
Abstract
Background:
The COVID-19 pandemic posed unprecedented challenges to healthcare systems worldwide, prompting governments to rapidly expand hospital bed capacity to meet the surge in demand for medical care. This study focuses on evaluating Colombia’s healthcare system response by examining the expansion of hospital beds during the health crisis.
Methods:
In an observational study, we used a national census of all healthcare facilities in Colombia, compiled by the Ministry of Health and Social Protection (MPSP), to analyze changes in hospital bed allocation from 2010 to 2022. Our analysis accounted for the size of each provider, its public or private ownership, and the types of services it was authorized to deliver. We applied interrupted time series models to assess changes at both the hospital and municipal levels over time.
Results:
Findings reveal a significant reduction in hospital beds in 2020, with adult beds decreasing by 1049 units and pediatric beds by 0.709 units compared to 2019. However, there was an increase in ICU beds for adults across all years, which persisted after the end of the crisis. The expansion mainly targeted small hospitals and the public network of providers. Most of the expansion was restricted to areas of the country that already had a supply of ICU and hospitalization beds.
Conclusion:
Colombia’s healthcare system responded dynamically to the COVID-19 pandemic by reallocating resources and expanding hospital bed capacity, despite the complex command and control configuration of its health system. Yet, it shows that the country needs to modify its financial and organizational structures to ensure better preparedness for future health crises.
Introduction
The COVID-19 pandemic had a significant impact on all countries, affecting both their economies and healthcare systems. 1 The rapid spread of the virus changed the capacity of healthcare systems worldwide to respond to the health emergency. With little time for preparation, national systems faced high limitations and constant concerns over medical resource scarcity. 2 Many hospitals struggled with the patient surge, revealing the need for adaptive strategies suited to each country. 3 While countries with centralized healthcare systems were able to quickly mobilize resources and restructure their capacities, the situation in countries with complex, privatized insurance models remains less clear. This is particularly relevant for Colombia, where the healthcare system operates under a managed competition framework with mandatory health insurance. 4 In Colombia, where the private sector dominates healthcare provision, accounting for 95% of services in 2023, healthcare providers rely on revenue generated from insurers. This contrasts with more centralized systems and presents unique challenges in coordinating a large-scale response. Moreover, before the COVID-19 pandemic, Colombia faced a severe shortage of hospital infrastructure, with just 1.7 hospital beds per 1000 inhabitants in 2020—the third lowest among OECD countries and substantially below regional leaders like Argentina (5) or Brazil (2.1).5,6
The increase in bed capacity, alongside the mobilization of medical personnel, was a critical factor in strengthening the resilience of Colombia’s healthcare system. Strategies employed during the COVID-19 pandemic were similar across countries: the establishment of dedicated COVID-19 units, the expansion of ICU and hospital capacities, and the reallocation of healthcare staff to meet the surging demand for care.7,8 Additionally, many countries experienced a shift in the management of mild COVID-19 cases, transitioning from hospital-based care to outpatient and remote consultations. Non-urgent medical services were often canceled or postponed during the initial peak of the COVID-19 pandemic. 3
As the COVID-19 pandemic unfolded, Colombia responded with a dramatic expansion of healthcare capacity. Between June and September 2020, the number of ICU beds surged by 133.4%, and by 2022, ICU capacity had grown by 156.2% compared to pre-pandemic levels. 9 The expansion involved converting pediatric ICU beds for adults, repurposing general beds, and building new facilities. In parallel, the government expedited the graduation of approximately 2500 medical students to bolster the healthcare workforce.
This paper explores the strategies employed by Colombia to expand healthcare capacity during the COVID-19 pandemic and the lessons learned from this response. Specifically, the paper aims to: (i) assess how Colombia’s healthcare system adapted to the unprecedented demand for hospital and ICU beds, within the context of its managed competition model; (ii) analyze changes in hospital bed capacity—across ICU, intermediate, and general hospitalization—before, during, and after the crisis (2010-2022), using administrative data; and (iii) examine regional disparities in healthcare provision. We use interrupted time-series models on administrative records to achieve these objectives.
Methods
Study Design
This is an observational study based on administrative data collected by the Ministry of Health through the Special Registry of Healthcare Providers (REPS, Spanish acronym), described below. The analysis includes the complete panel of authorized healthcare facilities in Colombia from 2010 to 2022. We focus on hospital-sites with at least 1 hospitalization bed in 2019, while also exploring the extensive margin—whether facilities without beds before the COVID-19 pandemic acquired capacity.
