
Abstract
Healthcare workers frequently experience emotional distress from repeated exposure to patient death, yet professional grief remains poorly recognized and inadequately supported. The COVID-19 pandemic further magnified these challenges, bringing professional grief into sharper focus. The purpose of this scoping review was to comprehensively examine professional grief among healthcare workers (HCWs) across different professions and specialties, map existing literature, identify research gaps, and provide educational, clinical, and policy recommendations. This scoping review followed Arksey and O’Malley’s methodological framework and PRISMA-ScR guidelines. Databases searched included PubMed, CINAHL, and PsycINFO for literature from 2004 to 2024. Studies were screened based on inclusion criteria focusing on professional grief experiences of HCWs dealing with patient deaths. Qualitative, quantitative, and mixed-method studies were included. Eighty-one publications were reviewed, with most studies published since 2020, highlighting increased attention post-COVID-19. Key findings identified significant individual (eg, early career vulnerability, lack of formal education), interpersonal (eg, patient demographics, relationship quality), and systemic factors (eg, emotional suppression culture, workload constraints) influencing professional grief. Existing interventions were predominantly peer-based and lacked demonstrated efficacy in reducing grief intensity. Measurement inconsistencies revealed discrepancies between qualitative and quantitative assessments of grief intensity, indicating a need for specialized measurement tools tailored to professional contexts. Professional grief among HCWs is multifaceted and deeply influenced by cultural, educational, and systemic barriers. Comprehensive strategies addressing these barriers must include structured educational curricula, ongoing clinical support programs, validated grief measurement tools, and institutional policies promoting open emotional expression. These approaches are essential to fostering resilience, enhancing professional well-being, and improving patient care outcomes.
Keywords
Introduction
Healthcare workers (HCWs) are facing a mental health crisis in the United States, which was intensified by the COVID-19 pandemic. 1 A recent study showed an increase in mentally unhealthy days between 2018 and 2022 (3.3 in the past 30 days vs 4.5 days). 1 HCWs face occupational exposures such as infectious diseases (including bloodborne illnesses), chemicals, ergonomic hazards, and workplace violence. 2 While these occupational hazards are well-recognized, exposure to psychologically straining situations like suffering, death, and dying have not been characterized as workplace exposures. 2 Even though there may be significant impacts of these experiences, including grief, compassion fatigue, diminished psychological and physical health, and healthcare workforce stability. 3 Furthermore, patient outcomes are impacted by both workforce turnover and HCWs whose grief has gone unacknowledged and/or unaddressed.4-6
Grief is considered a universal human experience and an expected reaction to loss. 7 For HCWs, grief may be experienced not only due to the loss of a patient but also due to observing suffering and losses related to illness. While the relationships between healthcare workers and patients are often time-limited, the emotional connection created when caring for someone in their extremity may relate to the depth of a worker’s grief. 7 In addition, the cumulative losses HCWs witness and experience, and the subjective experiences related to these losses may intensify grief.3,8 Grief is not an inherently negative experience and can potentially produce positive outcomes such as increased meaning and purpose, deeper connections with others, and post-traumatic growth.3,9
Papadatou first proposed the Model of Health Professionals’ Grieving Process in 2000, based on her extensive work as a clinical psychologist and research with oncology and critical care nurses coping with the death of children. The model pulls theoretical influence from the Dual Process Model of Coping and Bereavement 10 and conceptualizes HCWs reactions to cumulative patient deaths. Unlike traditional bereavement models that focus on the grief experienced with the loss of a loved one, Papadatou’s model specifically addresses professional grief, which differs from personal grief as it is anticipated daily, and a result of the job chosen by the HCWs. Because the professional’s first responsibility is to attend to workplace demands, professional grief is often hidden in “private shadows” and not openly expressed. 11
What makes professional grief so challenging for HCWs is that they not only accept it as part of the job, but they also return to work where they are likely to face loss again and again. 11 Without space or time to address grief in response to these losses, healthcare workers are at risk of experiencing complicated grief, 12 which is persistent grief that impacts daily life and relationships.12,13 In addition, HCWs may navigate feelings of guilt, anger, or despair, report feeling isolated due to their grief, be forced to confront their mortality, and have to balance their grief with ongoing work demands. Finally, HCWs’ ongoing exposure to grief and loss may lead to compassion fatigue. There are serious occupational and health consequences related to compassion fatigue including emotional blunting, increased work absenteeism or presenteeism, leaving the workforce, depression, anxiety, post-traumatic stress disorder (PTSD), insomnia, and poor physical health.3,4,7,8,14-16
Previous literature reviews have explored grief among HCWs. However, ours is the first to comprehensively examine professional grief across all healthcare professions and specialties, incorporating quantitative, qualitative, and mixed-method designs. While Yazdan et al 17 reviewed 29 articles on hospital-based interventions to address physician and nurse grief, highlighting the limited and heterogenous nature of existing studies, and Burm et al 18 reviewed 173 studies on physician and nurses’ experiences during the COVID-19, emphasizing the need for institutional support, these reviews were profession- or context-specific. Other reviews have also been limited in scope: Tamworth et al 19 examined grief among mental health practitioners, Findlay and Robertson 20 focused on home care workers, and Weiss et al 21 explored disenfranchised grief (a type of grief that is not openly acknowledged, mourned, or supported by others 22 ) within a nursing paradigm, while Fernández-Basanta et al 23 conducted a meta-synthesis on midwives’ and nurses’ grief related to pregnancy loss. In contrast, our review provides a holistic and cross-disciplinary perspective on professional grief, offering a broader understanding of how grief manifests and is managed across diverse healthcare roles.
