
Abstract
Background
As the global population ages (United Nations [UN], 2019), the gap in health outcomes between older adult men and women continues to grow (Gahagan et al., 2015; Wallace, 2014). Older women are more likely to be widowed, live alone, experience greater caregiver burden, have fewer financial resources and are less likely to receive informal care compared to older men, which may lead to inequities in health (Katz et al., 2000). These inequities are rooted in historical and structural inequalities between men and women and have a definite impact on health (Jayachandran, 2015; Sen & Östlin, 2008). For example, older men and women use healthcare services differently (Bertakis et al., 2000; Kastor & Shrestha, 2018; Vaidya et al., 2012), particularly in the way they seek and receive treatment (Suominen-Taipale et al., 2006; Thompson et al., 2016). These differences in healthcare utilization may be exacerbated in persons with dementia (PWD) due to a variety of factors, such as the need for individually catered care plans (Bamford & Walker, 2012; Bartlett et al., 2018; Mejia-Arango et al., 2020).
Dementia is a global public health challenge, with PWD needing tailored medical and social services to ensure high-quality healthcare (World Health Organization [WHO], 2023). Nonetheless, PWD have poorer access to healthcare, have higher rates of emergency department (ED) visits, spend more time in the ED, are 65% more likely to be admitted to the hospital, have higher rates of long-term care admissions (WHO, 2023; Prince et al., 2012; Prince et al., 2016), and have higher mortality rates (Giebel, 2020; Hapca et al., 2018) compared to their older adult counterparts. Although this evidence implies the presence of health inequities across multiple healthcare utilization indicators for PWD, we lack a full understanding of the scope of healthcare utilization of men and women with dementia. Indeed, the literature on sex-based differences in health service utilization in PWD is young and evolving (Bartlett et al., 2018; Nebel et al., 2019). Existing studies have examined sex or gender differences in PWD with a few indicators only, from one or two care settings, such as pharmacological care (Trenaman et al., 2019), long-term care (Gruneir et al., 2013; Stall et al., 2019), or acute care (Milani et al., 2016). Only one study has explored sex-based differences in PWD using indicators covering multiple care settings (Sourial et al., 2020). Potential sex-based differences in the management of dementia care continue to be a neglected component of dementia research, demonstrating a need for sex-based comparisons of healthcare use of PWD (Bartlett et al., 2018; Nebel et al., 2019; Trenaman et al., 2019).
Understanding how men and women with dementia use health services is important because dementia disproportionately impacts older women (Bamford & Walker, 2012), who are more likely to live alone (Webber et al., 1994). Furthermore, women make up nearly two-thirds of persons with dementia (Alzheimer's Association, n.d.; Alzheimer's Research UK, 2022; Government of Canada, 2017; Statistics Canada, 2017). More importantly, dementia programs and health policies have not been developed with sex-based equity in mind (Powell, 2018). Understanding differences between men and women with dementia in their healthcare utilization is imperative to inform more equitable policymaking (Bartlett et al., 2018; Powell, 2018). As such, the aim of this study is to describe differences in healthcare utilization and mortality between men and women with dementia in Quebec, Canada between 2000 and 2017.
Methods
Design, Setting, and Data Source
We conducted a repeated cohort study in Quebec—Canada’s second largest province and home to 7.5 million adults aged 65 and over (Statistics Canada, 2017). Data was obtained between the fiscal years 2000–2001 to 2016–2017 from the Quebec Integrated Chronic Disease Surveillance System (QICDSS), which links five health administrative databases across the province (Blais et al., 2014; Institut national de santé publique du Québec [INSPQ], 2018). The QICDSS contains data on services provided by the publicly funded universal healthcare system (e.g., primary care visits, hospital services and prescription drugs) and links this data with individual level demographics and mortality. The QICDSS offers an opportunity to study sex differences on healthcare utilization and mortality at a population level, covering 99% of the population aged 65 and over in Quebec (Blais et al., 2014).
Population
All community-dwelling older adults aged 65 and over with a new diagnosis of dementia (index date) between April 1st and March 31st for each cohort year were included. A validated algorithm from the Institute for Clinical Evaluative Sciences database and adopted by the Public Health Agency of Canada was used to establish a diagnosis of dementia (specificity = 99.1%; sensitivity = 79.3%) (Jaakkimainen et al., 2016). A diagnosis of dementia ascertained by one of the following criteria: (a) one hospitalization with a dementia code, (b) three or more physician visits with a dementia code, (c) a dementia specific prescription (See Supplemental file 1 for details on dementia diagnosis and establishment of community-dwelling).
In addition, we opted for person-centered language, in accordance with dementia-friendly language guidelines (Alzheimer Society Canada, 2017). Consequently, even though our variable is sex, we have chosen to employ the terms “men” and “women” to align with a more humane and inclusive communication style. Furthermore, we acknowledge the intertwined influence of biological and sociocultural factors on the human experience of healthcare service use.
Study Variables
We selected and operationalized 23 indicators from a validated framework of primary care performance and healthcare utilization for PWD (Godard-Sebillotte et al., 2021; Sourial et al., 2022). We measured each event of service use during the year following diagnosis, or until long-term care admission or death (more details in Supplemental file S2).
We grouped these indicators into five care settings: ambulatory care, pharmacological care, acute hospital care, long-term care, and mortality. Their operational definitions are provided in Supplemental file S3.
Ambulatory Care
We used five indicators for ambulatory care: (1) visits to family physicians, (2) continuity of care in the two years before the diagnosis, (3) continuity of care in the year after diagnosis, (4) First record of dementia in primary care, and (5) visits to cognition specialists. Missing data for the year 2011–2012 for the indicator First record of dementia in primary care is due to the fact that the physician code was not collected consistently in the pharmaceutical database during that year.
