
Abstract
Background:
The introduction of the International Classification of Diseases 10th Revision (ICD-10) code Z71.81 in 2015 enabled the systematic documentation of spiritual and religious counseling (SRC) in hospital settings, opening avenues for research into its effect on patient outcomes and healthcare resource utilization. Religion and spirituality are integral to many patients’ lives, influencing their well-being, recovery and health outcomes. Despite its potential to improve outcomes, limited data exist on SRC’s application and effect in the hospital setting.
Objectives:
This study evaluated the frequency and characteristics of SRC documentation and explored its associations with patient outcome in the inpatient hospital setting.
Design:
A retrospective observational study.
Methods:
Data were drawn from the Healthcare Cost and Utilization Project’s Nationwide Inpatient Sample from 2016 to 2021, encompassing all United States hospitalizations excluding military and specialty facilities. This dataset provided a nationally representative sample of all hospitalizations. Inpatient visits coded for SRC were identified using ICD-10 Z71.81. Statistical analyses assessed descriptive trends and associations with outcomes such as mortality, length of stay (LOS), and healthcare charges.
Results:
The analysis included 5910 SRC-documented inpatient visits from 89 hospitals. SRC was frequently documented for patients with severe or terminal conditions, as evidenced by a significantly higher mortality rate (10.9% vs 2.3% overall). Temporal trends demonstrated a steady, albeit modest, increase in SRC documentation over the study period. While SRC utilization varied across demographic groups, differences in access and outcomes were evident.
Conclusion:
SRC is primarily utilized in complex, high-mortality cases, underscoring its role in holistic care for severely ill patients. The disparities observed highlight the need for standardized SRC documentation and equitable access to SRC. Future research should investigate the clinical and economic impacts of SRC to enhance patient-centered care in alignment with value-based care practices.
Keywords
Introduction
The use of International Classification of Diseases 10th Revision (ICD-10) codes allows for streamlined and accurate data collection of the reasons associated with a patient hospital visit and the subsequent provision of care.1,2 These codes are used nationwide and allow for the description and comparison of outcomes in a real-world setting. In the transition from a fee-for-service model to a value-based care model the ability to assess the outcomes associated with healthcare interventions is imperative.
In October of 2015, the ICD-10 code Z71.81 was established for documenting spiritual and religious counseling (SRC) in the hospital inpatient setting. It is now possible to describe the provision of SRC and assess the effectiveness of SRC. The use of ICD-10 codes allows for the assessment of outcomes-oriented chaplaincy between hospitals. 3 Improved patient outcomes and satisfaction are at the heart of the transition to value-based care models. By promoting preventative care and holistic disease management, these value-based models aim to improve patient outcomes, patient experience, and reduce overall healthcare costs. 4
Religion and spirituality play a substantial role in the lives of many patients, influencing their beliefs, coping mechanisms, and overall well-being.5 -7 It is not a surprise then that SRC is associated with positive health outcomes in the hospital setting. Several studies, including meta-analyses, have shown that incorporating SRC into patient treatment plans improves quality of life (QOL), enhances coping mechanisms, and may reduce length of stay (LOS).8 -13 Engaging in spiritual and religious practices has been associated with lower levels of inflammation, improved cardiovascular health, and even increased longevity.12,14
Chaplains and other spiritual care providers facilitate communication between patients, families, and healthcare providers, contributing to more comprehensive and compassionate care plans. 15 This collaboration promotes a sense of comfort, support, and guidance that enhances the overall patient experience. 16 Patients receiving SRC are more likely to rate their care at the highest level. 17 In turn, patients whose spiritual or religious needs are adequately met are more likely to choose the same hospital again and recommend the hospital to family and friends. 16
The provision of SRC promote holistic health by addressing the mental and emotional well-being of patients. 18 It is a critical part of achieving the Triple Aim - (1) improve patient experience, (2) improve population health, and (3) reduce the per capita cost of care - of value-based care models. 19 Additionally, SRC helps patients navigate the existential dilemmas often accompanying severe illness. 20 By addressing these aspects of patient care, providers enhance outcomes and satisfaction, aligning with the objectives of value-based care models. However, while there are many studies examining the role of spiritual care in the hospital setting, none have used an administrative claims data to assess the role of SRC with respect to health outcomes and utilization.
