
Abstract
Background:
Intensive care unit (ICU) patients with coronavirus disease 2019 (COVID-19), have a high risk of developing bloodstream infections (BSIs). However, the characteristics of and risk factors for BSIs in these patients remain unclear.
Objective:
We aimed to identify prevalent causative pathogens of BSI and related factors in critically ill patients with COVID-19.
Design:
This was a single-center, retrospective cohort study.
Methods:
We analyzed the clinical characteristics and outcomes of 201 ICU patients with COVID-19. Logistic regression analysis was conducted to identify factors associated with BSI occurrence. Furthermore, we identified the primary causative pathogens of BSIs. The study outcomes were death or ICU discharge.
Results:
Among the 201 included patients, 43 (21.4%) patients developed BSI. The mortality rate was non-significantly higher in the BSI group than in the BSI group (65.1% versus 58.9%, p = 0.487). There were significant between-group differences in the obesity prevalence and sex distribution, but not corticosteroid usage. BSI occurrence was significantly associated with duration of mechanical ventilation (MV), presence of ventilator-associated pneumonia, use of neuromuscular blocking agents, length of stay in ICU (ICU LOS), high body mass index (BMI), and male sex. The main causative pathogens were Klebsiella pneumoniae, Acinetobacter baumannii, and Enterococcus faecalis. Multi-drug-resistant pathogens were found in 87% of cases. Regardless of the origin, the common risk factors for BSI were ICU LOS and MV duration. All BSIs were acquired within the hospital setting, with ≈60% of the cases being primary BSIs. A small proportion of the BSI cases were catheter-related (four cases, 6.2%). Ventilator-associated pneumonia and urinary tract infections were present in 25% and 9.4% of the BSI cases, respectively. On average, the first positive blood culture appeared ≈11.4 (±9.7) days after ICU admission.
Conclusion:
Elucidating the risk factors for and common pathogens of BSI can inform prompt management and prevention of BSIs.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has led to the deaths of millions of individuals and added a burden on healthcare systems worldwide. 1 COVID-19 primarily targets the respiratory system. Most patients with COVID-19 experience mild symptoms or remain asymptomatic; however, a subset of patients progress to severe disease requiring intensive medical care. Critically ill patients with COVID-19 often present respiratory failure requiring mechanical ventilation (MV) and are admitted to the intensive care unit (ICU). 2
Bloodstream infections (BSIs) are associated with high mortality rates, prolonged hospital stay, and increased healthcare costs in critically ill patients. Hospitalized patients with COVID-19 have an increased risk of developing various bacterial coinfections, 3 which have a significant negative prognostic effect. Bacterial BSIs are of particular concern in this patient population given the pathophysiological changes induced by viral infections, the use of immunomodulatory drugs, and the extensive use of invasive devices such as MV and intravascular catheters. 4 The interaction between viral infections and BSI often prolongs MV and length of stay (LOS); furthermore, it increases the risk of complications such as infection, sepsis, or septic shock. 5 Various pathogens cause BSIs in patients with COVID-19, including both common hospital-acquired organisms and opportunistic pathogens that exploit the immunocompromise caused by COVID-19. These BSIs are especially challenging to treat given the underlying virus-induced pathophysiological changes and potential drug interactions. 6 There are varying sources of BSIs, including ventilator-associated pneumonia (VAP), intravascular catheter-related infections, and urinary tract infections. 7 Common bacterial pathogens involved in BSIs include Staphylococcus aureus, Klebsiella pneumoniae, Escherichia coli, and Pseudomonas aeruginosa. 8 Notably, multi-drug-resistant (MDR) pathogens have been identified. Furthermore, BSIs in patients with COVID-19 are associated with unfavorable clinical outcomes, including high mortality rate as well as extended duration in the ICU and on MV.
Ippolito et al. 5 reported that the prevalence rate of BSIs among ICU patients was 29.6%; additionally, the mortality rate was 41% among all hospitalized patients. This high incidence could be related to several factors, including patient age, demographics, comorbidities, MV duration, and specific therapeutic approaches for COVID-19. 9
We aimed to determine the characteristics of BSI in ICU patients with COVID-19 and to identify the risk factors and prevalent causative pathogens for BSI.
