronic conditions. Means (standard deviation) of the outcome variables of patient information sharing, SDM, and doctor facilitation of SDM were 3.73 (0.74), 2.65 (0.67), and 3.82 (0.87), respectively, on a scale from 1 to 5.
Baseline Sample Characteristics.a

Abbreviation: SD, standard deviation.
a n = 273.
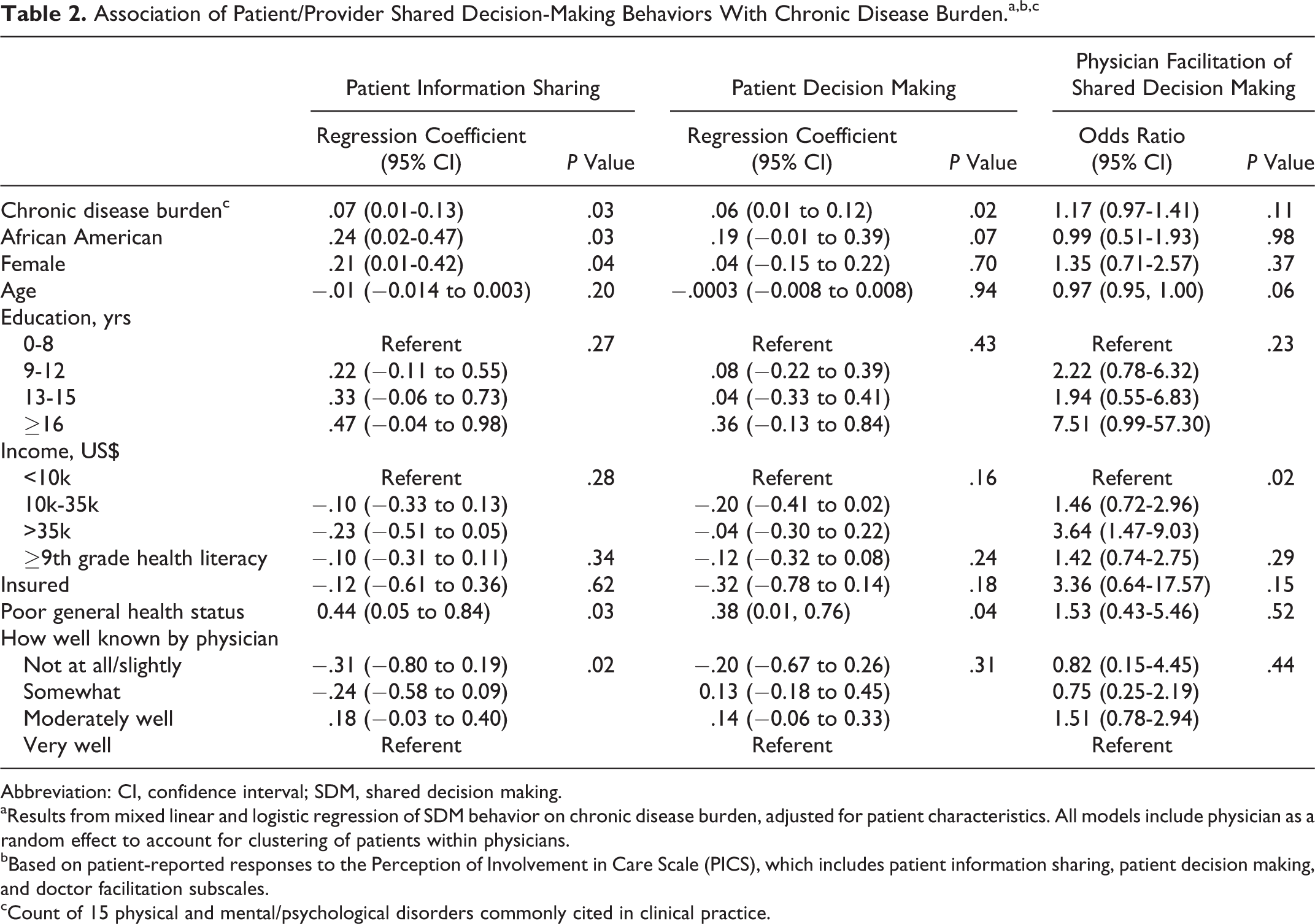
Patients with greater chronic disease burdens and diseases requiring self-management report sharing more information (β = .07, P = .03 and β = .12, P = .046, respectively) and engaging in more decision making (β = .06, P = .02 and β = .21, P < .001, respectively) with their physicians, in both adjusted (Tables 2 and 3) and unadjusted analyses (data not shown). Having diseases that did not require self-management had no correlation with reported information sharing or decision making among patients (data not shown). None of the chronic disease measures were associated with physician facilitation of SDM.
