
Abstract
Background:
Maternal and neonatal health outcomes are heavily influenced by equitable access to specialized healthcare providers. Globally, unequal distribution of obstetricians and gynecologists (OB/GYN) has been linked to higher maternal mortality rates and worse neonatal outcomes. In Saudi Arabia, ongoing regional disparities in healthcare infrastructure and workforce distribution continue to affect maternal and neonatal health despite reforms.
Objective:
This study aims to evaluate the regional distribution of obstetricians and gynecologists (OB/GYN) across Saudi Arabia and its impact on maternal and neonatal health outcomes.
Methods:
We conducted a cross-sectional secondary data analysis using the 2022 Saudi Ministry of Health Statistical Yearbook, covering all 20 health regions. We calculated the number of OB/GYN specialists per 100 000 females by region. Pearson’s correlation examined associations between specialist density, population size, infrastructure, and health outcomes. Multiple regression identified predictors of specialist distribution.
Results:
Specialist distribution varied widely. Rural regions, such as Qurayyat, had the highest specialist-to-female ratio (92 per 100 000), while urban regions, like Riyadh, had the lowest (53 per 100 000). A strong negative correlation existed between population size and specialist density (r = −.748, P < .001). OB/GYN bed availability was the strongest predictor of specialist distribution (β = .908, P < .001).
Conclusions:
This nationwide analysis highlights significant disparities in the distribution of OB/GYN specialists across Saudi Arabia. Urban regions are underserved relative to their population size, while rural regions often lack adequate infrastructure to support existing specialists. Addressing these imbalances through equitable workforce planning and infrastructure investment is crucial for enhancing maternal and neonatal outcomes in alignment with Vision 2030 goals.
Keywords
Introduction
Maternal and neonatal health are essential to societal well-being and crucial indicators of public health.1,2 Ensuring equitable access to obstetricians and gynecologists (OB/GYN) reduces maternal and neonatal mortality, improves health outcomes, and promotes healthcare equity. 3 While Saudi Arabia has made notable progress in lowering maternal and neonatal mortality rates, with maternal mortality decreasing to about 12 deaths per 100 000 live births, well below the global average of 211, 4 disparities still exist. Prematurity, congenital anomalies, and low birth weight remain significant contributors to neonatal deaths. In Jeddah, low birth weight was identified as a leading cause of perinatal mortality, representing 87% of cases. 5 These challenges highlight the importance of addressing inequities, especially in underserved regions, where disparities in healthcare infrastructure and access further worsen maternal and neonatal health outcomes.6,7
Saudi Arabia’s Vision 2030 initiative has emphasized the importance of reducing these inequalities through strategic efforts to enhance healthcare infrastructure, increase the availability of healthcare providers, and improve outcomes nationwide. 8 As part of Vision 2030, the Health Sector Transformation Program emphasizes enhancing service accessibility, improving quality, and implementing preventive measures against health risks. 9 Despite these efforts, regional disparities persist as a significant barrier, particularly in rural areas with limited access to healthcare. 4
Implementing the new Model of Care under Vision 2030 focuses on six dimensions of care, including women’s and children’s health, to ensure optimal coverage and timely access to skilled care when needed. 10 These initiatives represent pivotal steps toward achieving equitable access to healthcare and improving maternal and neonatal outcomes. Continuous evaluation and adaptation of these strategies are essential to meet the evolving healthcare needs of the population and align with Vision 2030’s broader goals. 11
This study examines the regional distribution of OB/GYN specialists and their impact on childbirth outcomes. However, despite progress in reducing maternal and neonatal mortality in Saudi Arabia, few studies have systematically examined how OB/GYN specialists are geographically distributed across regions or explored the effects of this distribution on maternal and neonatal health. Addressing this gap is crucial for informing policy decisions, supporting Vision 2030 goals, and promoting more equitable healthcare delivery.
