
Abstract
Background:
Cultural malpractices are socially shared perspectives and traditionally accepted behaviors experienced in a certain society that harm maternal health. In Ethiopia, about 18% of infant deaths occur due to cultural malpractice. However, evidence of cultural malpractice during the postnatal period is not well understood in Ethiopia, particularly in West Hararghe. Moreover, there is no study conducted on cultural practice during the postnatal period in this study area. Therefore, this aimed to assess the magnitude and factors associated with cultural malpractice among mothers attending postnatal care within 6 weeks after delivery at Gelemso General Hospital, Eastern Ethiopia.
Methods:
Institutional-based cross-sectional study design was conducted among 407 mothers attending postnatal care with their babies at Gelemso General Hospital. The study participants were selected by systematic random sampling technique. Data were collected using a pretested and structured interviewer-administered questionnaire. The collected data were entered into EpiData version 4.6 and exported to Statistical Package of Social Sciences version 27 for analysis. Descriptive statistics were computed to describe the characteristics of the participants. Bivariable and multivariable logistic regression analyses were fitted to identify factors associated with the outcome variable. Adjusted odds ratios along a 95% confidence interval were used to report the result and show the strength of the association. A P-value < .05 was used to declare a significant association. The results were presented using figures, tables, graphs, and text.
Results:
The study revealed that the magnitude of cultural malpractice during the postnatal period was 70.0% (95% CI: 65%, 74%). Lack of ANC visit (AOR = 3.3; 95% CI: 1.03, 10.27), partner’s being a farmer (AOR = 7.4; 95% CI: 2.11, 26.48), distance to health facility (AOR = 3.6; 95% CI: 1.68, 7.65), having greater than 5 alive children (AOR = 3.5; 95% CI: 1.25, 9.84) were factors significantly associated with cultural malpractice during the postnatal period.
Conclusions:
This study noted that more than two-thirds of participants committed cultural malpractice during the postnatal period. Therefore, emphasizing the importance of ANC follow-up, and encouraging home visits of postnatal mothers by professionals especially for those rural residents and remoter to health facilities may contribute to reducing the cultural malpractice.
Introduction
Cultural malpractices are defined as socially shared perspectives and traditionally accepted behaviors experienced in a certain society that harm maternal health. 1 The postpartum period is a very special phase in the life of a woman and baby. However, cultural practices and food taboos adversely affect the daily consumption of protein, energy, and some nutrients during the first month of nursing. 2 The practices are often implicated in determining the care received by mothers and babies during the postnatal period which is an important determinant of maternal deaths. 3 Cultural malpractices, with their numerous long-term devastating effects, are performed in all continents of the world even prevalence and degree may vary. 4
Globally, about 78 million newborns waited more than 1 hour to breastfeed, and 2 out of 5 newborns were excluded from colostrum feeding. 5 This means that every day, about 4000 infants and young children die due to colostrum avoidance and the introduction of pre-lacteal feds, which are part of cultural malpractice.5,6 Overall cultural malpractice during pregnancy, delivery, and the postnatal period killed 303 000 mothers and 2.7 million newborns each year. 7 The World Medicine Situation report estimates that between 70% and 95% of the population in developing countries and more than 80% of the population in Africa use cultural malpractice (CMP) during pregnancy. 8 Even if the WHO recommends exclusive breastfeeding for up to 6 months, 9 feeding practices happen early and colostrum discharging after delivery accounts for 4000 infant deaths every day in the world. 10 Confronting CMP unlike in the early 1990s only United Nations (UN) agencies and human rights groups began combating cultural malpractices, but the problem continued. 3