Pharmacological Care
We used six indicators for pharmacological care, three of which pertained to general pharmacological care: (1) cholinesterase inhibitor prescriptions, (2) memantine prescriptions, and (3) dementia prescriptions in primary care (cholinesterase inhibitors, or memantine). Missing data for the year 2011–2012 for the dementia prescriptions in primary care indicator is due to the fact that the physician code was not collected consistently in the pharmaceutical database during that year. The remaining three indicators were related to potentially inappropriate pharmacological care: (4) benzodiazepine prescriptions, (5) antidepressant prescriptions, and (6) antipsychotic prescriptions. These medications were categorized as potentially inappropriate pharmacological care following guidelines from the Canadian Consensus Conference on Diagnosis and Treatment of Dementia (Smith et al., 2020).
Acute Hospital Care
We used nine indicators for acute hospital care, four of which were from general acute hospital care: (1) ED visit, (2) number of ED visits, (3) hospitalization, and (4) days hospitalized. The other five indicators pertained to potentially avoidable use of acute hospital care: (5) ambulatory care sensitive conditions (ACSC) hospitalization for the aging/dementia population (Laberge et al., 2017), (6) ACSC hospitalization for the general population (Feng et al., 2014), (7) 30-day readmissions, (8) hospitalization with alternate level care (ALC), and (9) days hospitalized with ALC.
Long-Term Care
We used one indicator for long-term care admissions (e.g., to nursing homes where nursing services are available 24/7).
Mortality
We used two indicators for mortality: (1) mortality and (2) hospital death.
Analysis
Indicators were adjusted for age using direct standardization (Ahmad et al., 2001). The age adjustment was standardized using the distribution of the Quebec census population in 2011 as the reference population (Statistics Canada, 2022). The age groups chosen for standardization were 65–69, 70–74, 75–79, 80–84, 85–89, 90–94, and 95+ years.
We performed descriptive analyses of the baseline characteristics (mean age and standard deviation and percentage of women). To ascertain the sex-based differences, age-standardized person-year rates for the indicators were stratified by sex over 17 cohort years. These stratified rates were then graphed and visually analyzed for clinically meaningful interpretation. Differences were considered clinically meaningful upon a distinction between data points which is consistent in direction across the majority of the cohort years and presence of a temporal development on the graph (i.e., data points that are clearly distinct across multiple years would be considered clinically meaningful differences; temporal development refers to changes in the pattern of such distinction over time). We followed a two-step iterative expert consultation process to ascertain clinically meaningful differences (Sourial et al., 2020). Each of the stratified age-standardized graphs was discussed among a panel of experts comprised of a geriatrician and two primary care and health service researchers. The discussions were then expanded to a larger group of experts comprised of family physicians, an epidemiologist, a biostatistician, and a senior equity health service researcher. The presence or absence of sex-based differences in health service utilization between 2000–2001 and 2016–2017 were determined by collective consensus through this iterative process. This analysis method was chosen to avoid spurious statistically significant findings due to the large, near-population level samples (Faber & Fonseca, 2014) and to highlight clinically meaningful differences that may not be easily discerned through quantitative methods alone, without multiple testing.
Results
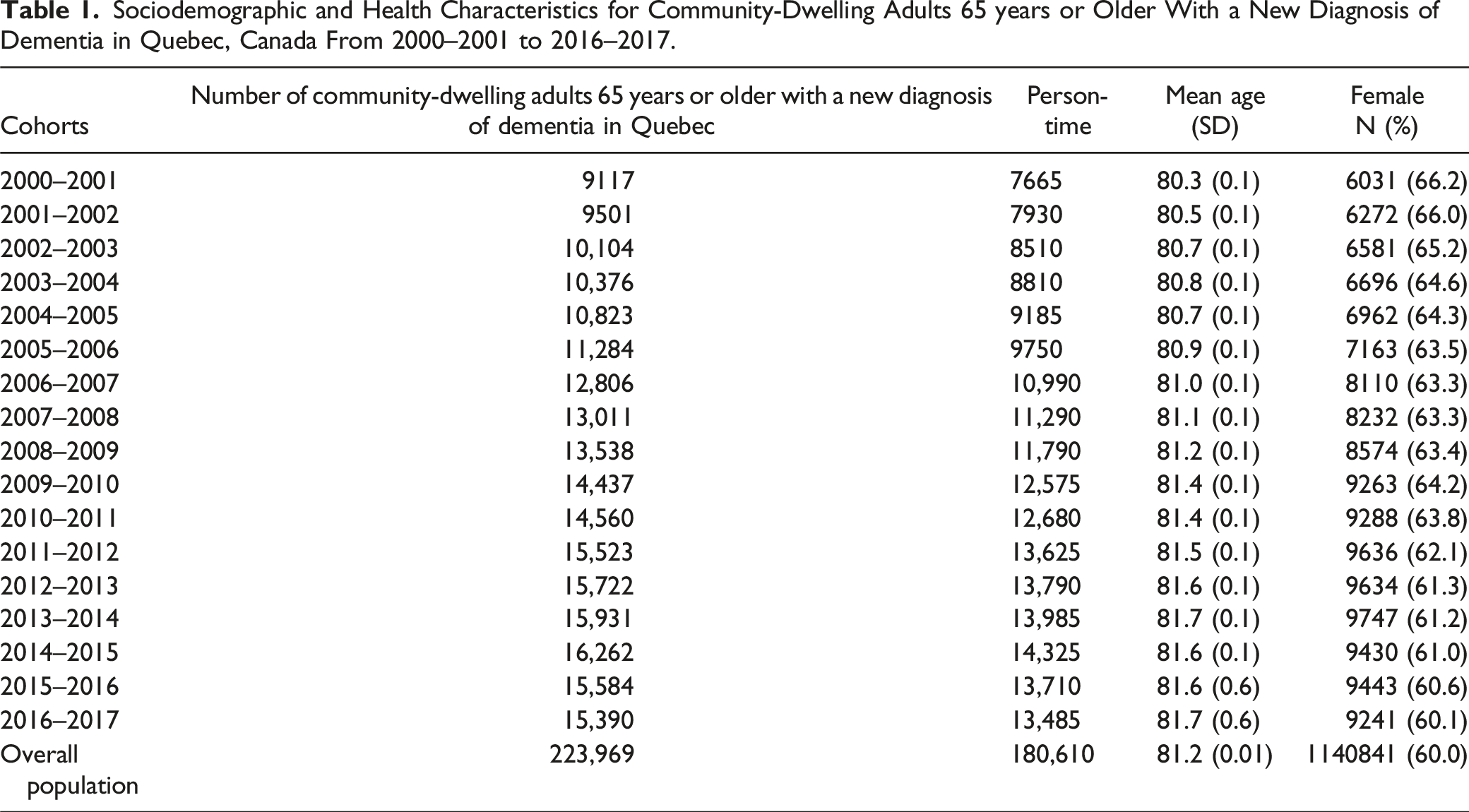
Sociodemographic and Health Characteristics for Community-Dwelling Adults 65 years or Older With a New Diagnosis of Dementia in Quebec, Canada From 2000–2001 to 2016–2017.