Methods
This study employed a secondary data analysis approach to examine the regional distribution of OB/GYN services throughout Saudi Arabia and their relationship with maternal and neonatal health outcomes. Data were obtained from the 2022 Saudi Ministry of Health (MOH) Statistical Yearbook, which provides anonymized and aggregated health-related statistics. 12 Key variables analyzed included the number of OB/GYN specialists, population data, childbirth outcomes (total deliveries, live births, abnormal and normal deliveries), healthcare infrastructure (OB/GYN beds), and surgical interventions related to obstetrics and gynecology. Because this study analyzed national-level data covering all 20 health regions reported in the MOH Yearbook, a formal sample size calculation or power analysis was not applicable.
Inclusion criteria for this study were established based on aggregated national health system data. All 20 health regions listed in the 2022 MOH Statistical Yearbook were included in the analysis. Only obstetrics and gynecology specialists with clearly defined regional placements were considered, while those categorized under “Other Government” or MOH headquarters without regional designation were excluded. The specialist workforce examined consisted of residents, registrars, and consultants, grouped under the category of OB/GYN specialists. Maternal and neonatal service indicators analyzed included total deliveries, abnormal and normal deliveries, live births, OB/GYN beds, and surgical procedures. No individual patient data were utilized.
Descriptive and inferential statistical techniques were used to assess patterns and disparities in the distribution of OB/GYN specialists. To standardize comparisons, the ratio of OB/GYN specialists per 100 000 female population was calculated for each region. The color shading in Tables 1–3 represents the relative magnitude of values across regions, with green indicating higher values and red indicating lower values. The shading is used for visual comparison only and does not denote statistical significance. Pearson’s correlation was employed to examine the relationships between the distribution of OB/GYN specialists and maternal and neonatal healthcare outcomes. Correlation coefficients (r) were interpreted as weak (.10 to .29), moderate (.30 to .49), or strong (⩾.50), in line with established conventions in health research.
Additionally, regression analysis was conducted to evaluate the predictive influence of factors such as total deliveries, live births, OB/GYN beds, and surgical procedures on the distribution of specialists. These analyses helped identify trends, disparities, and potential gaps in resource allocation across the 20 health regions of Saudi Arabia.
Results
The total OB/GYN workforce in various healthcare sectors across Saudi Arabia was reported to be 7181. However, 520 specialists employed in “Other Government” or at the Ministry of Health (MOH) headquarters were excluded from the regional analysis. These specialists, whose employment regions were not detailed in the MOH Yearbook, primarily served groups such as the military and defense sectors. After excluding these 520 specialists, the adjusted OB/GYN workforce analyzed totaled 6661, representing approximately 93% of the total workforce reported by the MOH.
The total female population across all health regions is 12 562 339, supported by 6661 specialists. Riyadh has the largest population (3 209 408) and the highest number of specialists (1691), while Qurayyat has the smallest population (49 741) and the fewest specialists (46). Other regions with notable specialists include Jeddah, which has 926 specialists, and the Eastern Region, which has 665. In contrast, regions like Al-Bahah and Northern Borders have comparatively fewer specialists, each with 114.
The 2022 data highlights a significant relationship between the distribution of OB/GYN specialists and key service delivery metrics across Saudi Arabia. A color-coded scale visual representation underscores these findings: regions like Riyadh are shaded in green, reflecting substantial resource allocation and superior healthcare delivery, while regions such as Qunfudah are shaded in red, indicating resource deficiencies and lower healthcare outputs (Table 1).
Ranked Distribution of Health Regions in Saudi Arabia by Number of OB/GYN Specialists (2022). 12 .