In many low-middle-income countries, the most common pre-lacteal foods given to infants can be divided into 3 categories: water only, water-based (rice water, herbal, juices), and milk-based (animal milk, infant formula). 11 Unclean tools are used to cut the umbilical cord during childbirth, and infection of omphaloi, a neonatal infection that starts in the umbilical cord is frequently found in developing nations and causes 520 000 neonatal deaths annually. 12 Delay in healthcare-seeking behavior due to (CMP) at home lead to uterine rupture, severe bleeding, fetal distress, and finally feto-maternal death. 1 Cultural malpractices are commonly practiced during different events and age groups, especially in females and their babies which include avoiding colostrum, feeding newborns, home delivery, food taboo, early marriage, marriage by abduction, giving “Koso” (herbal drug used for hookworm prevention), keeping babies out of the sun, son preference, unsafe abortion, usage of herbal drug, application of butter and cow dung on the umbilical cord are widely practiced with no or little attention to hygiene in Ethiopia. 4 Additionally, some studies have discovered that some religious components, such as religion and belief, untrained delivery attendants, and certain social and cultural factors, particularly in rural areas, are worsening the issue. 13
In Ethiopia, (CMP) the postnatal period accounts for about 18% of infant deaths. 10 The country has the highest maternal and infant mortality and morbidity rates in the world. 14 In 2020, there were 264 maternal deaths per 100 000 live births and 48 infant deaths per 1000 live births. 14 Ethiopia is a country with a famous and long-standing history with its own identity. It is also a country with many useful cultural practices that include breastfeeding, postnatal care, and social gatherings such as “caring for the aged person, children and religious leader”. 4 In contrast, (CMPs) are socially shared views and traditionally accepted behaviors experienced in a certain society that harm maternal health. 1 According to Ethiopian surveys, the magnitude of cultural malpractices during pregnancy and the postpartum period ranges between 37% and 85%. 15 In Ethiopia, cultural malpractices are pervasive among women and children. 15 Cultural practices and beliefs during pregnancy, childbirth, and the postnatal period have a significant impact on women’s healthcare-seeking behaviors. 15
To tackle the issues of CMP significant advancements have been made in terms of optimal breastfeeding promotion both within the facility and local communities. 16 In addition to the aforementioned, World Vision Ethiopia is currently implementing Counseling services on the Basic Health Service Package through Faith-Based Organizations, intending to contribute to the reduction of maternal and newborn morbidity and mortality by strengthening the Supportive Supervision and Primary Health Care Unit. 1 Furthermore, Ethiopia has created the National Infant and Young Child Feeding (IYCF) Guideline and recognized the benefits of the Baby Friendly Hospital Initiative (BFHI), which discourages pre-lacteal feeding practices on newborns to achieve optimal breastfeeding practices. 11 Ethiopia, on the other hand, is a country where (CMP) continues to wreak havoc on the health and social well-being of mothers and children. 10 Even if the cultural malpractices persist, they should be minimized by interventions like health education for mothers and their families about health service utilization. 17
In addition, during our literature searching there is a dearth of information and paucity of documented evidence regarding cultural malpractices during the postnatal period and associated factors toward babies whose mothers attending postnatal care both at the national level in general and in the study area in the particular. Therefore, this study aims to assess the magnitude of cultural malpractices during the postnatal period and associated factors toward babies whose mothers attending postnatal care at Gelemso Hospital, Eastern Ethiopia.
Methods and Materials
Study Area and Period
The study was conducted at Gelemso General Hospital, from December, 30, 2023 up to January 30, 2024. Gelemso Hospital is located in Habro Woreda, Gelemso town, West Hararge zone, in Oromia Region, Eastern Ethiopia. Gelemso Town is located 76 km from West Hararge Zonal town Chiro and 404 km East direction to Addis Ababa. The hospital has a catchment population of 1 149 106 and serve about 90 000 patients per year, 18 with 142 beds distributed in medical, pediatrics, surgical, gynecology, and obstetrics wards. Gelemso town is organized by 3 kebele. There is 1 hospital, 1 health center, and 11 private clinics in Gelemso town. Gelemso Hospital is a General Hospital that provides clinical services, laboratory services, and radiology services (X-ray and ultrasound services) for inpatient and outpatient attendances coming to the hospital. The hospital provides maternal and child health care for the people of the catchment area. The maternal and child health care units are run by an obstetrician/gynecologist and 23 midwives.