Ambulatory Care
Women with dementia demonstrated a higher use of ambulatory care than men with dementia for four out of five indicators: visits to primary care physicians, first record of diagnosis in primary care, continuity of care two years before diagnosis, and continuity of care in the year after diagnosis (Figures 1(A)–(D)). There was no meaningful difference in visits to cognition specialists between men and women. For example, women had more visits to primary care physicians compared to men, 17 years out of 17 years, and the rate difference was up to 0.48 visits per person-year. A breakdown of the standardized rates differences between men and women for each cohort-year and each indicator is presented in Supplemental file 4. Ambulatory care for community-dwelling adults 65 years or older with a new diagnosis of dementia in Quebec, Canada from 2000–2001 to 2016–2017 (N = 223 969). Note. This figure summarizes ambulatory care for men and women with dementia across 17 cohorts (x-axis) and age-standardized rates (y-axis). Rates for continuity of care are per 100-person-year, while those for visits to primary care physicians and visits to cognition specialists are per person-year. The blue line represents women, and the red line represents men. The panels are organized as follows: (a) rate of visits to primary care physicians in persons with dementia during the year following diagnosis; (b) continuity of care in the two years before the diagnosis; (c) continuity of care in the year after diagnosis; (d) rate of persons with a first record of diagnosis in primary care; (e) visits to cognition specialists in persons with dementia during the year following diagnosis. Note: Missing data for 2011–2012 for the rate of persons with a first record of diagnosis in primary care is due to the fact that the identification of prescribing doctors was not collected consistently in the pharmaceutical database during that year.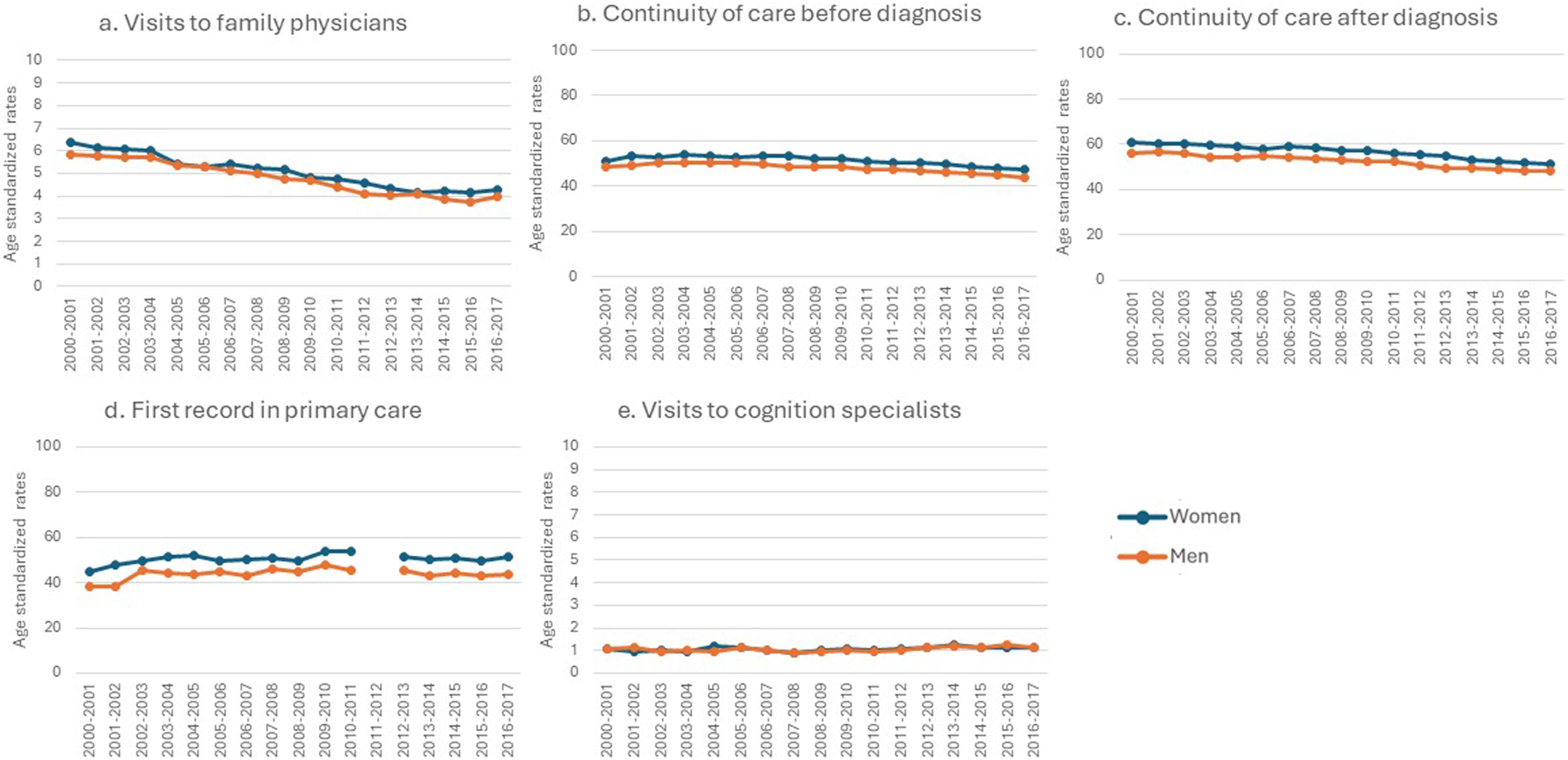
Pharmacological Care
Women with dementia had higher rates of pharmacological care compared to men with dementia for the five out of six indicators. Women had higher cholinesterase inhibitor prescriptions, dementia prescriptions in primary care, and memantine prescriptions, which was higher for women only prior to the 2009–2010 fiscal year (Figures 2(a)–(e):). For example, more women had dementia prescriptions by primary care physicians compared to men across all 17 years, and the rate difference was up to 10.7 per 100 person-year. They also had higher antidepressant and benzodiazepine prescriptions. There