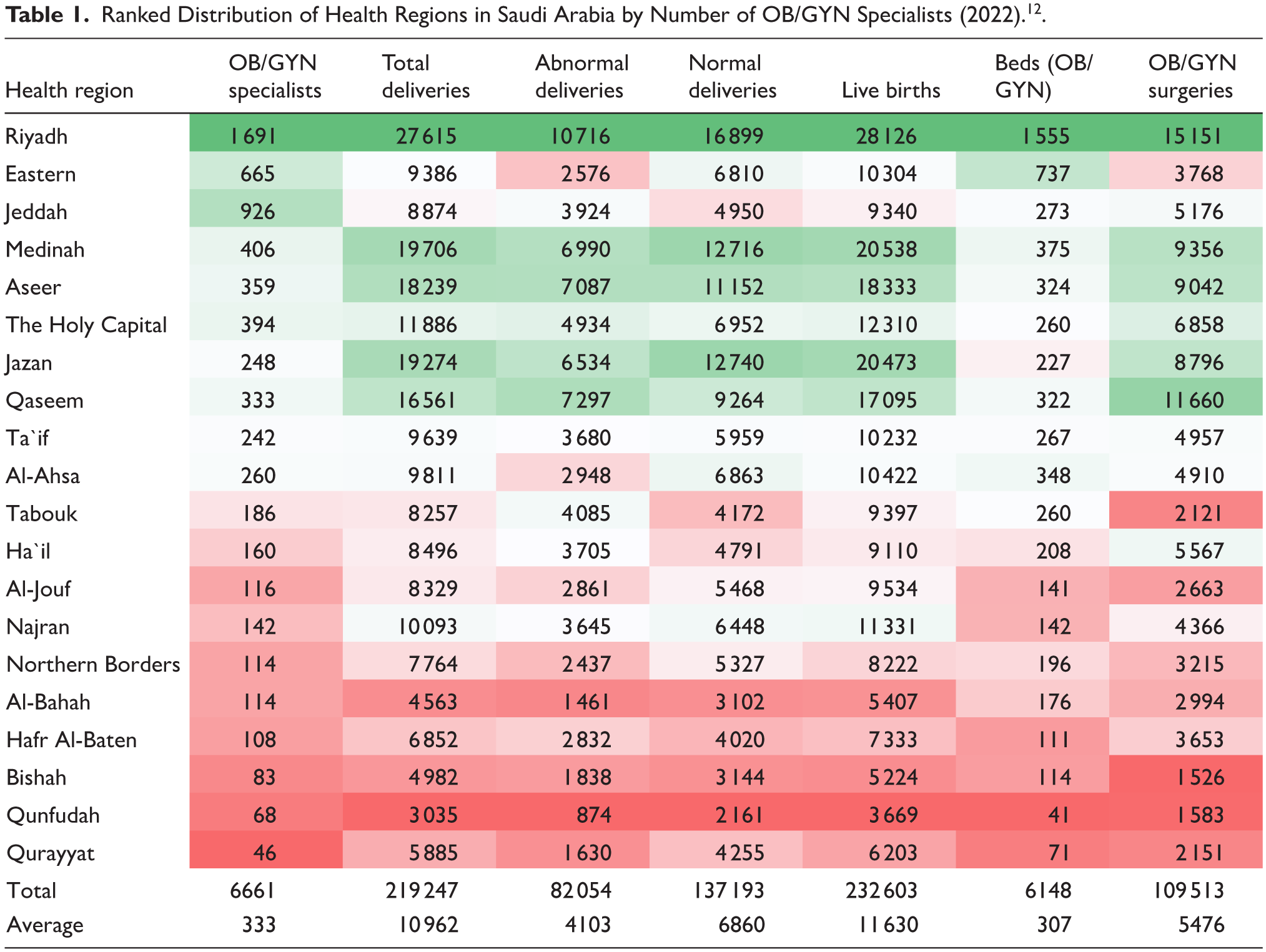

Regions with a higher density of OB/GYN specialists consistently report better healthcare outcomes, including higher rates of total deliveries, live births, and OB/GYN surgical procedures. Riyadh, which has the highest number of specialists (1691), exemplifies this trend, leading in service metrics such as total deliveries (27 615), live births (28 126), and OB/GYN surgeries (15 151).
Conversely, regions with fewer specialists, such as Qunfudah (68 specialists) and Qurayyat (46 specialists), exhibit significantly lower volumes across all service metrics. Total deliveries in these regions are notably reduced, at 3035 and 5885, respectively, along with a decrease in live births, at 3669 and 6203. Similarly, bed capacity closely aligns with the availability of specialists. Resource-rich regions, such as Riyadh with 1555 OB/GYN beds and the Eastern region with 737 beds, demonstrate substantially greater service capacity. In stark contrast, Qunfudah and Qurayyat, with the lowest bed counts of 41 and 71, respectively, face significant challenges in managing high patient volumes and responding to emergencies.