Study Population
All mothers attending postnatal care at Gelemso Hospital during the study period were source population whereas mothers who attended post-natal care within 6 weeks after delivery at Gelemso Hospital during the data collection period included in the study. Mothers who are critically ill or have psychiatric problems immediately after delivery were not included in the study.
Sample Size Determination
The sample size was determined by using the single population proportion with the following assumption: 41.5% of postnatal mothers experience Cultural malpractices throughout their postnatal period which is taken from a related study in Dire Dawa City, Eastern Ethiopia 19 are considered parameters to calculate the sample size. Then 10% of the possible non-response rate was taken into account.

Whereas n = minimum sample size required for the study, p = the estimated proportion of traditional malpractices during the postnatal period = (41.5%). Zα /2 = the cutoff value of standard normal distribution at 95% confidence level = 1.96, d = Margin of error = 5% (0.05).


Then by adding a 10% of non-response rate of 373, which is 37, the final sample size was =
Sampling Technique and Procedure
The systematic random sampling technique was used by considering the list of mothers attending postnatal care and immunization wards as a sampling frame. At Gelemso Hospital, on average, a total of 188 and 434 mothers visited the immunization ward and delivery ward respectively. This estimation was taken from the respective MCH clinic’s regular client registration for immunization and deliveries of the last 3 preceding months. Then proportional allocation was done for both wards. Kth interval was calculated using (K = 622/410 = 1.5 ~ 2). The first interviewed mother was selected by a lottery method from the number between 1 and Kth interval. Then the next mothers were selected at regular intervals every Kth individual until the required sample was obtained.
Data Collection Methods
A structured questionnaire was adapted and modified from relevant literature and similar studies.11,15,20-22 The questionnaire was prepared first in English, translated into the local language Afan Oromo to facilitate appropriateness and easy understanding by respondents, and then translated back into English by language experts to check its consistency. The questionnaire contains the socio-demographic characteristics of respondents, cultural-related factors, obstetrics-related factors, health care service utilization, and awareness-related questions. Two BSc midwives and 1 health officer were assigned as data collectors and supervisors respectively. Data collectors and supervisors were trained for 2 days on the overall objective of the study, the data collection process, ethical considerations, and how to facilitate and supervise the data collection process. Data collectors were supervised closely by the supervisor and the principal investigator daily.
Data were collected from mothers who were attending postnatal care within 6 weeks after delivery at Gelemso Hospital using an interviewer-administered pre-tested structured questionnaire. The women were interviewed at the postnatal unit after the discharge paper was written for them. The participants were interviewed in a private area after informed, voluntary written and signed consent was obtained from the study participants and head of hospitals. To protect the confidentiality of the information, names, and medical record numbers were not recorded on the questionnaire. The collected data were checked daily by the supervisor and PI to ensure the data collection process was being conducted as planned. Data collectors facilitated the data collection process by giving clarification and checking of completeness of the data.
Variables of the Study
Dependent variable: Cultural malpractice during the postnatal period
Independent Variables
Operational Definitions
Data Quality Controls
To maintain data quality we conducted a pretest before the actual data collection on 5% of the total sample size at Gelemso Health Center. Then the critical comments were incorporated into the final data collection tool to modify and increase its quality. Two days of training were given for data collectors and supervisors on the data collection tool and the data collection procedure. Data collectors were supervised closely by the supervisor and the principal investigators. The collected data were checked for completeness, accuracy, and consistency by the principal Investigator and supervisors daily. The supervisors and the principal investigators made frequent checks on the data collection process to ensure the completeness and consistency of the collected data.