This study aimed to describe the use of SRC in the inpatient setting from 2016 through 2021. The objectives of this research study were to understand the frequency of SRC documentation in the hospital claims data and generate hypotheses for future research of the effectiveness of SRC in the inpatient setting.
Methods
Data
Data were obtained from the 2016 to 2021 Agency for Healthcare Quality and Research (AHRQ) Healthcare Cost and Utilization Project (HCUP) Nationwide Inpatient Sample (NIS). 21 The HCUP NIS is the most comprehensive source of all-payer hospitalizations from United States (US) hospitals (excluding military, Veteran’s Affairs, rehabilitation, and long-term acute care hospitals). 21 States participating in HCUP cover more than 97% of the US population. The NIS contains approximately 20% of all community hospital discharges and can be generalized to represent all US hospitalizations using provided discharge weights. Depending on the year, the HCUP NIS has between 30 and 40 variables to capture all diagnoses and procedure codes for each patient visit. AHRQ data is publicly available and complies with the Health Insurance Portability and Accountability Act (HIPAA) by removing state, hospital, and restricting patient identifiers.
Statistical Analysis
All patient visits with an ICD-10 diagnosis code of Z71.81 were included in the analysis. Data measured on a continuous scale was summarized by way of mean, standard deviation, median, and inter-quartile range (IQR). Categorical data were summarized with counts and percentages. Time data were summarized using counts and rates reported over-time as compound annual growth rate (CAGR). All data were weighted using the provided weights to produce nationally representative results. The following outcome variables were analyzed using univariate statistical tests: length of stay (LOS), total visit charges, and mortality. The outcomes were assessed by Age (under 65 or 65 years and older), Sex (male or female), and Race (White or Non-White). The Mann-Whitney U test was used to assess differences between groups for LOS and total charges due to the data being non-normally distributed based on assessment of the skewness and kurtosis measures. The Chi-square test was used to assess differences in mortality between the groups. A stepwise logistic regression analysis was used to evaluate the odds ratios (OR) of SRC patient demographics on mortality. All analyses and graphical presentations were performed using SPSS software, version 28 (IBM, Armonk, NY). A P value < .05 was considered statistically significant. This study used HCUP NIS database which is a publicly available non-identifiable secondary data source and additional informed consent was not required. The study was reviewed and determined by the Xavier University Institutional Review Board (IRB) to be exempt from IRB review (IRB Waiver 20240307135527).
Results
The provision of SRC occurred in 5910 inpatient visits across 89 hospitals from 2016 to 2021 (Figure 1). The number of patient visits with SRC increased from 150 to a peak of 1535 in 2018. In 2020, the number of visits declined to 920 due likely to the COVID-19 pandemic and increased to 1250 in 2021. The 2016-2021 compound annual growth rate (CAGR) was 71%. The total number of all inpatient visits ranged from 35.7 million to 33.3 million during this period (CAGR −1.7%). SRC visits represented less than 0.01% of all hospital visits from 2016 to 2021. The number of hospitals documenting SRC increased from 5 in 2016 to 22 in 2021. Similar to the number of patient visits, there was a decrease in hospitals reporting SRC from 2019 to 2020.
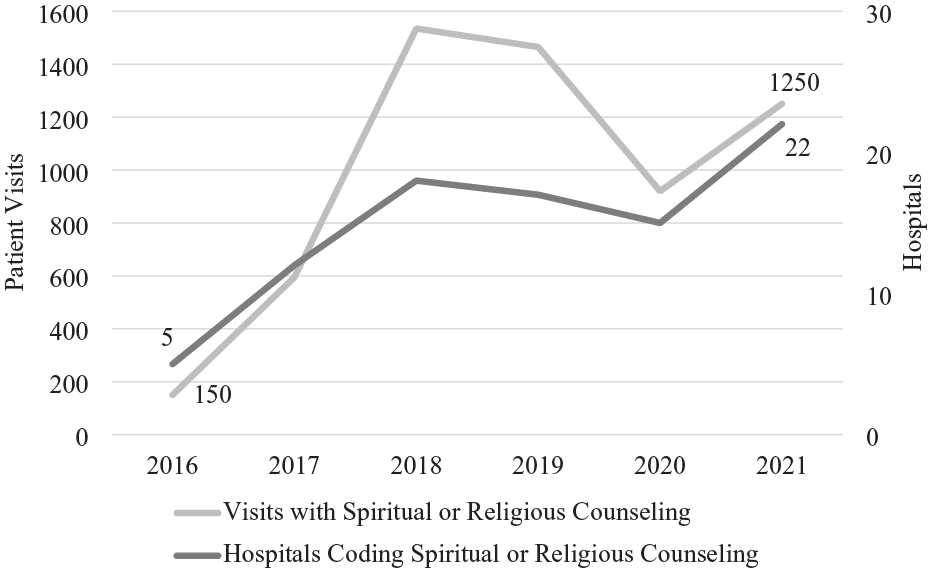
Patient visits and hospitals documenting spiritual and religious counseling.