Data and Data Processing
The national capacity of beds is primarily divided into 3 types: intensive care, intermediate care, and hospital beds. The Ministry of Health and Social Protection maintains a census of health infrastructure, REPS. The dataset includes information on hospital facilities, their characteristics, location, and the number of available beds. REPS serves as the registry of the services that legally can be provided by a health provider institution in the country in a specific year. As a result, it is periodically updated and audited by the Government and is open to the public via a web interface.
REPS allows us to identify the trends in resource availability for each hospital and provides insights into national trends. In terms of health infrastructure, it includes the number of beds and/or operation rooms by each location of a health provider institution (IPS, for its acronym in Spanish) and by the services that are authorized to provide. The data were requested from the Ministry of Health and Social Protection via a freedom of information request (derecho de petición) for a yearly version of the dataset from 2010 to 2022, allowing us to observe resource availability before, during, and after the COVID-19 pandemic. In particular, we can observe the transition that occurred as soon as COVID-19 began in 2019 and the subsequent availability of resources in the following years. We focus on hospitalization and observation beds, in particular, the total number of beds, of intermediate-level, and ICU, for both adults and children.
Sample size comprises 4357 health provider sites with infrastructure records in 1096 municipalities over 12 years (a health provider may have several sites across the country and even within the same municipality). This sample is attained as follows. The total number of sites with at least 1 capacity item (beds, rooms, ambulances, therapeutical facilities) in Colombia by 2019 was 4357 (in 1096 municipalities). Of those, 1797 (in 871 municipalities) had at least 1 hospitalization bed. The main exercise includes hospital facilities that had at least 1 hospitalization bed in 2019, but we also explore if there is a change in the probability of having at least 1 hospitalization/ICU bed.
Data cleaning procedures included checking consistency of reporting across years, removing duplicate entries, and harmonizing facility identifiers. Missing data for specific years were handled by replacing the capacity with a zero: if the site is not in REPS in a given year, it means that it was not authorized to provide that service in that site during that period. We revised the data for typos (unexpected increases or reductions in the capacity for a given site) and no amendment was deemed as required.
The main estimation relies on fixed-effect models at the provider level, supplemented by municipality-level aggregation, presented below. Descriptive and econometric analyses were conducted using STATA 18 SE.
Empirical Strategy
To compare the behavior of the healthcare system before and after the COVID-19 pandemic, we conducted a quantitative analysis using interrupted time series with panel data on potential impacts on hospital capacity. For this purpose, we perform the main analysis at the provider level. We complement this exercise with an analysis at the municipality level. The first exercise provides a view of changes within the hospital, but the municipality exercise offers a system-based strategy. 10 Colombia had 2 strategies to increase infrastructure: to create COVID-19-specific beds outside existing hospitals (eg, building beds in convention centers that were closed due to the lockdown), but mostly it was done by expanding capacities in existing hospitals and by providing hospital beds to health outposts that did not have such capabilities before. 11
We used this approach to examine changes in hospital capacity over time and assess the effects of the COVID-19 pandemic on the availability of hospital beds. Panel data allowed us to capture variations across different healthcare providers and identify any significant shifts in hospital capacity trends before and after the onset of the COVID-19 pandemic (years 2010-2022).

where
This regression model enables us to analyze how changes in hospital capacity (represented by
Results
Variation in Hospital Beds
The trend and relationship between intensive care and hospital beds have been similar for most years. The largest number of beds has been in intensive care, while intermediate care beds have been the least numerous. Figure 1 shows that since 2019, there has been an increase in hospital capacity for both intensive care and hospital beds, reaching a similar capacity in 2022 and closing the existing gap. In contrast, there has been a reduction in intermediate care beds since 2019, and in 2022, the quantity is similar to what it was in 2019.

National Hospital Capacity. Adult hospitalization beds 2010 to 2022. Own calculations using information from the Special Registry of Healthcare Providers (REPS).
Table 1 presents the empirical estimates of equation (1). Columns 1 to 3 report estimated coefficients for adult beds, while columns 4 to 6 report the estimated coefficients for pediatric beds. The first column in both cases represents hospital beds, the second represents intermediate care beds, and the third represents ICU beds.
Deviations from the trend in the number of hospitalization beds.