Data Analysis
The collected data were checked for completeness, coded, entered using Epi-Data 4.6 version, and then exported to SPSS 27 for analysis. Descriptive statistics like simple frequency, mean and standard deviation were computed to describe a characteristic of the study participants. The results were then presented using frequencies, tables, and figures. The outcome variable was coded as “1” for malpractice whereas “0” for others.
Binary and multivariable logistic regression analysis was used to examine the association between independent variables and cultural malpractice. To control the effect of confounding factors, all variables with p-values less than 0.25 in Bivariable analysis were taken in the final model Multivariable analysis. To check the presence of multi-co-linearity, we run the VIF and Tolerance test. As a result, no variables with VIF >10 and tolerance test <0.1 were found. The Hosmer-Lemeshow and the Omnibus test were used to test the model’s goodness of fit. The model was declared to be a good fit since the result was found to be insignificant for the Hosmer-Lemeshow test (P = .21) but significant for the Omnibus test (P = .000). The strength and direction of statistical association were measured by an adjusted odds ratio with 95% CI. Lastly, in multivariable regression, available with a P-value ⩽ .05 will be declared as having a statistically significant association with the outcome variable.
Results
Socio-Demographic Characteristics
Of the total 410 sampled participants, 407 women from the postnatal and immunization ward participated in the study, yielding a response rate of 99.3%. The mean age of the respondents was 28.5 ± 5.7 with age ranges of 44 years. Three-fifth, 248(60.9%) of the study participants did not attend formal education, while only, 175(43%) of their partner were not attended formal education. Regarding occupational status, the majority, 320 (78.6%) of the participants were housewives and nearly half of them, 231(56.8%) had a household income of less than 2000 (Table 1).
Sociodemographic characteristics of mothers attending postnatal care within 6 weeks after delivery at Gelemso General Hospital, Gelemso Town, West Hararge Zone, Oromia, Eastern Ethiopia (n = 407).
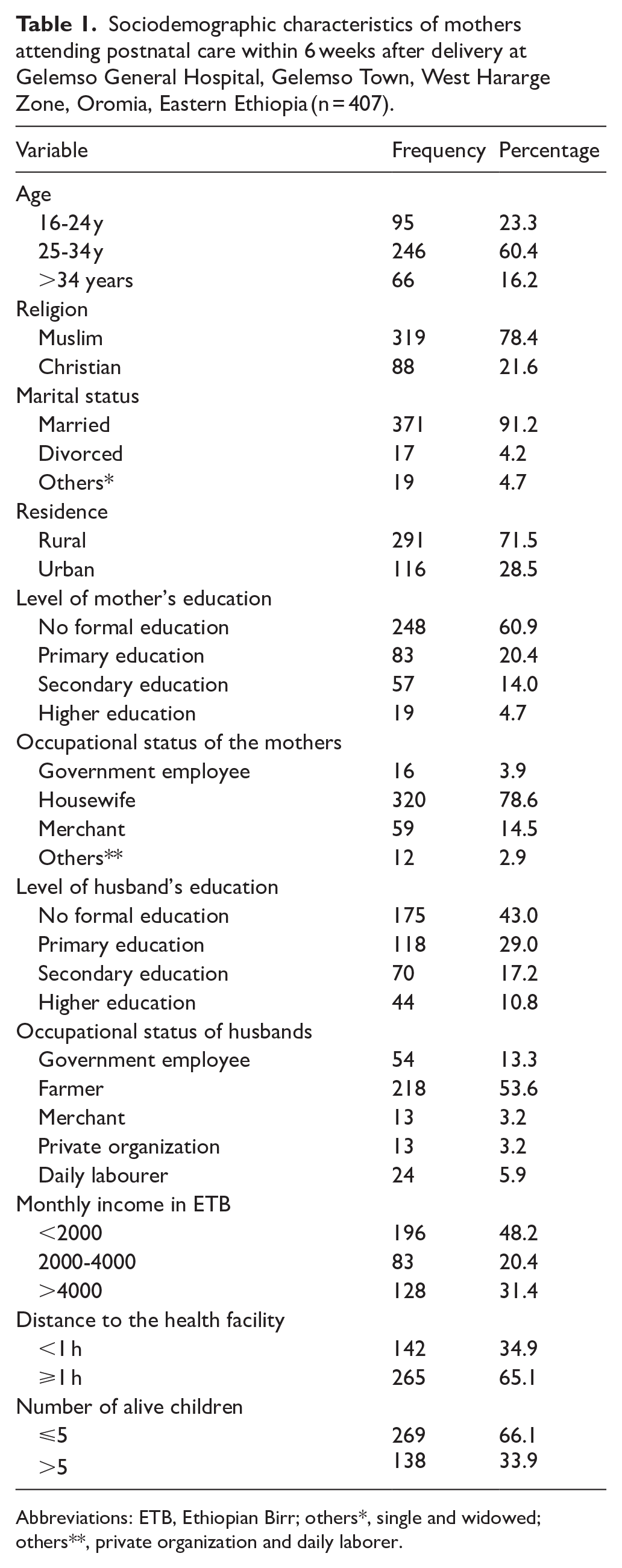
Abbreviations: ETB, Ethiopian Birr; others*, single and widowed; others**, private organization and daily laborer.
Obstetric and Gynecologic Characteristics of Study Participants