The patient visit characteristics are in Table 1. The median age of the patients receiving SRC was 62 (interquartile range (IQR): 40-75) and 50% were female. There were 610 (10%) patients who arrived for an elective visit and 3050 (52%) arrived through the emergency department. The majority (5910; 85%) of the patients receiving SRC were White. Medicare was the primary payer for 51% (3000) of the visits followed by private insurance 19% (1120) and Medicaid 17% (1000). Patients receiving SRC were more likely to live in low-income areas based on the median household income of their zip-code. The median length of stay was 5 days (IQR: 3-8) and the median hospital charges were $49 367 (IQR: $23 384 to $101 389). Patients were most likely to be discharged home, 48%, and 11% (645) of the patients died during the hospitalization.
Patient Visit Characteristics.

The hospital characteristics of patients receiving SRC are located in Table 1. The majority (4920; 83%) of visits occurred in hospitals in the South, in Urban/Teaching hospitals 85%, and hospitals with a large number of beds, 60%. The overwhelming majority, 99%, of patient visits receiving SRC occurred in non-profit hospitals.
Patients receiving SRC during their hospitalization had a wide variety of Diagnosis Related Group (DRG), primary ICD-10 diagnoses, and primary ICD-10 procedure codes (Table 2). DRG 885, psychoses, was the most frequent DRG with 350 (6%) visits including SRC. Sepsis, A419, was the most frequent primary diagnosis with 310 (5%) visits. The most frequent primary procedure was group psychotherapy with 140 (2%) visits. Evidenced by these low numbers, the vast majority of patients’ DRGs, primary diagnoses, and primary procedures consisted of other reasons for their visit.
Visit Diagnosis Related Group, Primary Diagnosis, and Primary Procedure Codes.

Abbreviations: MCC, major complications and comorbidities; MV, mechanical ventilation.
Mortality was compared between those receiving SRC and all patient visits. The overall mortality rate for all patient visits was 2.3%. The mortality rate for those receiving SRC was significantly higher at 10.9% (P value < .001) for the same period (Figure 2). Further examination of outcomes by sex, age, and race were completed (Table 3). Males receiving SRC had a higher total hospital charge ($90 677 vs $72 787; P value < .001) and were less likely to die during the visit (10% vs 12%; P value < .028). Patients 65 and older receiving SRC were more likely to die (16% vs 7%; p value < .001) compared to those under 65 years of age. Non-white patients receiving SRC had a longer LOS (9.04 vs 6.26 days; P value < .035), higher total charges ($109 554 vs $76 979; P value < .004), and lower mortality rate (7% vs 11%; P value < .001) compared to white patients.

Mortality during visit between 2016 and 2021.
Comparisons by Sex, Age, and Race.

The differences in mortality observed in the univariate analysis were examined further with a logistic regression model (Table 4). The differences based on sex were not significant (OR 1.156; P value .098) when controlling for patient demographics, elective visits, and hospital location. Patients who were under 65 (OR 2.442; P value < .001) and non-white (OR 1.661; P value .002) where more likely to have died during the visit.
Logistic Regression Results.

Dependent variable was died during visit.
Discussion
This study represents the first comprehensive analysis of SRC in US hospital inpatient settings using claims data. SRC was documented in 5910 inpatient visits between 2016 and 2021 which accounted for less than 0.01% of all inpatient visits. Approximately 2%, 89, of community hospitals reported the use of SRC during this period. The findings suggest that the documentation of SRC via the ICD-10 diagnosis code Z71.81 is grossly underreported.