Materials and methods
Study design and population
This single-center retrospective cohort study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology statement guidelines. A total of 235 adult patients with COVID-19 were admitted to the University Clinical Hospital ICU in Bialystok, Poland, between 3 March 2020, and 1 July 2021. The inclusion criteria were as follows: age >18 years, acute COVID-19 infection confirmed by a reverse transcription polymerase chain reaction test of nasal and pharyngeal swab specimens or lower respiratory tract secretions, and ICU admission for SARSCoV-2 infection. We excluded pregnant women and patients admitted to the ICU for reasons other than COVID-19, including elective surgery or emergencies. Accordingly, we included 201 eligible participants; among them, 43 patients developed BSI. Figure 1 presents a flowchart of the selection of participants. Positivity for BSI was indicated when at least four blood samples were collected and at least two of them were positive for a clinically significant organism.10,11 This was determined prior to the commencement of antibiotic treatment in order to avoid false-negative results. 12 To decrease the risk of falsely identifying contamination cases as clinically significant,10,11 we compared the blood test results with the patient’s conditions; furthermore, as aforementioned, two positive samples were required. In case of polymicrobial infections, each causal organism identified in the blood culture was considered a unique BSI. Fever and other laboratory findings indicative of infection were considered necessary for assigning a case of BSI. Bacteremia diagnosed ⩾48 h after hospital admission was classified as hospital-acquired BSI. Primary BSI was identified if the patient lacked a definite infection source. Secondary BSI was identified when an infection source was suspected, and the same microbe as that in the source was found in the blood culture.

Flowchart of patient screening and inclusion.
Antibiotic treatment was initiated based on clinical judgment, with consideration of factors such as the presence of fever or other infection signs as well as microbiological examination.
Statistical analysis
A t-test or chi-square test was used to assess the relationships between variables, and p values were reported. Two-state logistic regression was used to investigate significant risk factors for BSI. Statistical significance was set at p < 0.05. All analyses were performed using the R software version 4.1.1. 12
Results
Table 1 presents the demographic and clinical characteristics of the patients upon ICU admission and the risk factors for developing BSI. Among 201 included patients, 43 (21.4%) patients developed BSIs (BSI group), whereas 158 patients (78.6%) did not develop BSIs (non-BSI group).
Characteristics of ICU patients with COVID-19, risk factors for BSI, disease course, treatments, and outcome.
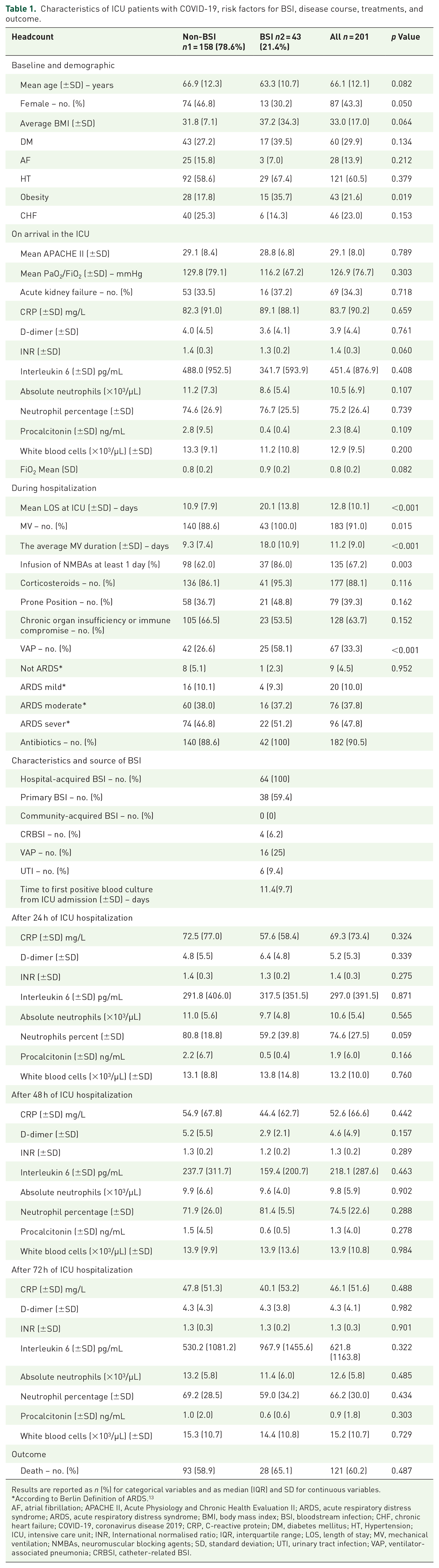
Results are reported as n (%) for categorical variables and as median (IQR) and SD for continuous variables.