was no meaningful difference in antipsychotic prescriptions between men and women. Pharmacological care for community-dwelling adults 65 years or older with a new diagnosis of dementia in Quebec, Canada from 2000–2001 to 2016–2017 (N = 223 969). Note. This figure summarizes pharmacological care for men and women with dementia across 17 cohorts (x-axis) and age-standardized rates (y-axis). All rates are per 100-person-year. The blue line represents women, and the red line represents men. The panels are organized as follows: (a) rate of persons with dementia who are prescribed cholinesterase inhibitor during the year following diagnosis; (b) rate of persons with dementia who are prescribed memantine during the year following diagnosis; (c) rate of persons with dementia who are prescribed cholinesterase inhibitors or memantine by a primary care physician during the year following diagnosis; (d) rate of persons with dementia who are prescribed antidepressants during the year following diagnosis; (e) rate of persons with dementia who are prescribed benzodiazepine during the year following diagnosis; (f) rate of persons with dementia who are prescribed antipsychotics during the year following diagnosis. Note: Missing data for 2011–2012 for the rate of persons with dementia who are prescribed anti-dementia medication from primary care is due to the fact that the identification of prescribing doctors was not collected consistently in the pharmaceutical database during that year.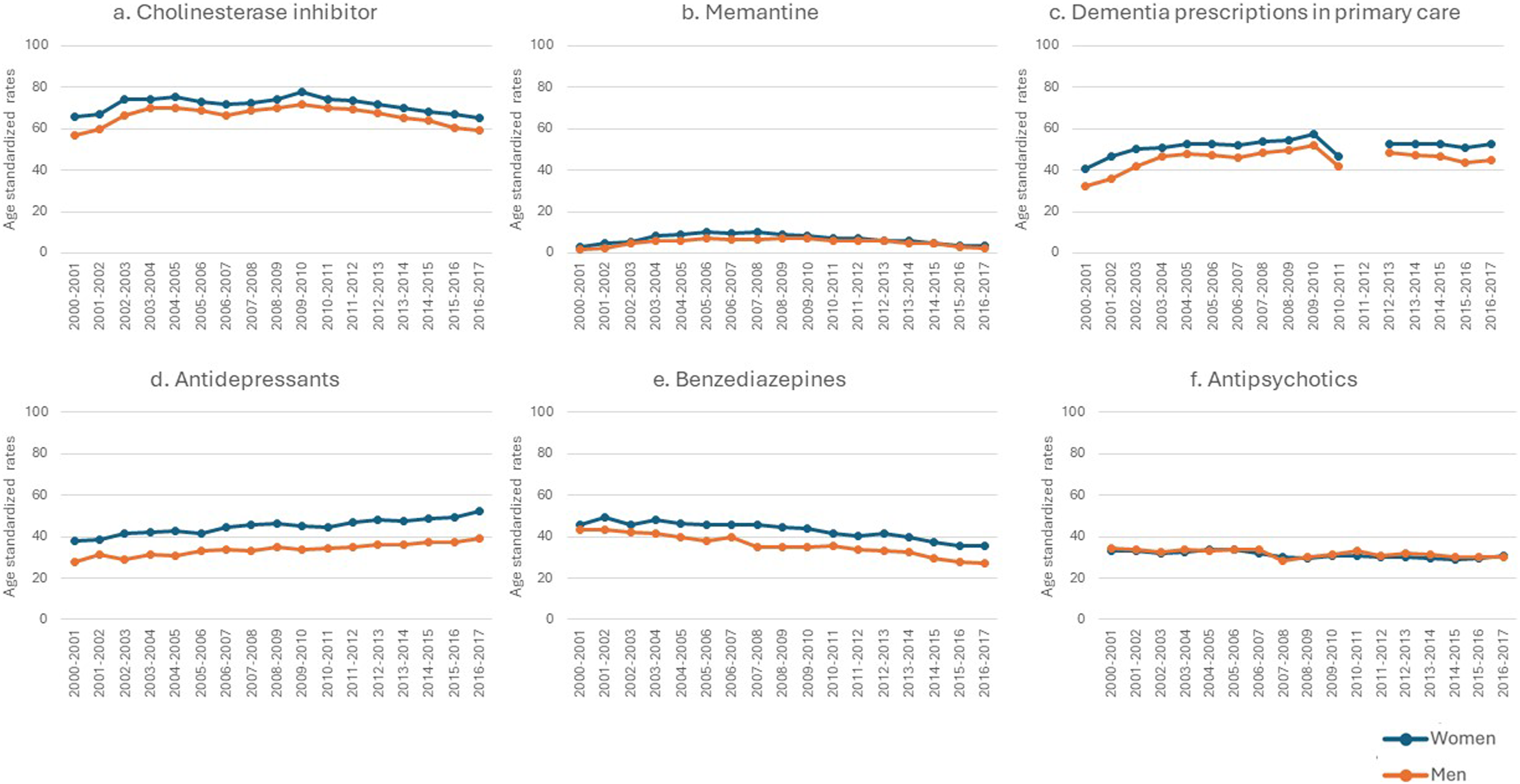
Acute Hospital Care
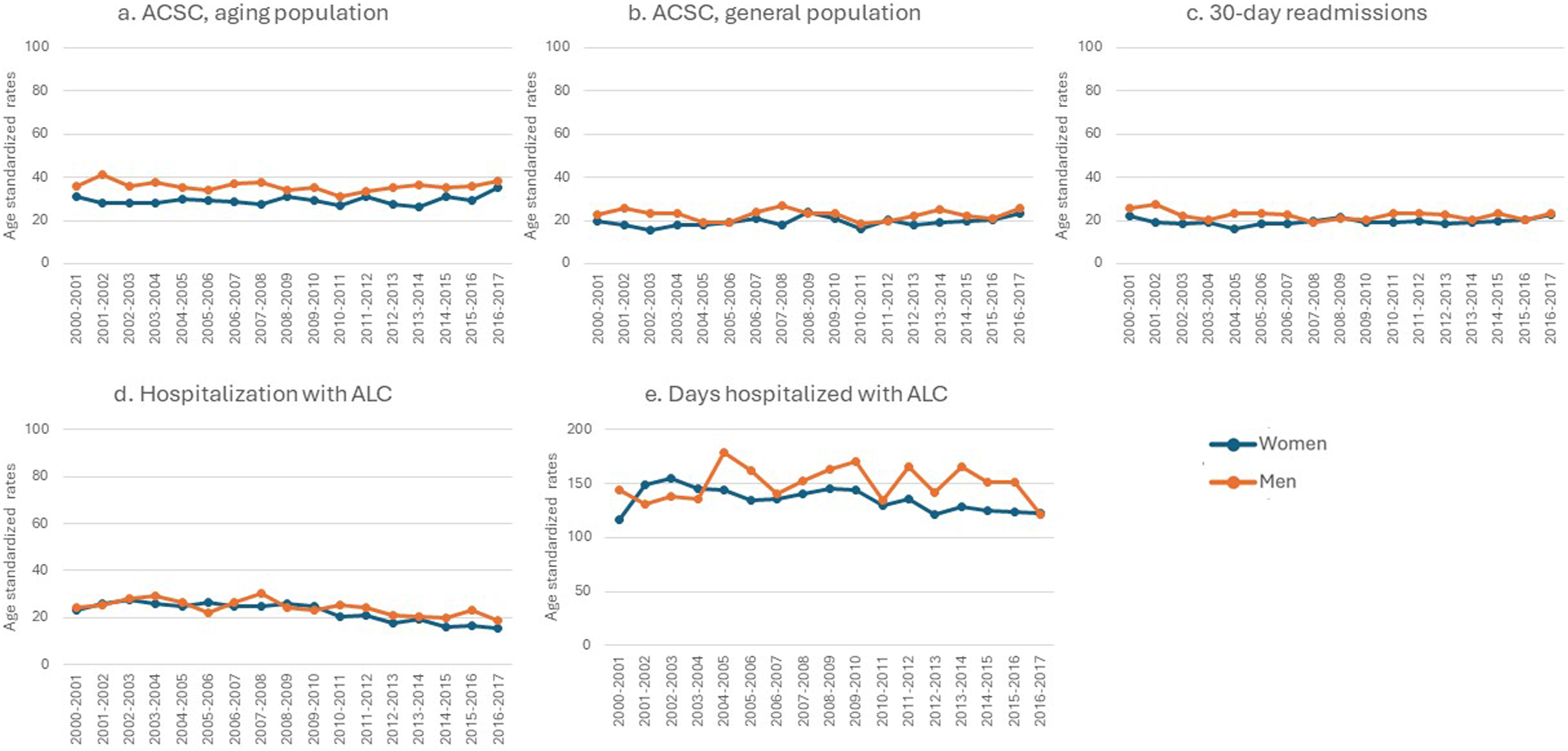
Men with dementia demonstrated higher rates of general and potentially avoidable acute hospital care use than women with dementia. This was true for three of the four indicators (Figures 3(a)–(d)): they had higher ED visits, the number of ED visits, and higher hospitalizations. For example, men had higher ED visits compared to women across all 17 years of the study, and the rate difference was up to 36 per 100 person-year. We included five indicators for potentially avoidable acute hospital care use (Figures 4(a)–(e)). Among these, men had higher 30-days readmissions (except between 2007 and 2010), a higher rate of hospitalization with ALC (especially after 2009–2010), and a higher rate of days hospitalized with ALC than women. For example, women had lower rates of alternate level care compared to men, 13 years out of 17 years. The differences between men and women on the other indicators were found inconsistent, and no trend was observed. Acute hospital care for community-dwelling adults 65 