Estimates suggest that 86% of hospitals have one or more chaplains on staff, and there are more than 10 000 total chaplains in the US.22,23 The likely barriers to reporting SRC include lack of awareness of the ICD-10 code, no financial payment from documenting the code, and confusion of who is allowed to document SRC.24,25 Specific to chaplaincy, there are concerns about patient privacy, lack of consensus on a documentation model, and historical precedence that the demarcation between a clinical provider and a chaplain was clinical documentation. 26
Despite the assumed under-documentation of SRC, several findings stand out. First, SRC was associated with a significantly higher mortality rate among patients receiving SRC (10.9%) compared to the overall inpatient mortality rate (2.3%). This discrepancy is likely attributed to the nature of the conditions leading to SRC documentation, which often involve severe or terminal illnesses. For instance, psychoses and sepsis were among the most frequent diagnoses associated with SRC, both of which are conditions with high morbidity and mortality rates. Second, mortality among non-white patients was significantly lower. However, when comparing patient demographics together through a logistic regression, this finding was reserved, and non-white patients were more likely to have died. Also, we see a similar switch between the univariate analysis of age compared to the multivariate analysis. Patients who were younger were more likely to have died based upon the regression analysis. These findings indicate the need for further research with larger data sets to assess the role of patient demographics on mortality for those receiving SRC. Finally, the vast majority (83%) of patients visits with SRC occurred in hospitals located in the South, consistent with prior research. 27
The ability to demonstrate SRC’s role in achieving the Triple Aim is contingent upon its documentation in the electronic management record. If SRC was documented in the same manner as clinical notes or social worker notes, the benefits can be quantified in a manner that will allow for its effectiveness to be assessed. This effort may allow healthcare systems to better address the holistic needs of the patients and be compensated for the expenses of pursuing value-based care models. Our results do not differ from other research regarding the use Z-codes, which has shown slow uptake by health systems since their inception in 2015.28,29 The authors recognize that the increasing the documentation of SRC presents a “Catch-22.” To receive resources to document the provision of SRC, the work must be completed. If the work is completed under the existing framework, then the resources must be adequate already.
The findings of this research have identified several areas for future research using the ICD-10 code Z71.81. First, research should explore the barriers to accurate documentation of SRC and investigate strategies to improve the utilization of the ICD-10. Second, the exploration of differences in outcomes between those receiving SRC and those that did not can be explored. Third, more research is necessary to understand if the apparent disparities across demographic groups are causally related to SRC. Proper care shall be necessary to minimize selection bias and prevent over generalization of any results using claims data. Finally, understanding the role of SRC in different demographic groups and its impact on health disparities should also be a priority, ensuring that all patients have equitable access to these essential services.
Limitations
Our research was observational in nature and relied on the documentation of an ICD-10 code. As noted, we believe that the capture of Z71.81 was substantially underreported in the claims data. This may be due in part to the code not contributing to the payment for the claim or those providing SRC chose not to document it in the patient’s electronic records. Due to the underreporting, we caution against any generalizations across demographic groups discussed in this study. Rather, we see these results as hypothesis generating for additional research. Second, we were limited by only what was observed and reported in the claims data. The use of Z71.81 does not provide any information on the length of counseling or specifics related to the counseling (ie, assessment, or type of intervention). There is a Current Procedural Terminology (CPT®) procedure code for SRC. However, it is limited to use in Veteran’s Affairs facilities. If this CPT code could be used in a community hospital setting, the HCUP NIS does not provide them. This study relied on all patients available in the HCUP NIS database who met the inclusion and exclusion criteria. Therefore, a power analysis was not performed for this observational study. Despite these limitations, the use of claims data is the foundation of value-based payment between insurers and providers. To understand the benefit of SRC, the use of standardized codes is necessary to assess its role in achieving the Triple Aim.
Conclusion
The integration of SRC into patient care aligns with the objectives of value-based care models, which emphasize a holistic and patient-centered approach to improve outcomes and patient experience, as well as reduce costs. The documented benefits of SRC, including enhanced patient satisfaction, improved quality of life, and better coping mechanisms, support its inclusion in comprehensive care plans. However, since its inception, SRC appears to be underreported, which creates a barrier to fully understanding its effectiveness in patient care.