Of the total study participants, nearly two third, 266(65.4%) of participants were multipara, they had given birth 1 to 4 times. Nearly all, 398 (97.8%) of the respondents gave birth through spontaneous vaginal delivery. Regarding birth interval, more than half of the respondents, 232(57.0%) had given birth in less than 24 months. Of the total participants, nearly three-fourths, 294(72.2%) had ANC follow-up. Of those who had ANC follow-up, one-third, 94(33.7%) of the participants attended ANC 3 times or less, and only, 177 (60.2%) of them received counseling regarding CMP during their visits (Table 2).
Obstetric-related characteristics of mothers attending postnatal care within 6 weeks after delivery at Gelemso General Hospital, Gelemso Town, West Hararge Zone, Oromia, Eastern Ethiopia (n = 407).

Abbreviations: ANC, antenatal care; CMP, cultural malpractice; C/S, cesarean section; SVD, spontaneous vaginal delivery.
Types and Reasons for Engaging in Cultural Malpractice
Of the total participants, nearly half of the respondents, 187(45.9%) did not expose their newborns to sunlight and more than half of them, 111(59.4%) mentioned the fear of evil spirits as a common reason for not exposing. Two hundred fifty-nine (63.6%) of respondents bathed their neonates in less than 24 hours. Slightly more than two-thirds, 276 (67.8%) of respondent put substances on the stump of their newborns. The most common substance mentioned to be put on the umbilicus cord was butter (69.2%). Slightly more than three-fifths, 259(63.6%) of respondents gave liquids other than breast milk to a child before the mother’s colostrum was given. The majority of them, 259(93.8%) reported that putting a substance on the umbilical cord prevents stump infection (Table 3).
Information related to Cultural malpractice of mothers attending postnatal care within 6 weeks after delivery at Gelemso General Hospital, Gelemso Town, West Hararge Zone, Oromia, Eastern Ethiopia (n = 407).

Magnitude of Cultural Malpractice During the Postnatal Period
In this study, of the total study participants, 285(70.0%; 95% CI: 65.3, 74.4) respondents committed at least 1 type of cultural malpractice during the postnatal period. The most common reasons mentioned for practicing cultural malpractice were the prevention of stump infection, the prevention of abdominal cramps, and fear of evil spirits (Figure 1).

Magnitude of cultural malpractice among mothers attending postnatal care within 6 weeks after delivery at Gelemso General Hospital, West Hararge Zone, Eastern Ethiopia (n = 407).