years or older with a new diagnosis of dementia in Quebec, Canada from 2000–2001 to 2016–2017 (N = 223 969). Note. This figure summarizes acute hospital care for men and women with dementia across 17 cohorts (x-axis) and age-standardized rates (y-axis). All rates are per 100-person-year, except for ED visits and days hospitalized, which are per person-year. The blue line represents women, and the red line represents men. The panels are organized as follows: A) rate of persons with dementia who have at least one emergency department (ED) visits during the year following diagnosis; B) rate of ED visits in persons with dementia during the year following diagnosis; C) rate of persons with dementia who have at least one hospitalization during the year following diagnosis; D) rate of days hospitalized in persons with dementia during the year following diagnosis. Potentially avoidable acute hospital care for community-dwelling adults 65 years or older with a new diagnosis of dementia in Quebec, Canada from 2000–2001 to 2016–2017 (N = 223 969). Note. This figure summarizes potentially avoidable acute hospital care for men and women with dementia across 17 cohorts (x-axis) and age-standardized rates (y-axis). All rates are per 100-person-year, except for days in alternate level of care, which are per person-year. The panels are organized as follows: (a) rate of persons with dementia who have at least one hospitalization with an ambulatory care sensitive condition (ACSC) for the aging/dementia population during the year following diagnosis; (b) rate of persons with dementia who have at least one hospitalization with an ACSC for the general population during the year following diagnosis; (c) rate of persons with dementia who were readmitted to the hospital within 30 days of discharge date during the year following diagnosis; (d) rate of persons with dementia who have at least one hospitalization with alternate level of care (ALC) during the year following diagnosis; (e) rate of days hospitalized with alternate level of care in persons with dementia during the year following diagnosis.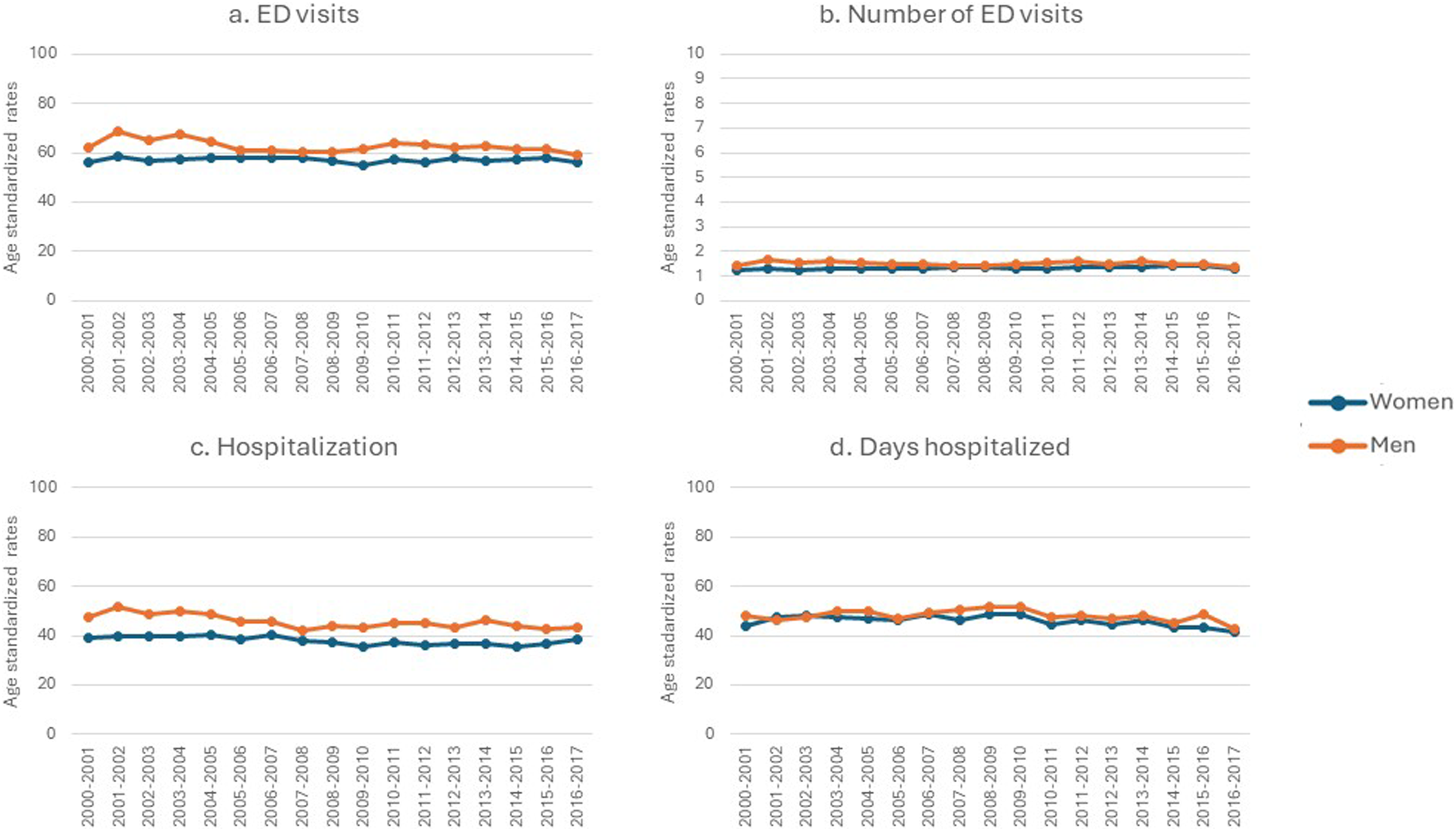
Long-Term Care
Men with dementia had higher rates of long-term care admission compared to women with dementia (Figure 5(a)). This was observed over the 17 study-years, and up to 4 per 100 person-year (Supplemental file 4). Long-term care and mortality for community-dwelling adults 65 years or older with a new diagnosis of dementia in Quebec, Canada from 2000–2001 to 2016–2017 (N = 223 969). Note. This figure summarizes long-term care and mortality