According to Berlin Definition of ARDS. 13
AF, atrial fibrillation; APACHE II, Acute Physiology and Chronic Health Evaluation II; ARDS, acute respiratory distress syndrome; ARDS, acute respiratory distress syndrome; BMI, body mass index; BSI, bloodstream infection; CHF, chronic heart failure; COVID-19, coronavirus disease 2019; CRP, C-reactive protein; DM, diabetes mellitus; HT, Hypertension; ICU, intensive care unit; INR, International normalised ratio; IQR, interquartile range; LOS, length of stay; MV, mechanical ventilation; NMBAs, neuromuscular blocking agents; SD, standard deviation; UTI, urinary tract infection; VAP, ventilator-associated pneumonia; CRBSI, catheter-related BSI.
Most patients in the BSI group were women (69.8% versus 53.2%, p = 0.050). Notably, the BSI group was non-significantly younger than the non-BSI group (63.3% versus 66.9%; p = 0.082).
There were no significant between-group differences in baseline characteristics such as body mass index (BMI); sex; age; and existing conditions such as diabetes mellitus, atrial fibrillation, hypertension, and chronic heart failure. However, the percentage of patients with obesity was significantly higher in the BSI group (35.7%) than in the non-BSI group (17.8%) (p = 0.019).
Upon arrival at the ICU, there was no significant between-group difference in the mean Acute Physiology and Chronic Health Evaluation II (APACHE II) scores (p = 0.789). Similarly, there were no significant between-group differences in the other clinical and laboratory parameters such as mean PaO2/FiO2 occurrence of acute kidney failure as well as levels of C-reactive protein, D-dimer, international normalized ratio, interleukin 6 (IL-6), neutrophils, procalcitonin, and white blood cells.
During hospitalization, the ICU LOS and duration of MV were significantly longer in the BSI group than in the non-BSI group (both p < 0.001). Moreover, the BSI group had a higher incidence of VAP than the non-BSI group (58.1% versus 26.6%, p < 0.001). In addition, the BSI group had a higher rate of infusions of neuromuscular blocking agents (NMBAs) compared with the non-BSI group (86% versus 62%, p = 0.003). The usage rate of corticosteroids was high in both groups, with no significant between-group difference (non-BSI, 86.1%; BSI, 95.3; p = 0.116).
All BSI cases (n = 64, 100%) were identified as hospital-acquired BSIs. Among them, 38 (59.4%) were primary BSIs. Catheter-related BSIs (CRBSIs) comprised a small proportion of the BSI cases (n = 4, 6.2%). VAP and urinary tract infections were reported in 16 (25%) and six (9.4%) patients with BSI, respectively. The average time from ICU admission to the first positive blood culture was 11.4 (±9.7) days. A high proportion of patients in both groups was treated with antibiotics, with no significant between-group difference (non-BSI, 88.6%; BSI, 100%; p = 0.132).
Regarding laboratory parameters at 24, 48, and 72 h after ICU admission, there were no significant between-group differences.
Finally, the mortality rate was non-significantly higher in the BSI group (65.1%) than in the non-BSI group (58.9%) (p = 0.487).