This table presents the results from the main specification in equation (1). Data derived from REPS that includes information from 2010 to 2022. Units are hospital-sites. Clustered robust standard errors at the municipality level are presented in parentheses.
P is significant at the 10% level. **P is significant at the 5% level. ***P is significant at the 1% level.
We found that hospital bed capacity decreased. Our estimates, robust in magnitude and significance, suggest that in 2020, the average number of hospital beds for both adult and pediatric patients decreased by 1049 and 0.709 units, respectively, compared to 2019. This reduction indicates a decline in hospital bed capacity during these years relative to 2019.
Furthermore, the average number of intermediate care beds for adults decreased by 2480 and 2345 units in 2020 and 2021, respectively. However, there was an increase in the number of ICU beds for adults in 2020, 2021, and 2022 compared to 2019. This increase was more pronounced in 2022, but significant increases were also observed in the other years.
For pediatric hospitalization beds, there was a decrease in all years, with 2021 showing the most significant reduction. As for pediatric ICU beds, there was a decrease of 1215 beds on average in 2021 compared to 2019, and 1008 beds on average in 2022 compared to 2019.
While a reduction in hospital and intermediate care beds was observed, this decline primarily reflects a substitution process, particularly in private hospitals, where resources were redirected toward expanding ICU capacity. Moreover, the overall healthcare infrastructure saw substantial growth in ICU beds, particularly in public hospitals and small healthcare facilities.
The temporary reduction in hospitalization beds was only observed in private healthcare providers. In contrast, the expansion in public hospitals provided a persistent capacity over time.
Variation Between Types of Hospitals
Table 2 presents 3 types of samples. Columns 1 and 2 have the complete sample, columns 3 and 4 have public providers, and columns 5 and 6 have private providers. The first column for each type represents hospital beds, and the second represents ICU beds.
Number of hospitalization beds according to the hospitals’ ownership.

This table presents the results from the main specification in equation (1). Data derived from REPS that includes information from 2010 to 2022. Units are hospital-sites per year. Clustered robust standard errors at the municipality level are presented in parentheses.
P is significant at the 10% level. **P is significant at the 5% level. ***P is significant at the 1% level.
In public healthcare providers, there was an increase in ICU beds during all years compared to 2019. This growth was 4234 units on average in 2020, 5318 in 2021, and 9988 in 2022. Regarding hospital beds, the most substantial increase occurred in 2022, with 1822 beds on average.
In private healthcare providers, there was also an increase in ICU beds during all years compared to 2019. The largest increase was by 1143 beds on average during 2021, followed by 1081 in 2020. These results were significant at 5%. In hospital beds, there was a reduction of 2458 units in 2020 compared to 2019.
Variation Between the Size of Hospitals
Table 3 shows differences found according to hospital size from the 25th to the 75th percentile. Columns 1 and 2 consider the complete sample. Columns 3 and 4 are for the smaller hospitals (25th percentile), while columns 5 and 6 are for larger hospitals (75th percentile). The first column in each section represents hospital beds, and the second represents ICU beds. Additionally, specific linear trends are accounted for at both the municipality and hospital facility levels.
Number of hospitalization beds according to the hospitals’ number of adult beds in 2019.