Table 2 highlights a positive overall alignment between OB/GYN specialist-to-100 000 female ratios and service outcomes throughout Saudi Arabia, indicating effective resource distribution in most regions. Areas such as Qurayyat and Hafr Al-Baten, featuring the highest ratios (92 and 82 specialists per 100 000 females, respectively), exhibit strong performance across key metrics, including total deliveries (11 831 and 5217) and live births (12 471 and 5583).
Regional Ratios of OB/GYN Specialists and Service Delivery Metrics Per 100 000 Females in Saudi Arabia. 12 .


However, certain regions exhibit dynamics that require further investigation. For instance, Jeddah, despite having a relatively high specialist ratio (67 per 100 000 females), reports lower service metrics, such as total deliveries (640) and live births (673). These disparities may be influenced by factors beyond specialist availability, including population demographics or systemic inefficiencies: Riyadh and the Holy Capital display similar patterns, with service outcomes slightly lagging behind their workforce ratios. In contrast, the Eastern Province, with the lowest specialist ratio (36 per 100 000 females), highlights the ongoing need for improved resource allocation in underserved areas (Table 2).
Regional Distribution of OB/GYN Specialists
The distribution of OB/GYN specialists throughout Saudi Arabia reveals significant regional disparities, particularly when adjusted for population size. Densely populated areas, such as Riyadh, with a population of 3 209 408, and the Eastern Province, with 1 855 376 residents, exhibit relatively low OB/GYN specialist densities of 53 and 36 specialists per 100 000 females, respectively (Table 3). Likewise, areas such as Medinah, which has 47 specialists for a population of 859 866, and Jazan, with 41 specialists serving 604 418 residents, demonstrate similar patterns.
Population and OB/GYN Specialist Distribution Across Health Regions in Saudi Arabia (2022) – Ranked by Population. 12 .


Compared to densely populated areas, smaller regions like Qurayyat (population 49 741) and Qunfudah (population 90 779) boast higher densities of OB/GYN specialists, with 92 and 75 specialists, respectively. Likewise, Al-Bahah has 79 specialists serving 144 916 residents, while Hafr Al-Baten has 82 specialists for 131 347 residents, indicating higher ratios in these regions.
The Correlation Between OB/GYN Specialist Densities and Key Metrics
Pearson’s correlation analysis revealed significant relationships between OB/GYN specialist densities and various factors. A strong negative correlation was noted between the number of specialists and population size (r = −.748, P < .001), indicating that regions with larger populations tend to have fewer specialists per capita, underscoring critical resource distribution challenges. In contrast, a strong positive correlation was found between the number of specialists and OB/GYN beds (r = .721, P < .001), suggesting that regions with more specialists are also better equipped with the necessary infrastructure for maternal healthcare services. Interestingly, the correlations between the number of specialists and service metrics, such as total deliveries, live births, and surgeries, were weak and statistically insignificant (Table 4).
Pearson’s Correlation Coefficients Between OB/GYN Specialist Densities and Key Variables.