The purpose of the current study was to (1) conduct a 20-year scoping review of studies on professional grief across healthcare disciplines and specialties; (2) map the field of study on professional grief in healthcare and identify gaps in the existing literature; and (3) provide recommendations that will inform future research, theory, education, and clinical practice.
Methods
We conducted a scoping review, which is a systematic literature review that is particularly useful for exploring the breadth of literature on a complex and diverse topic. 24 This methodology is appropriate for addressing our broad research question. Our review followed the Arksey and O’Malley 25 framework, which outlines five key stages: identifying the research question, identifying relevant studies, study selection, charting the data, and collating, summarizing, and reporting the results. Additionally, we adhered to the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews) protocol. 26 The PRISMA-ScR checklist is provided in Supplemental Additional File 1. A protocol was registered on March 8, 2025 with the Open Science Framework (doi:10.17605/OSF.IO/JYPUZ). 27
Stage 1. Identifying the Research Question
Our scoping review aims to answer the following research question: What is known about professional grief across healthcare professions and specialties?
Stage 2. Identifying Relevant Studies
On January 5, 2022, we searched PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL) Plus with Full Text, and PsycINFO by titles and abstracts using the following sets of search terms: “disenfranchised grief,” “professional grief,” and “healthcare professional grief.” We also used combinations of “grief” and different professions (ie, “nurse,” “doctor,” “social worker,” “chaplain,” and “medical assistant”) as additional search terms. CINAHL and PsycINFO were searched using EBSCOHost. The detailed search strategy is provided in Supplemental Additional File 2. We selected these three databases based on their comprehensive coverage of relevant, peer-reviewed literature on the topic. While additional databases could expand coverage, we were focused on publications in the health care field and the combination chosen provided a robust balance between comprehensiveness and practical feasibility. On December 6, 2024, we updated the search by using the same search terms in the same three databases. A 20-year date range of 2004 to 2024 was imposed on the search. All identified publications were combined, and duplicate publications were excluded using Covidence, 28 a web-based screening tool.
Stage 3. Study Selection
Next, the nonduplicate publications were screened by title and abstract using predetermined inclusion and exclusion criteria. Publications were divided among the five reviewers (CP, KT, DR, AV, SG), each reviewed independently by two reviewers, and any ambiguous publications were reviewed as a team to reach a consensus. The inclusion criteria for this scoping review were: (1) full text written in English, (2) focus on healthcare professionals (eg, doctors, nurses, social workers, chaplains, medical assistants), (3) primary outcome of professional or disenfranchised grief, and (4) examines the emotional experiences of HCWs coping with patient death and/or working in high-death contexts (eg, oncology, palliative care, hospice, and frontline roles during COVID-19). We defined HCWs as members of the healthcare team who play a vital role in the holistic care of patients, including addressing their spiritual and emotional needs.29,30 Furthermore, our inclusion criteria included HCWs routinely involved in end-of-life situations—settings in which professional grief is most likely to arise. No limitations were placed on study design—qualitative, quantitative, and mixed methods designs were included. Publications were excluded if they (1) did not provide peer-reviewed empirical data (eg, letters, commentaries, editorials, dissertations, conference abstracts, case studies, systematic reviews, or book chapters) or (2) only discussed family or informal caregiver grief (ie, no HCWs grief). Grey literature was excluded due to our focus on peer-reviewed studies, considerations regarding methodological rigor, and to reduce bias. 31 The remaining publications were screened by full text using the same inclusion and exclusion criteria.
Stage 4. Charting the Data
All studies that met eligibility criteria were extracted and compiled in Supplemental Additional File 2, which includes the authors, year, country, purpose, methodology, demographics, and findings.
Stage 5. Collating, Summarizing, and Reporting the Results
A descriptive analysis of the included studies was conducted to summarize the key characteristics of the research, including study design, sample characteristics, and primary findings. Quantitative data were synthesized using narrative synthesis, a well-established approach for integrating findings across heterogeneous studies. 32 This method facilitated a comprehensive understanding of professional grief across healthcare disciplines and specialties while identifying methodological trends and gaps in the existing literature. Qualitative study findings were analyzed using Braun and Clarke’s 33 thematic analysis process. Two reviewers (CP, KT) independently familiarized themselves with the qualitative data, reading and re-reading the findings to identify preliminary patterns and ideas. They then independently generated initial codes across the data set, marking segments of data relevant to the research question. Reliability was enhanced through regular meetings to compare interpretations, resolve discrepancies, and reach concensus on code definitions. Following initial coding, themes were developed by clustering similar codes into broader patterns. These themes were collaboratively reviewed and refined to ensure accuracy and comprehensiveness. To further enhance rigor, themes were continually cross-checked against the original data. No software was used during the analysis; all coding and theme development were conducted manually.