indicators for men and women with dementia across 17 cohorts (x-axis) and age-standardized rates (y-axis). All rates are per 100-person-year. The blue line represents women, and the red line represents men. The panels are organized the following way: (a) rate of persons with dementia who were admitted to long-term care in the year following the diagnosis, (b) rate of persons with dementia who died in the year following the diagnosis, and (c) rate persons with dementia who died at a hospital during the year following the diagnosis.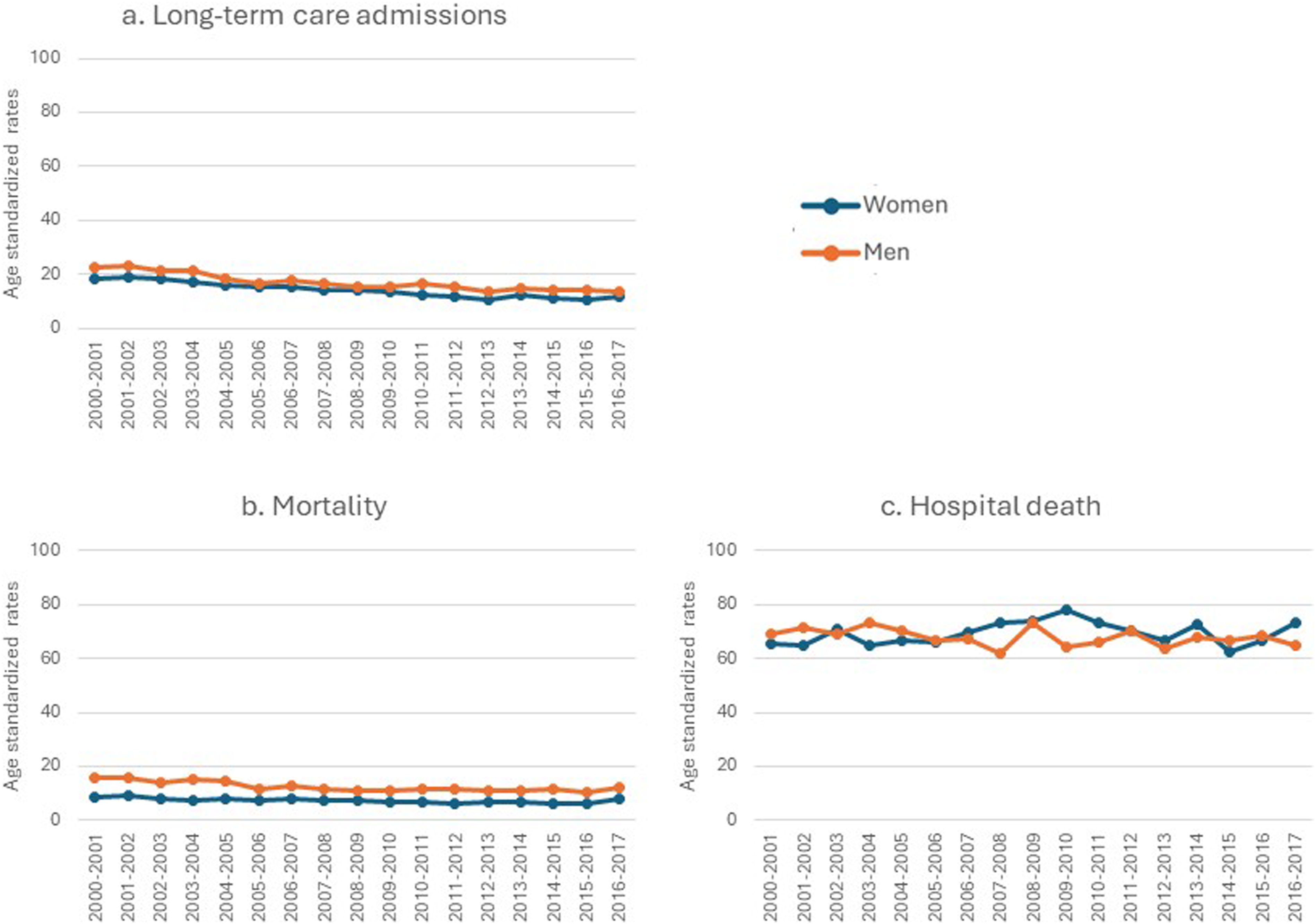
Mortality
Men with dementia had higher rates of mortality than women with dementia (Figure 5(b)), this was observed across the 17 years of the study, and the rate difference was up to 6.7 person-year (Supplemental file 4). There was no meaningful difference in the rate of persons who died at a hospital between men and women (Figure 5(c)).
Discussion
We found consistent differences in healthcare utilization between men and women with dementia in Quebec, Canada. Overall, between the fiscal years 2000–2001 and 2016–2017, women with dementia demonstrated higher use of ambulatory care and pharmacological care, while men with dementia demonstrated higher acute hospital care, long-term care admission, and mortality. Out of a comprehensive set of 23 indicators distributed across multiple care settings (ambulatory care, acute hospital care, pharmacological care, long-term care, and mortality), there were only 3 indicators where no differences between men and women with dementia were observed—rate of antipsychotic prescriptions, rate of visits to cognition specialists, and rate of persons who died at a hospital.
Our observations that women with dementia demonstrate higher use of ambulatory and pharmacological care, while men with dementia are more likely to seek acute hospital care, may be best explained by the following factors. It is likely that these sex-based differences in health service utilization in PWD are due to various biological and social factors, such as longevity, disease severity, comorbidity, and health seeking behaviors. On the other hand, it has been demonstrated that women with dementia may be more inclined to take charge of their health and seek out ambulatory care on their own (Forbes et al., 2008), while men with dementia may be less likely to visit a family physician (Galdas et al., 2005; Tudiver & Talbot, 1999). This delay in visiting a family physician may result in more severe dementia and/or more severe comorbidities, which may then result in higher acute hospital care