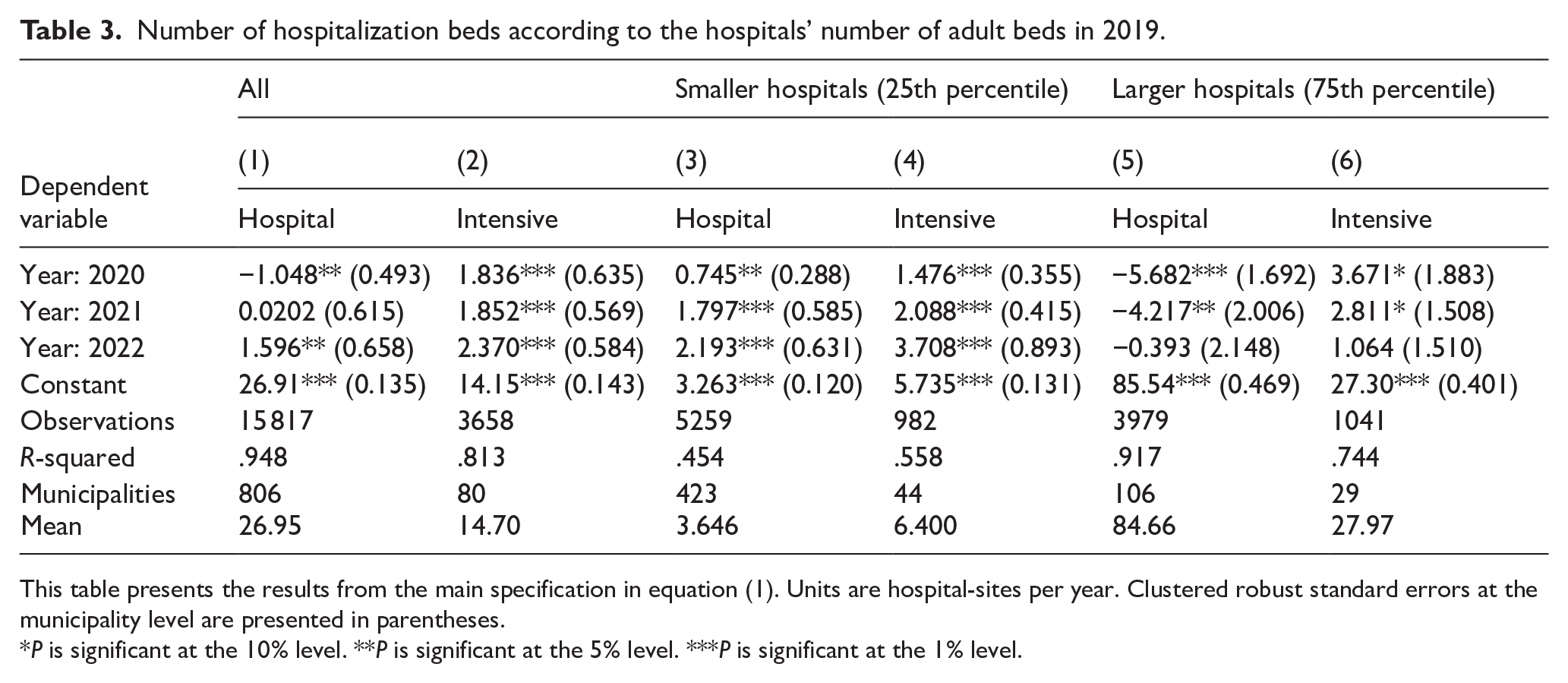
This table presents the results from the main specification in equation (1). Units are hospital-sites per year. Clustered robust standard errors at the municipality level are presented in parentheses.
P is significant at the 10% level. **P is significant at the 5% level. ***P is significant at the 1% level.
We observed that for hospitals in the 25th percentile, there was an increase in units for both types of beds during all years. The greatest increase occurred in 2022, with 2193 units on average for hospital beds and 3709 units for ICU beds compared to 2019.
In the case of hospitals in the 75th percentile, there was a decrease in hospital beds in 2020 and 2021. In 2020, there was a reduction of 5682, and in 2021, 4217. ICU beds showed a slightly significant increase in 2020 and 2021.
The significant expansion was evident in small hospitals, as evidenced by the increase in units for both observation and intensive care beds. However, in large hospitals, the adjustment was made through a reduction in hospital beds.
Extensive Margin
Table 4 shows the results for healthcare providers that had some type of authorized bed. The first column is for hospitalization beds, the second for intermediate care, and the third for intensive care.
Probability that the hospital has at least 1 hospitalization bed.