Results
Search and Screening
During stage 2, a total of 1,138 publications were identified. After removing 291 duplicates, 847 publications remained for title and abstract screening. During the screening of publications by title and abstract, a total of 655 publications were excluded. The remaining publications were sought for retrieval; however, two studies were not retrieved. A total of 190 publications proceeded to full-text screening. During the final phase of screening, 109 publications were excluded, for a total of 81 publications included in this scoping review. Figure 1 presents the full search and screening process.

PRISMA flow diagram.
Descriptive Characteristics of Included Publications
The included 81 publications represent 80 unique studies and samples; 2 publications reported data from the sample study—one qualitative and the other quantitative findings from their intervention.34,35 A summary of the 81 publications is presented in Supplemental Additional File 2. The studies were published between 2004 and 2024, with the majority (46/80; 58%) published since 2020, demonstrating a growing interest in this area of research. Ten studies were explicitly published in response to the COVID-19 pandemic. In total, the studies were conducted in 26 countries across North America, South America, Europe, Asia, Africa, and Oceania, with the largest proportion (28/80; 35%) published in the United States. Qualitative designs were most common (47/80; 59%); the remaining studies used cross-sectional (22/80; 28%), quasi-experimental (7/80; 9%), or mixed-methods (4/80; 5%) designs. Most of the included studies (46/80; 58%) did not mention a guiding philosophical or theoretical framework. Several theories were used, with Stroebe and Schut’s 10 dual process model of coping with bereavement,34,36,37 Doka’s 38 concept of disenfranchised grief,39-41 and Papadatou’s 11 model of health professionals’ grieving process14,42 referenced the most frequently. Additionally, 10 of the qualitative studies adopted a phenomenological approach43-52 and 10 used a grounded theory method.14,53-61
Sample sizes across the studies ranged from 6 to 794, with an average of 87 HCWs per study. Most studies (47/80; 59%) had fewer than 50 participants. The largest proportion of studies focused on oncology (15/80; 19%), obstetrics and neonatal intensive care units (12/80; 15%), and pediatrics (12/80; 15%). Other specialties included inpatient and outpatient mental health (7/80; 9%), home health or long-term care facilities (7/80; 9%), palliative care or hospice (6/80; 8%), intensive care units (5/80; 6%), emergency medicine (1/80; 1%), podiatry (1/80; 1%), anesthesiology (1/80; 1%), and mixed acute care settings (12/80; 15%). One study did not specify specialty. 62 Regarding professions, nurses were the most frequently studied group (33/80; 41%), followed by physicians (10/80; 13%), healthcare aides (6/80; 8%), nurse midwives or obstetricians (4/80; 5%), and social workers (4/80; 5%). The remaining 17 studies included a diverse range of professionals, with nurses and physicians appearing in nearly all samples. Other professions represented included advanced practice registered nurses, psychologists, respiratory therapists, chaplains, and paramedics. Further details on study samples are available in Table 1.
Study characteristics.

Abbreviations: APRN, advanced practice registered nurse; CNA, certified nurse aide; HCWs, healthcare workers; HHA, home health aide; ICU, intensive care unit; LPN, licensed practical nurse; LTC, long-term care; PICU, pediatric intensive care unit.
Qualitative Findings
In this scoping literature review, we explored professional grief across healthcare disciplines and specialties. Our analysis identified key themes across individual, patient, and systemic factors, as well as coping strategies and the impact of patient death on HCWs. Finally, a sub-analysis of findings related to the COVID-19 pandemic are provided.