Association of Patient/Provider Shared Decision-Making Behaviors With Chronic Disease Burden.a,b,c
Abbreviation: CI, confidence interval; SDM, shared decision making.
aResults from mixed linear and logistic regression of SDM behavior on chronic disease burden, adjusted for patient characteristics. All models include physician as a random effect to account for clustering of patients within physicians.
bBased on patient-reported responses to the Perception of Involvement in Care Scale (PICS), which includes patient information sharing, patient decision making, and doctor facilitation subscales.
cCount of 15 physical and mental/psychological disorders commonly cited in clinical practice.
Association of Patient/Provider Shared Decision-Making Behaviors With Burden of Chronic Diseases Requiring Self-Care.a,b,c

Abbreviation: CAD, coronary artery disease; CHF, congestive heart failure; CI, confidence interval; COPD, chronic obstructive pulmonary disease; SDM, shared decision making.
bBased on patient-reported responses to the Perception of Involvement in Care Scale (PICS), which includes patient information sharing, patient decision making and doctor facilitation subscales.
cCount (0-5) of the following 4 conditions: diabetes, asthma/COPD/chronic lung disease, CAD/angina, and heart failure/CHF.
Persons with poor health status were more likely to report sharing information and engaging in more decision making with their physicians than those in better health, but physicians were not significantly more likely to facilitate SDM among those who were in poor health. African Americans and women reported sharing more information with their physicians (in comparison to non-Hispanic whites and men, respectively), with adjustment for chronic disease burden, but these associations were not significant with adjustment for self-management disease burden.
The only patient variable associated with physician facilitation of SDM was income. Persons with the highest income (≥US$35 000 annual household income) had more than 3 times the odds of having their physicians engage them in SDM (Tables 2 and 3).
Discussion
We found that patients with greater chronic disease burdens and diseases requiring self-management were more likely to report engaging in SDM behaviors than patients without chronic diseases or with diseases not requiring self-management. Our study suggests that patients whose diseases require self-care at home are more active with their physicians during clinical encounters. Although the reasons for these associations are not clear, patient knowledge and self-efficacy may mediate these relationships. 34 –40 That is, patients who manage their diseases at home may be more knowledgeable about their conditions and feel more confident in making clinical decisions about their care. These patients may, in turn, be able to translate these skills into clinical settings when interacting with their physicians. This is important because even when patients want to have an active role in decision making, they may find it challenging to do so. 41 Thus, identifying ways to empower patients during clinical encounters is an important area of research.
Our study suggests that women may be more likely to engage in information sharing with their physicians than men, a finding that is consistent with prior studies about SDM preferences and behaviors. 11 Our study also suggests that African Americans may be more likely to share information with their doctors than whites. There has been relatively little work regarding racial differences in SDM behaviors among patients, 26,42,43 but in a study of diabetic patients receiving care at community health centers, Peek et al found that African Americans had nearly twice the odds of reporting initiating discussions with their physicians about diabetes care. 26 In a study of patients with hypertension, Cené et al reported that African Americans had similar rates of partnership-building conversations with their physicians as their white peers. 43 Thus, our current study adds to the literature that suggests that patient preferences and/or patient behaviors may not be the causes of previously documented racial differences in SDM. 26,42,44 However, our findings contrast those of Johnson et al who found that African Americans were less verbally engaged with their doctors than non-Hispanic whites. 42 More work is needed to clarify the role that race plays in determining patients’ SDM behaviors.