Regression Analysis
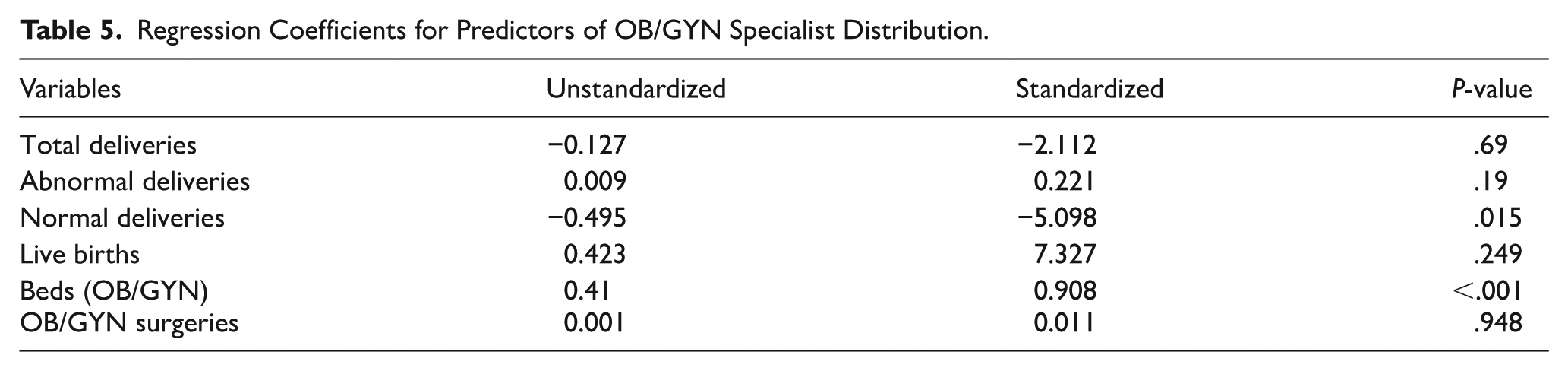
The regression analysis revealed a strong predictive relationship between the number of OB/GYN specialists and key healthcare variables, with an R2 of .731, indicating that the included predictors explain 73.1% of the variance in the number of specialists. The overall model was statistically significant (F(6, 13) = 5.902, P = .004), with OB/GYN beds identified as the most critical predictor (β = 0.908, P < .001).
Normal deliveries demonstrated a significant negative relationship with the number of specialists (β = −5.098, P = .015), while other predictors showed weak or insignificant associations (Table 5).
Regression Coefficients for Predictors of OB/GYN Specialist Distribution.
Discussion
This study reveals significant disparities in the distribution of OB/GYN specialists and supporting infrastructure across Saudi Arabia, as well as ongoing challenges in achieving equitable maternal and neonatal healthcare outcomes. Urban-rural disparities persist despite the reforms implemented for Vision 2030, affecting the workforce and infrastructure. Urban populations, particularly in Riyadh and Jeddah, are relatively resource-rich but have experienced a decline in specialist density, given their large population sizes, resulting in delays in service delivery. In contrast, more rural areas, such as Qurayyat and Qunfudah, have a higher ratio of specialists to the population but lack essential infrastructure, including OB/GYN beds, to manage complex cases effectively. These findings align with global evidence13,14 that consistently identifies infrastructure gaps as a significant barrier to healthcare equity.
Beyond these broad disparities, the analysis demonstrates a strong correlation between workforce distribution and healthcare performance, highlighting the crucial role of equitable specialist allocation in achieving improved maternal and neonatal health outcomes. In several regions, such as Al-Bahah and Bishah, resource availability and service outputs appear well balanced, suggesting that effective alignment between workforce capacity and population needs is achievable. Such examples provide insights into potential best practices for other regions.
Conversely, certain areas illustrate systemic inefficiencies. Jeddah, Riyadh, and the Holy Capital report relatively high specialist-to-population ratios yet show lower service outputs, suggesting that workforce availability does not always translate into improved healthcare delivery. On the other hand, the Eastern Province demonstrates persistent shortages despite being one of the most densely populated areas. These mismatches suggest that specialist numbers alone are insufficient to ensure optimal performance and that broader system-level factors also influence maternal and neonatal outcomes.
The regression analysis reinforces this interpretation by identifying the number of OB/GYN beds as the most significant predictor of workforce distribution. This finding highlights the crucial role of infrastructure in shaping service capacity, underscoring that adequate facilities and support must complement the availability of specialists. Without this balance, workforce distribution risks being underutilized, thereby reducing its potential impact on outcomes.
The observed negative association between OB/GYN specialists and normal deliveries requires careful interpretation. Normal deliveries are typically managed by nurse-midwives or general practitioners, rather than OB/GYN specialists, so including them as a predictor may not accurately reflect specialist demand. This could explain the inverse relationship observed in the regression model. Rather than suggesting that the OB/GYN workforce is less effective, the finding highlights the need to consider skill mix in maternal care, where nurse-midwives play a key role in managing uncomplicated deliveries. Future analyses should account for this division of labor to prevent misinterpreting the role of specialists in service outcomes.