Factors Associated With Cultural Malpractice
In Bivariable logistic regression, 11 variables were associated with the outcome variable at p value less than 0.2. These variables were maternal age, residence, maternal education, maternal occupation, maternal occupation, monthly income, parity, ANC, distance to health facility, number of alive children, and the type of profession who attended the delivery. However, in the final model of multivariable logistic regression analysis, predictor variables like paternal occupation, ANC, distance to health center, and number of alive children were independently associated with cultural malpractice.
Accordingly, women whose husbands’ occupations were farmers were 7 times (AOR = 7.41; 95% CI: 2.11, 26.48) more likely to be involved in cultural malpractice than women whose husband was Government employee. Likewise, the odds of participating in cultural malpractice were 3 times (AOR = 3.25; 95% CI: 1.03, 10.27) higher among women who lack ANC follow-up as compared to their counterparts. Furthermore, women who traveled ⩾1 hour to reach the health facility were 3.6 times (AOR = 3.58; 95% CI: 1.68, 7.65) more likely to participate in cultural malpractice compared to those who traveled <1 hour. Finally, the likelihood of participating in cultural malpractice among mothers who had ⩾5 alive children was 3.5 times (AOR = 3.5; 95% CI: 1.25, 9.84) higher than mothers who had <5 alive children (Table 4).
Bi-variable and multivariable logistic regression analyses of factors associated with Cultural malpractice among mothers attending postnatal care within 6 weeks after delivery at Gelemso General Hospital, West Hararge Zone, Eastern Ethiopia (n = 407).

Significant with P-value < .05; **Significant with P-value < .001: Others*, private org and daily Laborer and TBA, traditional birth attendant.
Discussion
This study showed that 70% of women practiced cultural malpractice in Gelemso town during their post-natal period. Putting substances on the umbilical cord, bathing newborns in less than 24 hr, and applying leaf of pepper were the most commonly mentioned cultural malpractices during the postnatal period. Multivariable logistic regression results showed that not having an ANC visit, Husband’s occupation being a farmer, distance to the health facility, and having more than 5 alive children were significantly associated with cultural malpractice.
The proportion of malpractice during postnatal in the present study was similar to the studies carried out in southwest Ethiopia 72.6%. 26 But, the present finding is higher than the study conducted in Dire Dawa City (41.5%), 7 northwest Ethiopia (21.6%), 27 and Gozamen District Ethiopia (31.5%), 28 while the finding of this study was lower than the study conducted in Meshet Town Northwest Ethiopia (76.1%), 3 and India 97.5%. 29 This discrepancy could be justified by the fact that there was a variation in the tool used to measure malpractice between the studies. The other possible explanation for the discrepancy is the place where the studies were conducted. For example, the present study was conducted at a health facility while the rest were conducted at the community level.3,26,28 Variations in sample size, study population, and study time also may contribute to the differences in an estimation of cultural malpractice. Geographical variation of cultural sensitivity among health professionals when evaluating a woman’s clinical health during prenatal care visits, childbirth, and postpartum visits might also brought the discrepancy.
In this study, the occupational status of the husband being a farmer is significantly associated with committing cultural malpractice during postpartum. This finding is consistent with studies conducted in Loma Woreda, Southwest Ethiopia,15,26 and Northern Karnataka India. 30 The systematic review conducted in Ethiopia 31 also supports this finding which states that Rural-dwelling community were more likely to participate in cultural malpractice after giving birth. A possible explanation could be the fact that in the Ethiopian context, the majority of farmers are rural residents and not educated. As a result, they my lack information about the harmfulness of CMP and encourage the family to experience it. In addition, community who live in rural areas lack access to information which disseminated through media outlet that could help them to make decisions about healthy behaviors, such as promotion and education of maternal and child health. 1
In the present study, we found a strong association between Lack of ANC follow-up and cultural malpractice. This finding is supported by previous studies conducted in Northwest Ethiopia,1,15,31 and Ghana, 32 which reported women who did not have ANC follow-up up more likely to engage in malpractice. This may be explained by the fact that women who have received ANC services at a health facility are likely aware of the dangers and complications associated with CMP. 31 Nevertheless, this outcome did not align with a study conducted in Turkey. 33 This discrepancy may result from variations in the infrastructure of health services’ accessibility and availability.