Table 2 shows the logistic regression analysis of factors associated with BSI occurrence. Univariate analysis identified six factors significantly associated with BSI occurrence, including the use of NMBAs [odds ratio (OR): 3.776, 95% confidence interval (CI): 0.95–1.01, p = 0.153], ICU LOS [1.086 (0.0467–0.118), p < 0.001], BMI [1.017 (−0.01 to −0.9), p < 0.001], sex [0.492 (−1.43–0.01), p 0.05], VAP [3.836 (0.643–7.734), p < 0.001], and MV duration [1.11 (0.06–0.147), p < 0.001)]. Table 2 also shows the results of the multivariate analysis of the factors associated with the occurrence of BSI.
Logistic regression of factors associated with BSI occurrence.

APACHE II, Acute Physiology and Chronic Health Evaluation II; BMI, body mass index; BSI, bloodstream infection; CLABSI, Central Line-associated bloodstream infection; ICU, intensive care unit; Inf., infinity; LOS, length of stay; MV, mechanical ventilation; NMBA, neuromuscular blocking agent; OR, odds ratio; UTI, urinary tract infection; VAP, ventilator-associated pneumonia.
We examined factors associated with the occurrence of CRBSI. Univariate logistic regression analysis identified that the ICU LOS (OR: 1.05; 95% CI: 1.007–1.1031, p = 0.024) and duration of MV (OR: 1.06; 95% CI: 1.004–1.12, p = 0.033) were significantly associated with an increased risk of CRBSI. However, the significance of these relationships disappeared in the multivariate analysis (ICU LOS: OR 0.932, p = 0.548; duration of MV: OR 1.040, p = 0.726).
Regarding VAP, ICU LOS and duration of MV were significantly associated with VAP in the univariate analysis (ICU LOS: OR 1.0376, 95% CI 1.0077–1.0685, p = 0.013; duration of MV: OR 1.0493, 95% CI 1.0140–1.0859, p = 0.006). However, these significant associations were nullified in multivariate analysis (ICU LOS: OR 0.9885, p = 0.874; duration of MV: OR 1.0308, p = 0.726).
Regarding, primary BSI, univariate analysis revealed that ICU LOS (OR: 1.0349, 95% CI: 1.0091–1.061, p = 0.008), duration of MV (OR: 1.0470; 95% CI: 1.0164–1.079, p = 0.002), and prone positioning (OR: 2.5181; 95% CI: 1.1178–5.672, p = 0.026) were significantly associated with the occurrence of primary BSI. However, these significant associations were nullified in multivariate analysis (ICU LOS: OR 0.9556, p = 0.426; MV duration: OR 1.1009, p = 0.149; prone position: OR 2.3230, p = 0.052).
The most common circulatory pathogens were K. pneumoniae, Acinetobacter baumannii, and Enterococcus faecalis (Table 3). Bacterial pathogens responsible for BSI were classified as sensitive, MDR, or extensively drug-resistant based on the European Centre for Disease Prevention and Control definition. 11 Interestingly, most of the bacterial pathogens were MDR (87%), with only 13% present of the cases being caused by sensitive pathogens.
Causative pathogens for BSI.

BSI, bloodstream infection.
Discussion
This study investigated the characteristics of BSI characteristics in ICU patients with COVID-19 as well as the related risk factors and prevalent pathogens. BSIs occurred in only 21.4% of our study cohort. Furthermore, there were no significant between-group differences in the mortality rates. Obesity, sex, and age, but not corticosteroid usage, differed significantly between the groups. The common risk factors for BSI, independent of the infection source, were ICU LOS and MV duration. The predominant causative pathogens were K. pneumoniae, A. baumannii, and E. faecalis, with 87% of the cases being caused by MDR pathogens. Furthermore, all BSI cases were hospital-acquired (100%), with 59.4% of them being primary. The average time to the first positive blood culture was 11.4 days.