In contrast to patient behaviors, physician SDM behaviors were not associated with the chronic disease status of their patients. Our study suggests that physicians may not be tailoring their behaviors to match those of their patients, at least among patients with chronic diseases. Physician behavior was, however, associated with patients’ income; higher income patients had approximately 3 times the odds of reporting that their physicians engaged them in SDM. These findings are consistent with prior work demonstrating that physicians are unable to accurately predict which patients prefer more information sharing and SDM, 45 –47 even when, as in the case of our study, some patients’ behaviors clearly express a preference for decision-making style. Physicians may use “substitute judgments” about patient preferences for information sharing and SDM rather than asking patients directly, 45 and these judgments may be shaped by sociodemographic factors such as income. In a study by Waitzkin et al, physicians were more likely to underestimate the preferences for information sharing among patients with lower incomes and/or less education. 46
Our study has several limitations. First, we measured patient and physician behaviors based on patient self-report, which may have impacted the accuracy of these measures. However, several studies suggest that patients may be able to accurately assess the quality of patient/provider communication. For example, in one study of patient/physician communication, researchers found similar assessments between audiotaped encounters (analyzed by a blinded research team) and patient surveys about physician communication during the encounter. 48 Similarly, Beach et al found that patients were able to perceive when physicians had less respect for them and gave them less information. 27 A second limitation to our study is that our data are cross-sectional in nature, and causal relationships cannot be inferred from our study. Third, we were not able to control for all potential confounders in the patient–provider relationship that affect SDM. Finally, our data were collected from a geographically limited sample, and, thus, our findings may not be generalized to patients in other regions of the United States.
Nonetheless, our study has several strengths. First, it includes patients’ reports on their own activation behaviors and their physician’s facilitative communication behaviors within the same clinical encounter, which allows a simultaneous evaluation of both partners in the SDM process. Second, we were able to adjust for several important sociodemographic factors and patient/provider relationship measures that may affect patient and physician behaviors related to SDM. Third, our study focuses on the clinical experiences of an urban, disproportionately minority, and chronically ill patient population receiving care in traditionally underserved clinical settings. This population is generally understudied yet is often most at risk for poor health outcomes.
In summary, we found that patients with chronic diseases, particularly those that require self-management, were more likely to report engaging in SDM behaviors (ie, information sharing and decision making). Yet, physicians were not more likely to engage such patients in the SDM process. Our findings also suggest that African Americans and women may be more likely to engage their physicians in SDM, while physicians may be more likely to engage persons with higher incomes. Although SDM is an important goal for all patients, regardless of socioeconomic status or disease status, targeting patients with chronic disease for SDM may be one strategy to improve health outcomes among the chronically ill, especially those in poor health. This may be particularly relevant for vulnerable patients with chronic diseases (eg, racial/ethnic minorities, low-income patients) who suffer disproportionately from such conditions and may be less likely to have their physicians engage them in SDM than other populations. 39,42,49,50
Footnotes
Author’s Notes
An abstract of this work was presented at the American Academy on Communication in Healthcare National Conference in October 2010.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Heart, Lung, and Blood Institute (R01HL69403) and the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) Chicago Center for Diabetes Translation Research (P30 DK092949) and Diabetes Research and Training Center (P60 DK20595). Dr Peek was supported by the Robert Wood Johnson Foundation (RWJF), Harold Amos Medical Faculty Development program and the Mentored Patient-Oriented Career Development Award of the National Institute of Diabetes and Digestive and Kidney Diseases (K23 DK075006). Dr Cooper was supported by a grant from the National Heart, Lung, and Blood Institute (K24HL083113).