Individual Factors
Early Career Challenges
HCWs reported experiencing more difficulty in the early stages of their careers when confronted with patient death and that it becomes easier with more experience.37,48,50,56,57,61,63-68
Lack of Education on Coping with Work-Related Emotions
Many HCWs feel unprepared to manage professional grief, particularly due to a lack of formal education on bereavement, grief processing, self-care, and communication with dying patients and their families.35,37,39,43,46,47,50,52,55,58,64,65,67-72 While on-the-job experience helps professionals learn to compartmentalize and set emotional boundaries, cope, and become more comfortable with difficult conversations,37,46,56,61,65,66,73 many desired more structured education on palliative care, self-care strategies, and interpersonal skills related to end-of-life care.35,39,43,46,52,56,67,69-71,74,75
Personal Loss and Identification with Patients and Family
HCWs frequently experience stronger emotional responses when a patient or family member reminds them of themselves or their own loved ones.37,46,49,54,58,59,63,65,66,70,73-80 This identification can enhance empathy and improve patient care but also intensifies the grief response. Those with prior loss histories may find patient deaths especially triggering, while others develop coping strategies and bereavement skills informed by their past grief experiences.37,43,46,52,59,65,66,74
Patient Factors
Patient Characteristics and Length of Relationship
Outside of pediatrics and the neonatal intensive care units, deaths of younger patients, pregnant individuals, and parents of young children are often described as particularly distressing, versus the death of older adults which is seen as natural.37,39,48,49,52,58,59,63,66,76,81-83 More intimate patient-care relationships foster stronger therapeutic bonds, which are beneficial for patient-centered care but can make death more emotionally challenging for HCWs.39,44,47-49,52,54,55,58,59,61,63-66,71,74,75,78,80-88
Expectation and Prognosis of Death
Unexpected and sudden deaths, particularly in general wards, community settings, and cases involving COVID-19, are especially difficult for HCWs.14,43,46,48,49,54,56,58,59,61,63,67,69,73,76,78,80,82,83,85,86 Unlike chronic patients, such as in the ICU 48 or pediatric oncology, 61 where there is time to process the prognosis and engage in anticipatory grieving, the sudden decline in a patient can be particularly distressing. 67 These situations may also lead to heightened feelings of guilt and self-doubt among healthcare workers, as they question whether they did everything possible to prevent the outcome. 86
Good Death Versus Bad Death
HCWs report that a “good death”—one in which suffering is minimized, patient wishes are fulfilled, unnecessary treatments are avoided, and occur in a home-like environment—provides emotional relief and a sense of meaning for HCWs.37,39,48,52,61,70,71,74,75,80,84 Conversely, “bad deaths,” characterized by prolonged suffering with no effective interventions to offer, often lead to feelings of guilt, powerlessness, and emotional burden.14,46,48,55,58,59,61,63,68,73,75-77,80,82,84,85,88 Managing family grief is an additional emotional burden for HCWs. Conflicts within families and difficulty accepting a prognosis are associated with a “bad death” and can complicate the professional’s experience of loss.37,58,59,72,75,82,83
System Factors
Culture of Healthcare and Stigma Around Grief
The healthcare environment often discourages open expressions of grief, reinforcing a culture of emotional suppression.35,37,39,47,49,51,52,58,63-66,69,70,72,76,80,81,84,86,88 Grief expression, counseling, and debriefing are sometimes viewed as a weakness or lack of professionalism and inexperience,52,58,63,66,87 particularly in maternity settings where professionals fear blame and litigation.43,69 Different healthcare professions believe other professions are better at processing and coping with patient death. Physicians often feel pressured to appear strong and believe it is more acceptable for nurses and midwives to express grief.43,69,76 In contrast, nurses express a desire for a closer emotional connection with physicians, hoping for mutual support.43,68 In palliative care, grief is more openly acknowledged and supported, but the work remains emotionally challenging.35,63 Therapists believe their profession is more challenging because they are trained to display empathy, while physicians can focus more on the clinical aspects of care. 60
Professionals must balance the expectation to remain composed and professional (repress grief) with the need to show compassion and build therapeutic relationships (express grief).37,39,49,56,57,60,61,63-65,70,72,73,81,84,87 Neonatal Intensive Care Unit (NICU) and pediatric HCWs often feel they lack the “right” to grieve since the deceased was not their child.61,87 There is also uncertainty around funeral attendance, with concerns about colleague judgment, appropriateness, and whether the family would appreciate it.54,74,79,81,87 Gender norms, with male professionals more likely to compartmentalize their emotions, were only mentioned in one study. 58