Our findings reflect a broader trend seen both within Saudi Arabia and globally, where geographic disparities in healthcare resource distribution continue. A recent study analyzing the nursing workforce across Saudi Arabia showed that nurse-to-population ratios vary significantly, from 3.13 to 9.89 per 1000 people across regions, with a national Gini coefficient of 0.48 indicating notable regional inequality. 15 Similarly, an analysis of hospital bed distribution in 2022 reported a national average of 2.43 beds per 1000 people. Still, it highlighted critical shortages in urban areas, such as Makkah and Jeddah, despite higher absolute resource figures, which mirrors our observation of underperforming service outputs in regions with a high density of specialists. 16
These local patterns resonate with other trends: for instance, regional analyses of primary healthcare centers revealed that Riyadh had a relatively high PHC-per-capita ratio (7.5 per 100 000). At the same time, Jeddah lagged at just 3.2, underscoring persistent inequities in healthcare access even within the same national system. 14 Together, these comparisons reinforce the interpretation that specialist allocation alone does not guarantee equitable maternal and neonatal outcomes; structural infrastructure and regional system performance must be addressed in tandem.
International comparisons further reinforce these insights. In many middle- and high-income countries, equitable specialist distribution remains a challenge. For example, OECD data emphasize persistent disparities in access to specialized maternal care across regions, even when overall specialist-to-population ratios appear adequate.17-19 These parallels suggest that Saudi Arabia’s regional imbalances are part of broader global health system challenges, reinforcing the need for context-tailored workforce and infrastructure planning.
Placing these findings in a broader context, international benchmarks reveal that Saudi Arabia faces challenges similar to those faced by other middle- and high-income health systems. For example, OECD data indicate that persistent regional disparities in maternal specialist availability remain a common issue, even in countries with relatively high overall OB/GYN densities.17-19 Studies in comparable health systems, including those in the Gulf states, have also highlighted imbalances between urban and rural service provision, despite substantial investments in infrastructure. 20 These parallels suggest that the disparities observed in Saudi Arabia are part of a broader global trend, reinforcing the need for workforce planning strategies that incorporate international best practices and align with global benchmarks.
Vision 2030 presents a promising framework for addressing these disparities, primarily by promoting digital transformation and public-private partnerships. 21 Digital health technologies, such as telemedicine, could extend the reach of specialists into underserved areas, thereby mitigating the consequences of uneven geographic distribution. 22 At the same time, strengthening public-private partnerships can accelerate infrastructure development in resource-constrained rural regions. 23 Global examples demonstrate how strategic partnerships and technology-driven solutions can improve healthcare access and outcomes in resource-constrained settings. 13 Optimizing service demands, including the fair distribution of specialists, is crucial for addressing systemic inequities in healthcare. To further this goal, regional workforce retention programs will be implemented to boost workforce stability and confront disparities. These initiatives aim to transform healthcare delivery systems, aligning with the broader objectives of Vision 2030, ensuring sustainable and impactful outcomes. 21
This study highlights significant regional disparities in the distribution of OB/GYN specialists across Saudi Arabia. Larger and more densely populated regions, such as Riyadh and the Eastern Province, report lower specialist-to-population ratios than smaller regions, like Qurayyat and Qunfudah. This imbalance indicates a critical strain on healthcare resources in urban centers, while rural areas, despite having higher specialist densities, struggle with inadequate supporting infrastructure, such as OB/GYN beds. The strong negative correlation between population size and specialist density further emphasizes these challenges. Moreover, the positive correlation between OB/GYN specialists and beds underscores the essential role of infrastructure in workforce distribution.