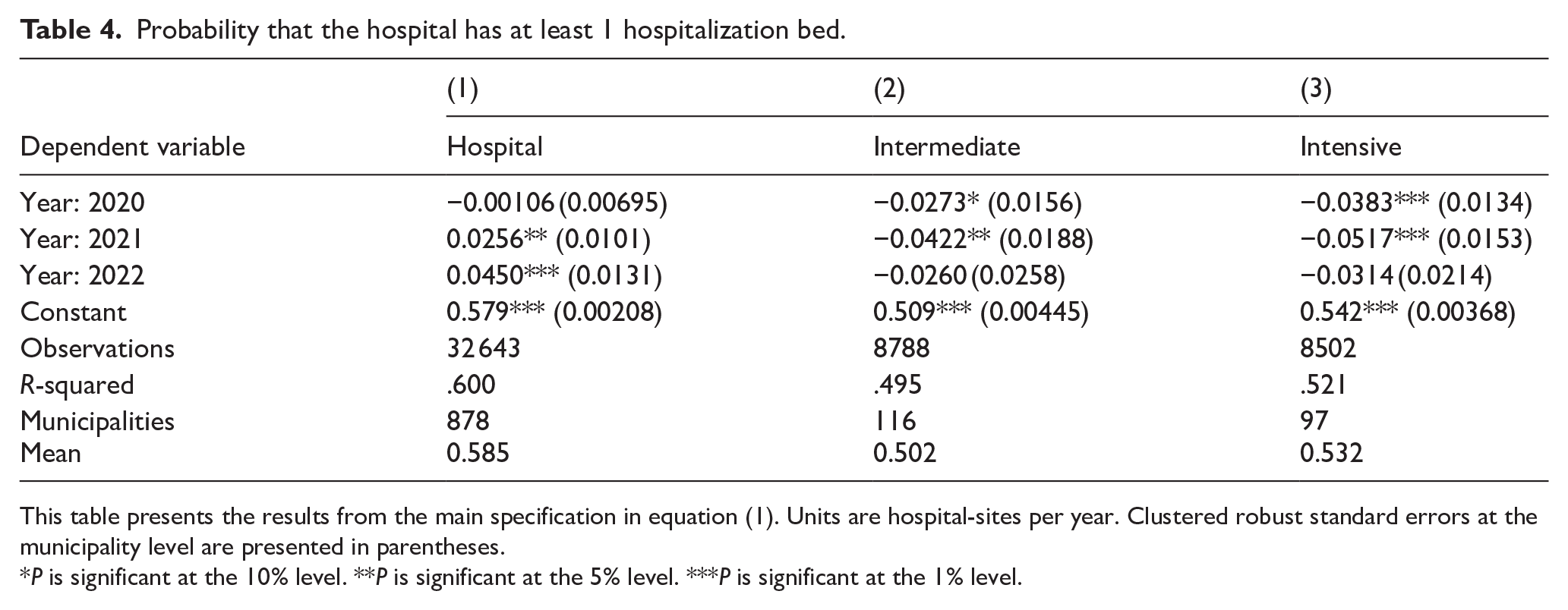
This table presents the results from the main specification in equation (1). Units are hospital-sites per year. Clustered robust standard errors at the municipality level are presented in parentheses.
P is significant at the 10% level. **P is significant at the 5% level. ***P is significant at the 1% level.
For the year 2022, the probability of having a hospitalization bed increased by 4.5 percentage points. This is compared to 57% of healthcare providers having at least 1 hospitalization bed in 2019. While there was also an increase in probability by 2.56 percentage points in 2021, this was only significant at the 5% level.
In 2019, 50.9% of hospitals with beds had an intermediate care bed. By the year 2021, there was a reduction in the probability of having such a bed by 4.2 percentage points.
Similarly, in 2019, 54.2% of hospitals with beds had an intensive care bed. The probability of having one of these beds decreased in both 2020 and 2021. In 2020, it was 3.83 percentage points lower, and in 2021, it was 5.17 percentage points lower.
Municipalities
Table 5 shows the results at the aggregated municipal level. Column 1 refers to hospital beds, and column 2 to intensive care beds.
Probability that the municipality has at least 1 hospitalization bed.

This table presents the results from the main specification in equation (1). Units are municipalities per year. Clustered robust standard errors at the municipality level are presented in parentheses.
P is significant at the 10% level. **P is significant at the 5% level. ***P is significant at the 1% level.
There was no change in the probability of a municipality having a hospital bed or an intensive care bed in any year. In 2018 and 2019, the municipal average of hospital beds was 72.7%. For intensive care beds, it was 7.2% in 2019 and 8.2% in 2022. These results underscore persistent geographic disparities in ICU availability.
Discussion
The Colombian Strategic Response: Temporal Substitution of the Usage of Beds
We contribute to understanding how the national government responded to the crisis. The changes and modifications made during this time can be understood through variations in hospital capacity. To address the question of how healthcare responded to the COVID-19 pandemic, we exploit records of available resources for the years 2010 to 2022.