Lack of Time and Space to Grieve
HCWs often report that heavy workloads, understaffing, and the pressure to quickly transition to the next patient hinder their ability to process grief, leading to emotional strain.14,35,37,45,46,50,52,55,63,64,66,68,70,73,74,80,82,84-86 Additionally, a high volume of patient deaths can intensify emotional exhaustion.14,61,82,89,90 Participants express a desire for more time and space to engage in rituals and properly process their grief, as they feel they don’t have enough time to fully grieve or honor and respect the deceased patient.37,63,66,80,84
Coping Strategies
Formal Support
Many professionals report a lack of formal institutional support for grief processing, representing a disconnect between those on the frontline and those in administrative and management roles.35,39,43,47,54,57,64,69,70,74-76,80,86-88,90 Desired resources include paid time off from work following difficult deaths,39,55,74,86 designated time and space to grieve at work,63,64,66,80,86 structured debriefings and support groups,35,43,46,52,56,57,65,67,70,74,75,86 and professional grief counseling.39,60,75,86 Unlike other professions, healthcare aides experienced additional financial stress related to patient deaths and coping. Home health aides, whose jobs are directly tied to their clients, face job insecurity when a client dies, making it difficult to take time off for their own wellbeing due to financial consequences. 39 Other aides reported financial strain from attending memorial services, as this time is unpaid, 86 and others reported not being able to take time off without it affecting their salary or vacation time. 74 When formal support systems do exist, they are largely unsuccessful because they either occur too late, 87 occur once (vs ongoing support),46,70 lack structure or clear policies on when and how they should occur,70,87 occur off-the-clock,39,78,87 focus on clinical outcomes rather than emotional impact, 70 or are led by an outsider. 80 In psychiatry and community health settings, providers desire a better system for notifying staff of a patient’s death.54,86
Informal Support
Colleagues provide the most meaningful support, particularly colleagues from the same unit where shared experiences foster understanding.37,39,43,46-51,53-57,61,63-68,70,73,74,76,77,80,81,83,86-89 Compared to formal support like professional counseling or support groups, some professionals reported that they prefer talking with colleagues during their shift because they do not want to bring work home and feel less inhibited when sharing with peers.37,48 Nurse participants voiced the importance to support younger nurses.56,65,68,70 Support from family and friends was also commonly discussed.35,39,46,47,50,51,53,54,65,77,80,83 However, compared to support from colleagues, family and friends are often less helpful due to a lack of understanding of the nature of professional grief and need to protect them from harsh reality of their work.39,46,61,65,68,87
Personal Self-Care and Finding Meaning
Many HCWs use self-care strategies, such as spirituality, outdoor activities, spending time with pets, or relaxing through massages, baths, reading, or music, to process grief.37,39,44-46,49,51-53,55,60,64,67,70-73,76,78,80,83,91,92 Some also find comfort and closure in remembering deceased patients through personal rituals.35,70,81,87 Additionally, qualities like inner strength, resilience, mindfulness, a positive attitude, and maintaining boundaries are seen as beneficial to grief management.39,44,63,64,68,78 HCWs often find meaning in their experiences by rationalizing the situation, using destiny-based explanations, believing they have fulfilled their caregiving responsibilities, or viewing their profession as a calling, with grief viewed as part of their professional responsiblity.37,39,45,47,50,54,57,61,63-65,70,73,76-78,89-91,93
Emotional Avoidance
Some HCWs cope by suppressing or compartmentalizing their emotions.35,37,39,44,48-50,53,55,56,60,61,63,65,67,72-81,83,84,86-88 While this may help them fulfill their duties and maintain a task-oriented approach to patient care (versus whole person-oriented),37,52,53,61,63,72,79-81,83 it can have negative long-term effects due to not adequately processing grief, including loss of empathy37,50,77,81,84 and emotional shutdown both professionally and personally.50,55,60,63,74,81 Additionally, some HCWs engage in other forms of maladaptive coping, such as alcohol consumption or binge eating.35,37,46,52,53
Impact of Death on Healthcare Professionals
Awareness of Mortality
Caring for dying patients often increases healthcare professionals’ awareness of their own mortality and prompts them to prepare and reflect on their personal priorities.37,44,48-51,55,57,61,64,65,67,68,79,91,92
Psychological and Physical Impact