These findings are further illustrated through regression analyses, which emphasize the significance of the number of OB/GYN beds as the most important predictor of the proportion of specialists allocated, with suggestive associations with other system outputs, such as deliveries and live births. This highlights the inefficient use of specialist availability to enhance outcomes. These results indicate that more strategic workforce planning and infrastructure investment will be necessary, particularly in densely populated regions. Addressing these systemic gaps is crucial for ensuring equitable maternal and neonatal care outcomes, aligning closely with the goals of Vision Ultimate. Finally, integrating these insights into healthcare policy reform will enable Saudi Arabia to develop a more equitable and effective healthcare system.
Based on these findings, several policy improvements can be made. Workforce planning should address not only the number and distribution of OB/GYN specialists but also focus on infrastructure development, particularly in terms of OB/GYN beds and surgical capacity. 24 Incentive programs to attract specialists to underserved urban areas, along with investments in midwifery and nursing support in rural regions, would enhance efficiency and coverage. 25 Furthermore, integrating digital health solutions, such as tele-obstetrics, and fostering public-private partnerships may help distribute care capacity more fairly across different regions. 26
Strengths and Limitations
This study has several strengths, including the use of comprehensive, nationwide data from the Saudi Ministry of Health Statistical Yearbook, which enabled a thorough evaluation of regional disparities in OB/GYN specialist distribution across all 20 health regions. The use of both correlation and regression analyses offered valuable insights into the relationship between workforce density, infrastructure, and maternal health outcomes. However, certain limitations should be recognized. Relying on secondary, aggregated data may conceal within-region variations and does not account for private sector or military-employed specialists excluded from the dataset. Additionally, the cross-sectional design limits causal conclusions, and other unmeasured factors, such as socioeconomic status, quality of care, and patient referral patterns, may also influence outcomes. Another limitation is the lack of a priori sample size or power analysis. Because the study used complete aggregated national data, it was not possible to evaluate statistical power for detecting smaller subgroup associations. Despite these limitations, the study provides substantial evidence to inform workforce planning and healthcare policy, aligning with Vision 2030 goals.
It is essential to note that our use of total deliveries as a service metric encompasses regular deliveries, many of which are typically managed by nurse-midwives rather than OB/GYN specialists. This overlap may contribute to the weak or negative correlation observed between specialist density and total deliveries. Future research should differentiate between normal and abnormal deliveries to more accurately reflect the demand for specialist services and ensure that workforce planning aligns with the specific skills needed in maternal care.
Conclusions
This study highlights significant regional disparities in the distribution of OB/GYN specialists across Saudi Arabia, underscoring inequities in access to maternal and neonatal healthcare. Rural areas such as Qurayyat and Qunfudah exhibit relatively high specialist-to-population ratios but face challenges due to inadequate infrastructure, particularly a shortage of OB/GYN beds. In contrast, urban centers such as Riyadh and the Eastern Province experience lower specialist densities due to their large populations, which may place additional strain on healthcare systems.
A strong negative correlation between population size and specialist density highlights the challenges of meeting healthcare needs in densely populated areas. Furthermore, the availability of OB/GYN beds has become a crucial factor affecting specialist distribution, emphasizing the vital role of infrastructure in determining service capacity. Despite these challenges, some areas show effective resource allocation, suggesting potential best practices that warrant further investigation.
Footnotes
Acknowledgements
The authors would like to thank the Saudi Ministry of Health for making the Statistical Yearbook data publicly available, which enabled this analysis. The author also gratefully acknowledges the Deanship of Scientific Research (DSR) at King Abdulaziz University, Jeddah, Saudi Arabia, for its technical and financial support.
Ethical Considerations
Not applicable (analysis of publicly available data).
Author Contributions
Eman Qattan led the study, which included data collection, analysis, and manuscript drafting. Waleed Kattan supervised the research process, contributed to data interpretation, and revised the manuscript for clarity and academic rigor.
Funding
The project was funded by KAU Endowment (WAQF) at King Abdulaziz University, Jeddah, Saudi Arabia. The authors, therefore, acknowledge with thanks WAQF and the Deanship of Scientific Research (DSR) for technical and financial support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available at the MOH website: https://www.moh.gov.sa. These data were derived from the following resources available in the public domain: MOH, ![]()