The occurrence of BSI did not significantly influence mortality, which may be attributed to prompt and appropriate interventions, including early detection and appropriate management. Prompt initiation of empirical antibiotics, followed by adjustment according to culture results, may help prevent adverse outcomes. Additionally, all patients in this study had severe COVID-19, which may have been the major determinant of mortality. Factors related to COVID-19 infection, including acute respiratory distress syndrome, systemic inflammatory response, and multi-organ failure, could have influenced the overall mortality regardless of the presence of BSIs. Additionally, other factors such as the presence of comorbidities, age, and other risk factors could play a more significant role in determining the mortality outcome than the presence of BSI. Furthermore, immune responses may significantly vary across individuals according to genetics, underlying health conditions, and other factors such as nutrition. Consistent with previous reports, 4 our findings demonstrate the significance of BSIs as adverse complications in ICU patients with COVID-19 since it extends the duration of hospital stay, increases healthcare costs, and increases the patient’s morbidity and mortality risk. 14 Previous studies have reported a prevalence rate of BSIs among ICU patients of 29.6%, 4 29.6%, 57%, 8 and 19.5%. 15
Consistent with previous reports, 16 we found that the BSI group had higher BMI values than the non-BMI group, implying a relationship between obesity and an elevated risk of BSI. The immune system can be compromised by obesity and related chronic inflammatory conditions, which increases the susceptibility to infections. 16
Our results revealed that the risk of BSI increased with longer ICU stay and extended MV duration, which is consistent with previous reports. 17 However, the COVID-19 pandemic has added another layer of complexity. Specifically, these extended durations could be a result of severe respiratory complications related to COVID-19, which further increase the risk of BSI. An extended ICU stay has been shown to increase the risk of nosocomial infections due to prolonged exposure to potential pathogens. 18
Notably, the use of corticosteroids was not a significant risk factor, which is consistent with a previous report.19,20 This may inform further research regarding the efficacy and safety of different treatment strategies for COVID-19, including the role of other medications such as tocilizumab or other drugs targeting cytokines, which modulate the immune response and may influence the risk of bacterial infections. Tocilizumab, which is an IL-6 receptor antagonist, reduces the severity of cytokine storms in patients with severe COVID-19. 21 However, these immunosuppressive effects increase the risk of bacterial infections. 21 Taken together, the widespread use of immunomodulatory drugs, MV, and intravascular catheters for treating patients with COVID-19 produces a conducive environment for the occurrence of BSI. 22
Our findings highlight the multifactorial etiology of BSIs among ICU patients with COVID-19, which is consistent with previous reports demonstrating the complex interplay between several factors in the development of secondary bacterial infections in ICU settings. 22 Additionally, the most frequently isolated pathogens were similar to those in previous reports, 23 which may inform potential targets for diagnostic and therapeutic interventions. Contrastingly, a high rate of co-infection with S. aureus has been reported in patients with flu. 24
Consistent with previous reports, 17 we observed a high prevalence of MDR pathogens (87%). Previous studies have cautioned against the overuse of antibiotics given the risk of multi-drug resistance, 25 which is consistent with our findings. However, the heightened antibiotic use during the COVID-19 pandemic for severe respiratory complications and co-infections may potentially worsen the MDR crisis. 26
These findings emphasize the need for effective infection control measures, antimicrobial stewardship, and early detection and management of BSIs in critically ill patients with COVID-19. Moreover, our findings regarding multi-drug resistance demonstrate the need for more stringent antibiotic stewardship in the ICU, especially during pandemics involving surges in antibiotic use. The variations observed in the risk factors for COVID-19 indicate the need for a more personalized approach to ICU care involving customized medication regimens and monitoring protocols. Additionally, our findings regarding the risk factors for BSI may inform clinical decision-making and management of these patients in ICU settings. Specifically, they demonstrate the need to optimize patient flow and reduce LOS, and thus the need for robust infection control strategies in ICUs.
Our study has several limitations, including its retrospective and single-center design, which introduces inherent biases and limitations associated with the use of existing medical records. Nonetheless, the large sample size and meticulous data collection strengthen the reliability of our conclusions.
Conclusion
Our investigation of critically ill COVID-19 patients in the ICU revealed a significant association between BSI and prolonged ICU stays and MV durations without impacting mortality. These findings underscore the need for heightened vigilance in monitoring BSI symptoms, an emphasis on antimicrobial stewardship given the rise of MDR pathogens, and a call for personalized care plans based on identified risk factors. Addressing these aspects can potentially enhance patient outcomes, reduce healthcare costs, and optimize ICU resource allocation amidst the ongoing pandemic challenges. Further prospective studies are warranted to validate our findings and elucidate the underlying mechanisms.