Grieving professionals often experience feelings of loneliness, stress, and burnout, along with sleep disturbances, increased blood pressure, chest pain, fatigue, anger, intrusive flashbacks, depression, and negative impacts on their personal relationships due to unprocessed grief.35,39,43,44,48,51-53,56,59,61,64-66,71,81,83,87,92 Some providers consider leaving or leave the profession partly due to professional grief,60,61,64,79 while others become hypervigilant in their practice or peruse higher education to provider better quality care.50,64,79,81 HCWs often feel responsible for a patient’s death, reflecting on what they could have done differently and reviewing whether everything was done correctly.39,43,49,51,52,54,58,59,61,63,66,67,69,72,76,81,83,85-87,90 For many, self-doubt and guilt become more overwhelming than the grief itself. In some cases, such as abortions 72 or the removal of ventilators, 67 spiritual guilt is tied to the patient deaths.
Impact of COVID-19 on Professional Grief
The COVID-19 pandemic exacerbated professional grief in several ways. Many deaths occurred in isolation, depriving patients and families of meaningful goodbyes and leaving HCWs feeling powerless and guilty.14,77,93 The responsibility of triaging limited resources, such as ventilators, placed immense ethical burdens on professionals, and providing substandard care.77,89,93 A lack of preparation and constantly changing guidelines contributed to emotional fatigue.14,53,93 Social support systems weakened as professionals worked remotely or in isolation.89,93
Quantitative Findings
Grief Instruments
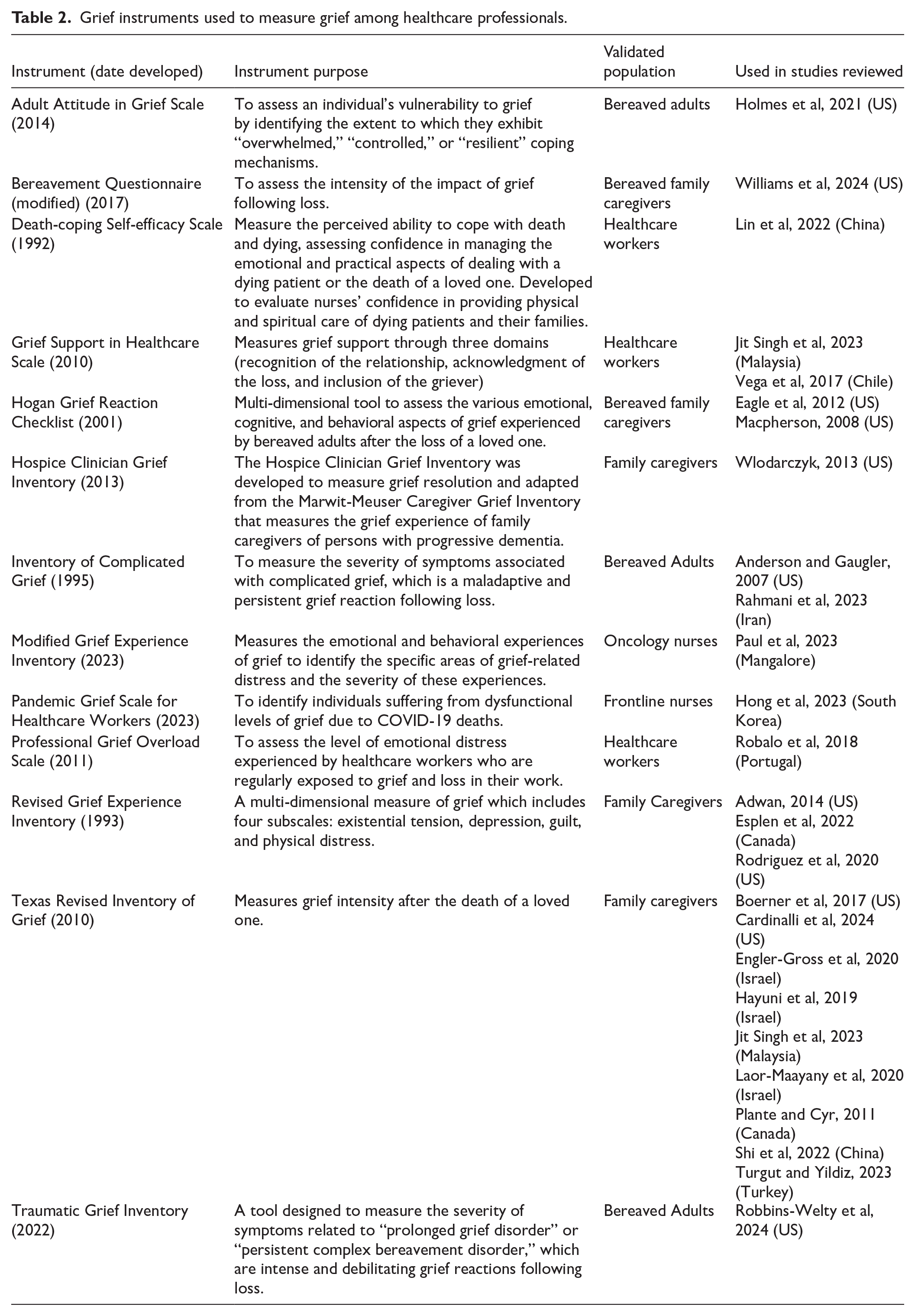
Thirteen valid and reliable instruments were used to measure grief (Table 2). However, most of these instruments have been validated for assessing grief in family caregivers or bereaved adults and have not been specifically tested or validated for use among healthcare workers. Only five of the instruments included in this review have been validated in healthcare worker populations.36,83,94-97 Seven studies used non-validated, investigator developed surveys to measure various dimensions of grief among their participants.68,90,98-102
Grief instruments used to measure grief among healthcare professionals.
Grief Intensity
Most of the studies that used validated family caregiver grief instruments, registered low to moderate levels of grief intensity upon measurement.9,34,41,42,94,103-109 Plant et al 110 found high levels of grief intensity among participants and notably highest among the respiratory therapists in their sample. Further, Rahmani et al 12 found that nearly 60% of nurses in their study were suffering from complicated grief. The two studies62,83 that used validated instruments for bereaved adults in general, showed a mixture of results. Paul et al 83 found that 66% of nurses in their study had moderate to high levels of grief and Holmes et al 62 found that 16.22% of social workers in their study had severe grief symptoms. The instruments developed specifically for healthcare professionals measured a variety of grief factors, such as grief support, professional grief overload, death-coping self-efficacy, and pandemic grief intensity. Overall, these studies found that low to moderate levels of grief support,94,95 low level of professional grief overload, 36 and a medium level death-coping self-efficacy. 96
Contextual Factors, Associations, and Predictors of Grief Intensity
Grief intensity was significantly and positive correlated with burnout,42,103,104,106,111,112 secondary traumatic stress or compassion fatigue,41,103,104,112 loneliness, 97 insomnia, 97 and depression.97,111 Boerner et al 106 found that grief factors accounted for unique variance in depersonalization (a component of burnout), over and above staff, patient, and institutional factors. Hong et al 97 found that depression in nurses directly influenced pandemic grief reaction. Social support was the most consistent significant negative correlation,12,40,41 meaning that greater social support was correlated with less grief intensity. Jit Singh et al 94 found that grief support mediated the relationship between grief intensity and burnout through a significant indirect effect.
Other contextual factors that were associated with higher grief intensity were younger HCWs age, 110 gender, 12 and working less time on a unit with high levels of patient death. 9 Anderson and Gaugler 40 found that certified nursing assistants who reported higher levels of fear in their attitude toward death and who reported fewer deaths of residents in their facilities tended to experience higher levels of complicated grief. Lower levels of grief intensity were associated with having education in palliative or end-of-life care,9,36,96 comfort caring for terminal patients and supporting the patient’s family,9,96 and professional support from the hospital staff. 9 Notably, Agyei et al 98 found that 89% of their participant did not grieve the loss of patients due to fear or as a show of professionalism. Alternatively, Plante and Cyr 110 found that 70% of participants spoke with colleagues, 48% with friends and families, and that 37% believed this was what helped them most. Similarly, Strote et al 102 found that talking with colleagues (78%) or friends and family (69%) and simply continuing to work (61%) were the most common coping strategies and that post-death debriefing rarely or never occurred for 64% of their participants.