The odds of committing cultural malpractice during postnatal were significantly higher among mothers who had 5 or more live children compared to their counterparts. This finding is in line with studies conducted in Eastern and Northwest Ethiopia,7,27 Nepal, 34 and Turkiye. 33 This could be explained due to social norms and values which probably make them continue their practice because of misconceptions about traditional malpractice from previous delivery experiences. 26
The odds of committing cultural malpractice among mothers who traveled more than 1 hour to reach the health facility were higher than mothers who traveled less than 1 hrs to reach the health facility. This result is in line with a systematic review conducted by Meseke and his colleagues, 35 in which they stressed travel time and distance are crucial factors for people living in rural and remote areas to access health services. A scoping review from Ethiopia also states that people from remote communities found it difficult to get to health facilities. 36 This could be explained by the fact that care-seeking behavior is structurally impeded by the distance to a healthcare facility due to great distances and lack of transportation, particularly ambulances. 37
Strength and Limitation
This study used primary data that may reduce the number of missing important factors. The study also attempted to identify important factors of cultural malpractice during the postnatal period. This study is not without some limitations, since we used self-reporting (interview response) to collect the data which may lead to recall bias. The study was not generalizable to the whole population of the catchment area, since the study was restricted to health facilities, the mothers who had no postnatal visits were not addressed by the study. Additionally, the study were also excluded mothers who had critical illness and psychiatric problem which might limit the representativeness of the finding.
Conclusion and Recommendation
This study noted that more than two-thirds of participants committed cultural malpractice during the postnatal period. Being a farmer, Lack of ANC follow-up, having more than 5 alive children, and distance to health facilities were significantly associated with engaging in cultural malpractice during the postnatal period. Therefore, emphasizing the importance of ANC follow-up, and encouraging home visits of postnatal mothers by profession especially for those rural residents and remoter to health facilities may contribute to reducing the cultural malpractice. In addition Woreda Health Bureau should work with the concerned stakeholders on comprehensive intervention strategies to strengthen ANC follow-up and better to emphasize on community education to alleviate misconceptions about traditional malpractice. Furthermore, healthcare providers should work in collaboration with health extension workers to provide education to women on the impact of cultural malpractice and its consequences. Finally, further investigations employing different approaches and community based study will recommended for future researchers.
Footnotes
Acknowledgements
We would like to express our deepest gratitude to Haramaya University, College of Health and Medical Sciences. We also want to thank data collectors, supervisors, study participants, and all others who directly or indirectly supported this work.
Ethical Considerations
Ethical approval was obtained from the Institutional Health Research Ethics Review Committee (IHRERC) of the College of Health and Medical Sciences of Haramaya University (Ref. No. IHRERC/256/2023). An official letter was also secured for Gelemso Hospital. Before conducting the study, informed, voluntarily, written and signed consent was obtained from the study participants and head of Gelemso Hospital. Respondents were informed that they had the right to refuse or withdraw from the study at any time if they so desired. Participants were also informed about the attainment of confidentiality of the information they provided.
Author Contributions
JS, DA, AD, TB, and EY had made a substantial contribution to the conception/design of the research idea, JS, DA, AD, and TB proposal development, JS, DA, AD, EY, NB, RYI, BG and TB were participated in the analysis, interpretation of the data. Manuscript draft and write-up were done by EY, NB, RYI, BG, and TB. Then JS, EY, NB, RYI, BG, and TB revised the paper critically and added their intellectual content. All authors have read and approved the final manuscript for publication.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data for this study is available online within the manuscript.