Findings reveal a significant reduction in hospital beds, particularly in 2020, with adult beds decreasing by 1049 units and pediatric beds by 0.709 units compared to the expected values if the pandemic had not unfolded. Despite a decrease in hospitalization and intermediate care beds in some facilities, these reductions coincided with a significant and persistent increase in ICU capacity, especially in public hospitals and smaller facilities, indicating a strategic reallocation of resources rather than an overall contraction. Moreover, while small hospitals experienced an expansion in bed capacity, larger hospitals witnessed a reduction in beds. These findings underscore the dynamic nature of healthcare resource allocation during the COVID-19 pandemic and are in line with previous findings in the literature. 9
Colombian hospital capacity had been increasing steadily before the COVID-19 pandemic onset. In response to COVID, the country witnessed a rapid acceleration in hospital capacity expansion, particularly in terms of ICU beds. This expansion was robust in the public sector but also occurred within the private sector. In private healthcare, there was a temporary conversion of beds, with reductions in intermediate and hospitalization beds to accommodate more ICU capacity. Overall, the expansion built upon existing infrastructure, without notable changes in the availability of hospitalization or ICU beds at the municipal level. The country’s healthcare system demonstrated swift and adaptable responses in hospital capacity, amidst a period of rapid prior growth. This is encouraging, since the best performance has typically been observed in countries with centralized governance of the health system, with strong integration between inpatient and outpatient services. 12 Hence, the experience showed that despite the fragmented nature of the Colombian health system, there were efficient coordination mechanisms, a prerequisite for a successful expansion as identified in other contexts.7,13
Hospital capacity varied in the years 2020, 2021, and 2022. This variation occurred in both the number of beds allocated for adults and those for pediatric patients. The public sector concentrated an important part of this variation, which was generally positive. Private hospitals showed a substitution of beds, transitioning from hospital beds to ICU beds, a pattern already described by Prada et al. 9 Regarding hospital size, there was a notable expansion in small hospitals. This is the opposite phenomenon to what was found in China, where large hospitals drained demand from smaller ones in the post-pandemic period. 14
Equity Implications of the Pandemic Response
The disparities in hospital infrastructure across different regions have significant implications for healthcare equity. Cacace et al 12 conducted a comparative analysis of hospital structures in 5 countries, revealing that regions with underdeveloped infrastructure faced greater challenges in responding effectively to the COVID-19 pandemic. Similarly, Birchenall-Jiménez et al 15 examined spatial inequalities in Colombia, demonstrating that areas with limited healthcare facilities experienced higher mortality rates during the pandemic. These findings underscore the critical need for equitable distribution of healthcare resources to ensure all populations have access to necessary medical care.
Inequalities are exacerbated when considering ICU beds. In Colombia, fewer than 10% of municipalities had ICU capacity in 2019, and this proportion did not significantly improve during the COVID-19 pandemic. As a result, critically ill patients from remote and underserved areas were often transported to urban hospitals, leading to delays in care and increased mortality risk. Patients in those areas also faced socioeconomic characteristics linked to poverty that increased their COVID-19 mortality risk.15-17 This geographic disparity reflects structural limitations in the country’s healthcare financing and planning mechanisms. 9
The results of our analysis show that there was a missed opportunity to expand the capabilities of the system in the remote areas of the country. Anecdotally, the news showed airplanes lifting sick patients from remote areas to large cities and promises of new health capabilities in those areas to reduce such difficult interventions. The lack of change in the capabilities reflects a lack of adequate financial structure to sustain such temporary efforts over time.
To improve equity, future strategies must include targeted infrastructure investment, modular hospital units deployable in rural areas, and subsidies that incentivize service provision in remote locations. 14
Impact on the Healthcare Workforce
The rapid expansion of ICU capacity and the surge in COVID-19 cases placed extraordinary pressure on Colombia’s healthcare workforce. This expansion strategy included a significant reallocation of resources, as many general hospital beds were repurposed as ICU beds. To support this shift, the government not only expedited the graduation of approximately 2500 medical students 9 but also implemented emergency training programs for general practitioners and medical students to operate ICU equipment and provide critical care services.18,19 These crash courses and simulations were critical to temporarily bolstering the ICU workforce.
While these actions increased short-term capacity, they introduced challenges including supervision burdens, accelerated learning curves, and risks of clinical error. Moreover, surveys during the COVID-19 pandemic indicated high levels of emotional exhaustion and burnout among healthcare workers, particularly in overstretched public hospitals.20-23 These workforce challenges underscore the need for long-term investments in training, mental health support, and surge capacity planning for future health emergencies.