Intervention Studies
There were six quasi-experimental (non-randomized) studies examining the effect of an intervention on grief (Table 3).34,68,99,100,107,108 Five of the six studies were conducted in the United States. The interventions consisted of educational modules, debriefing, and storytelling. Most of the interventions involved a component of peer-support and were implemented with pediatric healthcare professionals. There was a large range of intervention lengths ranging from 2 sessions to a 3-day retreat. Four of the six interventions were categorized as system-level interventions since they were implemented with teams within one institution. Only two studies107,108 showed measured grief as a quantitative outcome of their study and neither study showed significant changes in grief intensity post-intervention.
Intervention characteristics.

Discussion
This scoping review extensively explores professional grief experienced by HCWs across various disciplines and specialties. Professional grief, distinct from personal grief due to its recurring and occupational nature, is deeply influenced by individual, interpersonal, and systemic factors, emphasizing the complexity of grief experiences in healthcare settings. Our findings suggest multiple levels where professional grief is impacted and could be addressed with a systems-level approach. This contribution is unique because grief is often viewed as a personal experience. Therefore, it should be dealt with at a personal level. HCWs encounter death and dying, sometimes in traumatic ways, as part of their occupation. Therefore, professional grief should be situated as a potential outcome of occupational exposure, death, and dying, which may have differential effects based on individual, interpersonal, and systems-level factors.
At an individual level, certain personal characteristics and experiences can shape how HCWs experience and cope with professional grief. Early-career vulnerability is well documented, with novice HCWs often feeling unprepared for patient deaths and reporting more intense emotional impact.113,114 Gender norms, personal loss history, and identification with patients or their families further influence the intensity of grief, highlighting the necessity of personalized support and educational interventions tailored to address these emotional complexities. Studies note that most HCWs enter the field without formal preparation for dealing with death, leading them to “learn by experience” and potentially struggle for years to find healthy coping methods115,116 and with greater risk for burnout, secondary traumatic stress, and depression if healthy coping methods are not achieved.97,106
Interpersonal factors also significantly shape healthcare professionals’ grief experiences. Patient-related factors such as age and circumstances of death can intensify grief. For instance, unexpected deaths or the death of a young patient often provoke stronger feelings of sorrow, guilt, or shattered expectations for HCWs. 15 Further, HCWs who develop a close therapeutic bond or care for a patient over a long period may experience the patient’s death as a significant personal loss.106,112,116 Our findings reveal that younger patient deaths, unexpected deaths, and prolonged suffering contribute to heightened grief responses. The notion of a “good death” versus a “bad death” emerged qualitatively, with HCWs finding solace in fulfilling patient wishes and minimizing suffering. Quantitatively, social support correlated with lower grief intensity, suggesting that professional grief is mitigated when HCWs feel they have provided appropriate end-of-life care. 94
Institutional culture can either mitigate or exacerbate professional grief. In some settings, there exists an unspoken expectation that “death is part of the job,” leading to a culture of silence where staff feel they must quickly “move on” without openly grieving. This lack of acknowledgment can make grief feelings more isolating. High workload and time pressures are other systemic factors—busy acute-care environments often allow little time for reflection or mourning, compelling clinicians to suppress grief and continue working. 15 Conversely, organizational support (or lack thereof) plays a critical role. Clinicians report better coping and less emotional exhaustion when healthcare institutions provide structured support—such as team debriefings, counseling services, or peer support. 80 Unfortunately, most studies found that HCWs do not feel adequately supported by their organizations in managing grief.
Different professions and specialties exhibit variations in grief experiences, shaped by specific clinical cultures and professional expectations. For instance, nurses may form closer bedside connections with patients, witness death more directly, and experience grief more emotionally. 59 Conversely, physicians tend to adopt a more transactional approach toward grief, focusing primarily on clinical outcomes. They may also be more prone to view patient death as a personal or professional failure, which can lead to feelings of guilt or suppressed grief.15,114 Uniquely, home care aides show greater interest in formal grief support, highlighting possible disparities in how various medical cultures acknowledge and manage emotional distress.39,74
The concept of a “good death” varies distinctly by specialty. For example, critical care providers prioritize control and predictability during end-of-life care, valuing structured clinical conditions. 48 In contrast, oncology and palliative care professionals emphasize comfort, peace, and symptom management as core elements defining quality death. 117 Expressions of grief and coping mechanisms in settings where HCW-patient relationships are longer and foster deeper emotional connections potentially intensify the grieving process. Nurses in long-term care, palliative care, oncology, and community settings face heightened emotional demands, frequently tasked with balancing emotions within the HCW-patient dynamic, often experiencing significant emotional labor, underscoring the necessity for supportive organizational structures and interventions. 118
Changing Healthcare Culture: Educational, Clinical, and Policy Recommendations
Based on the findings from this review, there is an urgent need for cultural change within healthcare environments, explicitly addressing the pervasive issue of emotional suppression and stigma associated with professional grief. Healthcare professionals often feel pressured to repress emotional responses to maintain a professional image. This professional culture limits genuine emotional processing, intensifies isolation among HCWs, and contributes to emotional exhaustion.