and mortality as observed in our study. Indeed, improving continuity of care with the family physician has been shown to decrease ED visits and hospitalizations including in persons with dementia (Godard-Sebillotte et al., 2021; Menec et al., 2006). While it is known that generally, men with or without dementia demonstrate comorbidities of greater severity and prevalence than women (Gambassi et al., 1999; Milani et al., 2016; Rajamaki et al., 2021), this should not justify their higher use of potentially avoidable hospital care as observed in our study.
Similarly, higher prescriptions for any medications, including disease-modifying medications for dementia, in women with dementia may be due to higher frequency of visits to primary care physicians (Lane et al., 2021). Higher prescriptions for benzodiazepine and antidepressants may be due to the fact that there is a higher prevalence of depression (Fuhrer et al., 2003) and anxiety (Potvin et al., 2011) among women with dementia than men. Alternatively, it is known that men are less likely to receive anti-dementia medications than women because they are more likely to have drug contraindications for cardiovascular diseases (Newman et al., 2005) or different subtypes of dementia (Podcasy & Epperson, 2016).
Sex-based differences in general pharmacological care of PWD has been relatively more explored in the literature. A scoping review (Trenaman et al., 2019) found that community-dwelling women with dementia were more likely to receive potentially inappropriate medications, especially benzodiazepines, as observed in our study. On the other hand, Trenaman et al. (2019) also presented that community-dwelling men with dementia received more antipsychotic prescriptions and more cholinesterase inhibitors, which contradicts our observations. Such discrepancies may be attributed to the fact that the studies included in this review were based in different countries, while the context in Canada may differ due to differences in health system structure.
The literature on sex-based differences in long-term care admissions for PWD also offer partial support to our findings. Two studies in Ontario, Canada found that older men and women, regardless of their dementia diagnosis status, have similar LTC admission rates (Gruneir et al., 2013; Sourial et al., 2020), which contrasts our observation of higher LTC admission rates in men. Nevertheless, there were two studies that supported our findings, demonstrating higher rates of LTC admissions among older women living in the United States (Gaugler et al., 2007; Mudrazija, 2015).