International Comparison and Lessons Learned
Compared to other low- and middle-income countries (LMICs), Colombia’s response showed a relatively high degree of adaptability given its fragmented insurance-based system. While Peru, which also has a fragmented health system, struggled to expand ICU capacity, Colombia leveraged existing public infrastructure and regulatory flexibility.9,24 For instance, the temporary use of non-hospital spaces (eg, a large convention center with 274 hospitalization beds) mirrored approaches in several other countries.25-27 However, unlike some Asian LMICs (eg, Vietnam or Thailand), Colombia lacked a centralized command structure to coordinate response efforts uniformly. 13 Best practices from these contexts—such as rapid mobilization teams, unified data systems, and scalable rural facilities—offer valuable insights for Colombia and similar systems. 8
While the country showed flexibility in responding to the COVID-19 pandemic despite its complex organization of multiple insurers and demand-driven providers’ revenue, Colombia must reform organizational structures to incentivize the expansion of capabilities beyond its large cities. Such changes are needed to ensure better preparedness for future health crises.
Conclusion
We present a case study showing how countries with complex, mixed healthcare models can respond to health crises. Colombia’s experience offers valuable lessons for other low- and middle-income countries with similarly fragmented systems. By analyzing both successes and shortcomings, this study contributes to global discussions on COVID-19 pandemic resilience and equity. There are 4 general conclusions from this study.
First, there was a dynamic but uneven response. Colombia demonstrated remarkable agility in reallocating healthcare resources during the COVID-19 pandemic, especially in ICU bed expansion. The public sector played a central role in this scaling-up effort, while private hospitals temporarily repurposed other types of beds. However, the focus remained on regions with existing infrastructure, leaving rural and underserved areas at a significant disadvantage.
Second, we observed a missed opportunity in rural areas. Despite the COVID-19 pandemic’s unprecedented demands, less than 10% of municipalities had ICU capacity, reflecting structural inequities in Colombia’s healthcare system. Transporting critical patients to urban centers became a necessary but inefficient stopgap. While it is true that there is a need to consider capabilities instead of capacities (who we can treat rather than the location of facilities), 28 the lack of permanent infrastructural changes in these areas suggests a missed opportunity to address longstanding healthcare disparities.
Third, the increase in ICU capacity was predominantly temporary, relying on resource reallocations rather than permanent system expansions. For example, pediatric ICU beds were repurposed for adult use, and temporary facilities were constructed. This raises concerns about whether these adaptations have left Colombia better prepared for future public health emergencies.
Fourth, the study highlights how Colombia’s fragmented healthcare system, governed by private insurers and demand-driven financing, created bottlenecks in response coordination. While the government led the ICU bed expansion, the financial burden of sustaining these investments was disproportionately placed on public hospitals, potentially compromising long-term resource allocation.
To ensure preparedness for future crises, we recommend: (i) establishing funding mechanisms to incentivize infrastructure development in underserved regions and ensure the sustainability of basic capabilities by partially subsidizing the supply of services; (ii) designing permanent infrastructure that can be rapidly scaled up during emergencies, such as modular hospital units; (iii) investing in the healthcare workforce through training pipelines, mental health support, and surge capacity strategies; and (iv) implementing equity-focused policies to close geographic disparities in critical care access.
This study offers valuable insights into how a middle-income country with a complex, mixed healthcare model responded to a health crisis. Colombia’s experience illustrates both the adaptability of fragmented systems and the structural vulnerabilities that can undermine equitable, sustainable responses. By comparing national responses, highlighting workforce and financing challenges, and analyzing equity implications, this paper contributes to the global literature on pandemic resilience and healthcare preparedness. These lessons are particularly relevant for LMICs facing similar constraints and seeking to strengthen their health systems in the wake of COVID-19.
Footnotes
Acknowledgements
We acknowledge members of the AGORA team for their valuable comments and feedback.
List of abbreviations
ICU: Intensive care units
OECD: Organization for Economic Co-operation and Development
MPSP: Ministry of Health and Social Protection
REPS: Special Registry of Healthcare Providers
Ethical Considerations
We perform an observational study based on secondary data which is publicly available by the Colombia Government. No ethics approval is required for this study in consequence.
Author Contributions
PR was in charge of the conceptualization, methodology, formal analysis, writing, resources, supervision, project administration, and funding acquisition. SR participated in the investigation, data curation, software, formal analysis, and visualization. CD was a major contributor to writing the original draft and visualization. All authors read and approved the final manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Colombian Ministry of Science and Technology through the project AGORA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.