Comprehensive educational, clinical, and policy-level interventions are necessary to transform healthcare culture effectively. Pre-licensure education is a critical starting point, yet current curricula significantly lack approaches to teach emotional resilience, grief management, and skills to cope with complex work-related emotions.119-123 To address these gaps, educational institutions should incorporate structured grief education including personal coping assessment, emotional awareness, and boundary management strategies through simulation-based training.64,118,122,123
Healthcare institutions must prioritize ongoing, structured grief interventions such as peer support groups, professional counseling services, and formalized grief-processing programs embedded within workplace culture.11,17 But as this review shows, these programs are often underutilized by HCWs, likely because of cultural norms and systemic barriers. In embracing the framework of Total Worker Health, as proposed by the National Institute for Occupational Safety and Health (NIOSH), policy changes are necessary to create a work environment that addresses the safety, health, and well-being of health care professionals by acknowledging the workplace exposures of grief and loss.124,125 While grief as a workplace exposure has not been fully recognized, it falls under the umbrella of psychosocial stressors. 126 We propose that grief-related stress be formally recognized as a work-induced condition, thereby allowing affected workers to access mental health support, bereavement leave, and structured debriefing sessions. Additionally, updating workers’ compensation frameworks to cover the emotional toll of chronic exposure to loss could mitigate long-term mental health consequences and improve retention rates in the healthcare workforce. These changes validate healthcare professionals’ lived experiences and pave the way for a more supportive and sustainable work environment.
Research Implications
Future research should concentrate on developing and evaluating evidence-based interventions designed for the unique experiences of healthcare disciplines and specialties, recognizing distinct patterns in how grief manifests and is processed among individuals and professional roles. Additionally, research must systematically address institutional barriers—such as time constraints, stigma, and inadequate access to formal support—that currently limit healthcare professionals’ ability to cope with professional grief effectively. There is also a critical need for more precise measurement frameworks, as existing instruments primarily assess familial or informal grief, not capturing the unique nuances of professional contexts. Opportunities for future studies include refining professional grief measures to capture professional grief experiences better and to conceptually distinguish professional grief from other constructs such as burnout, compassion fatigue, moral distress, and moral injury.
Limitations
This review isn’t without limitations. First, we only included studies written in English, which may have resulted in the absence of literature published in other languages. Second, we acknowledge that limiting our search to three databases and excluding grey literature might have resulted in missing some relevant studies or emerging data. Future research could expand the scope by incorporating additional databases or including grey literature to further enhance comprehensiveness. Third, many studies had small sample sizes, potentially limiting generalizability. Additionally, most of the studies included utilized qualitative methodologies, though rich in depth, which may reflect subjective interpretations and limit broader application. The absence of longitudinal studies further restricts understanding of how professional grief evolves over time and in response to prolonged exposure.
Conclusion
This review highlights the significant and multifaceted nature of professional grief among healthcare professionals, underscoring the urgent need for systemic changes to better address emotional well-being. Integrating qualitative and quantitative research findings across professions and specialties reveals substantial gaps in education, institutional support, and effective grief interventions, emphasizing the complexity of professional grief within healthcare contexts. A shift in the healthcare culture from one that values stoicism and emotional suppression to one that normalizes emotional expression is imperative for any future strategies to be successful. By actively acknowledging grief as an inherent aspect of healthcare work and embedding supportive practices into the healthcare culture, institutions can significantly mitigate psychological distress among healthcare professionals, enhance their resilience, and ultimately elevate patient care outcomes and professional sustainability.
Supplemental Material
sj-docx-1-his-10.1177_11786329251344772 – Supplemental material for Hidden in Plain Sight: A Scoping Review of Professional Grief in Healthcare and Charting a Path for Change
Supplemental material, sj-docx-1-his-10.1177_11786329251344772 for Hidden in Plain Sight: A Scoping Review of Professional Grief in Healthcare and Charting a Path for Change by Carolyn S. Phillips, Katie Trainum and Megan C. Thomas Hebdon in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329251344772 – Supplemental material for Hidden in Plain Sight: A Scoping Review of Professional Grief in Healthcare and Charting a Path for Change
Supplemental material, sj-docx-2-his-10.1177_11786329251344772 for Hidden in Plain Sight: A Scoping Review of Professional Grief in Healthcare and Charting a Path for Change by Carolyn S. Phillips, Katie Trainum and Megan C. Thomas Hebdon in Health Services Insights
Footnotes
Acknowledgements
The authors would like to thank Dona Ravandi, Aashi Vishnoi, and Saneeva George for their contribution to the scoping review.
Author Contributions
CP and MH conceived and designed the review. CP developed the search strategy, and CP and KT conducted the literature search. CP and KT screened and selected the studies, extracted the data, and carried out the analysis and interpretation. All authors reviewed, read, and approved the final version of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.