The literature on sex-based differences in ambulatory and acute hospital care in PWD also offers partial support to our findings. Congruent with our study, Sourial et al. (2020) for instance, reported that more community-dwelling women with dementia in Ontario, Canada were diagnosed in primary care than men, while men demonstrated higher ED visits, ALC, and hospital readmissions, and similar rates of ACSC were found between men and women. However, community-dwelling men with dementia in Ontario had higher rates of visits to primary care and higher continuity of care, which contradicted our findings. Other studies involving older adults without dementia from Ontario, Canada (Gruneir et al., 2013) and the United States (Cameron et al., 2010) reported higher rates of ACSC in men with dementia compared to women. It is possible that some of these indicators were measured differently in administrative databases, leading to such discrepancies. Finally, we found no Canadian literature on sex-based differences in mortality rates of community-dwelling PWD.
As the literature is still quite broad and few in number, an appropriate comparison based on the literature is difficult due to possible variations in cultural contexts and methodologies, particularly in measuring indicators. Further, more research is needed to strengthen the body of evidence to better understand the health service utilization patterns in men and women with dementia and the factors that drive these differences.
Limitations
Our study has limitations that should be considered when interpreting our results. First, our study is descriptive. We chose not to adjust or control for covariates such as disease severity or comorbidities precluding causal inference. Second, data collected from administrative databases were limited to medical acts performed by physicians who are paid on a fee-for-service basis, which may have led to an underestimation of services rendered, especially by other healthcare providers, such as nurses. It is possible that men and women use services provided by other healthcare providers (e.g., nurses or homecare service providers) differently (Forbes et al., 2008). Finally, sex as measured in administrative databases is thought to be primarily biological in nature, as attributed at birth. Nonetheless, the methodology and cultural attitudes and beliefs surrounding the distinction between sex and gender have evolved dramatically over the past 80 years. Thus, more consideration should be put into what this variable does or does not encompass by design. Despite such limitations, our study offers almost two decades’ worth of population-wide, comprehensive, and clinically meaningful overview of the scope and factors affecting sex-based differences in health service use among PWD. Not only did the database we used contain information collected from nearly all persons with dementia in Quebec (Giebel, 2020), but our multi-disciplinary team of expert stakeholders also allowed for a rich, practical, and clinically well-informed interpretation of our results.
In light of the comprehensive exploratory nature of our study, future research could examine the effectiveness of interventions targeted at improving dementia care, such as with the application of time series analysis. However, such an assessment would need to carefully consider, separately for each of the 23 indicators, all potential demographic, social and health characteristics involved in the relationship between sex and each indicator to provide a robust assessment.
Policy Implications
The findings of our study have significant policy implications across various healthcare domains. The observed lower use of ambulatory care and higher use of acute care by men with dementia suggests a potential need for targeted interventions and support tailored to their specific healthcare needs. Policymakers, health managers, and clinicians may consider initiatives such as awareness campaigns aimed at enhancing access to primary care for men. This may involve developing strategies to enhance community-based care and preventive measures to reduce avoidable hospital admissions. Access to a primary care physician has been shown to decrease emergency and hospital use in persons with dementia (Godard-Sebillotte et al., 2021). The observed higher rates of medication use by women may indicate the necessity for sex or gender-sensitive prescription guidelines and pharmacovigilance practices. Initiatives to increase public awareness, especially women, on the risk of using benzodiazepines could be an option. The reasons behind these disparities need to be explored and evaluate whether they reflect appropriate and equitable healthcare provision. Finally, the higher rates of long-term care admission and mortality among men with dementia call for a comprehensive evaluation of the support systems available to individuals with dementia, with a focus on sex and gender factors influencing outcomes. Women who are caregivers of persons with dementia suffer higher emotional burden (Duangjina et al., 2023) and may need support at home. Men with dementia may need to access more home services. Alternatively, these findings may point to better chronic diseases preventive measures in men. Policymakers may need to consider sex and gender-sensitive strategies in the planning and delivery starting with home services and prevention. Overall, these results underscore the importance of sex-specific considerations in dementia care policy development and implementation to ensure equitable and effective healthcare for all individuals with dementia. Neither the Quebec Alzheimer Plan (Bergman et al., 2009) nor the Canadian Dementia Strategy (Bergman, 2019) addressed these considerations.
Conclusions
This study offers a comprehensive, population-level assessment of sex differences in healthcare utilization and mortality for men and women with dementia in Quebec, Canada. Bringing to light such differences in healthcare utilization and mortality by men and women with dementia could help address potential inequities that arise from factors such as cultural norms surrounding sex and gender. Our findings will help inform decision-makers for the development and implementation of adequate practice guidelines and policies to promote equity in dementia care and ultimately improve the health of all men and women with dementia.
Supplemental Material
Supplemental Material - Sex Differences in Healthcare Utilization in Persons Living with Dementia Between 2000 and 2017: A Population-Based Study in Quebec, Canada
Supplemental Material for Sex Differences in Healthcare Utilization in Persons Living with Dementia Between 2000 and 2017: A Population-Based Study in Quebec, Canada by Genevieve Arsenault-Lapierre, Tammy Bui, Claire Godard-Sebillotte, Nia Kang, Nadia Sourial, Louis Rochette, Victoria Massamba, Amélie Quesnel-Vallée, and Isabelle Vedel in Journal of Aging and Health
Footnotes
Acknowledgments
We would like to acknowledge Ms Juliette Champoux-Pellegrin for contributing to production of the data visualizations.
Author Contributions
GAL, CGS, and IV contributed to the conception and design of the study. All authors contributed to the interpretation of results. TB and GAL drafted the manuscript, and all other authors critically appraised its contents. All authors approved the final version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Canadian Institutes of Health Research Canada Graduate Scholarship for a master’s project, the Quebec Research Network on Aging (Réseau québécois de recherche sur le vieillissement) and the Canadian Consortium on Neurodegeneration in Aging (2019–2024) (CNA-137794). The Canadian Consortium on Neurodegeneration in Aging is supported by a grant from the Canadian Institutes of Health Research with funding from several partners. The funding bodies had no role in the study design, data collection, its analysis, and interpretation.
Ethical Statement
Data Availability Statement
The data that support the findings of this study are available from the Quebec Integrated Chronic Disease Surveillance System (QICDSS), but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.