
Abstract
Introduction/Objectives:
African American persons living with Alzheimer’s disease and related dementias (ADRD) experience health disparities in health care decision making. This study’s objective is to understand what influences health care decision making for African American persons living with ADRD from the perspectives of primary care providers and care team members.
Methods:
Twenty primary care providers and care team members completed semi-structured interviews to identify barriers associated with their involvement in health care decision making for African American persons living with ADRD. The interviews were analyzed with directed content analysis.
Results and Conclusion:
Three themes were identified: Systemic Healthcare Obstacles; Relational Healthcare Obstacles; and Individual Health Care Obstacles. The themes diverged to yield 9 categories (Inability to See/Hesitancy to Address Racism; Care Coordination at End of Life; Perceived Lack of Trust; Inadequate Answers and Connections; Uncertainty with Decision Making; Racial and Ethnic Identity; Lived Experiences; Definition of a Good Decision; and Hurt Feelings) and 2 subcategories (Cultural Miscommunication and Time to Build Mutual Understanding). To effectively support decision making processes for African American persons living with ADRD, there is a need to equip primary care providers and care team members with means to identify and address obstacles at multiple levels.
Keywords
Introduction
Numerous studies and reports have documented disparities in the health care of African Americans, including older adults.1,2 These healthcare disparities, such as challenges with access to health care and quality disease manage-ment, often result in a disproportionate disease burden in African American communities. 1 Of relevance to this study, African American older adults have approximately double the prevalence of Alzheimer’s disease and related dementias (ADRD) compared to non-Hispanic White older adults, 3 increasing the need for family caregiving in this racial group. 3 Importantly, family caregiving is highly dependent on access to quality health care. 4
Health care is essential to the treatment and management of persons living with ADRD. 5 With the shortage of dementia care specialists, primary care providers play a pivotal role in the treatment,5,6 management,5,6 and maintenance of quality of life6 -9 of persons living with ADRD. Eighty two percent of primary care providers report they are the frontline providers of ADRD care in the United States. 6 Despite their role in ADRD care, some primary care providers feel ill-equipped and uncomfortable answering patients’ questions about ADRD care. 10 As a result, some primary care providers feel uneasy diagnosing someone with dementia. 10 This lack of understanding and agency is a barrier for families, and even more so for African American families who are also more likely to experience challenges related to social determinants. 11 African American care partners expect primary care providers to be the point of contact for an ADRD diagnosis and to possess the knowledge needed to support these care partners with navigating health care decisions. 11 In addition, African American care partners expect other care team members to be liaisons between them and primary care providers. 11 Despite the importance of both primary care providers and their care team members, there is limited research from their perspectives on their experiences with supporting African American families navigating health care decisions for African American persons living with ADRD. Therefore, we do not know how these experiences frame and dictate the healthcare quality and outcomes for African American persons living with ADRD.
This study was informed by The Black Family Socio-Ecological Context Model (Figure 1), 12 a conceptual framework that considers the ecological contexts of African American older adults. This model suggests that relationships move from larger systems through successively smaller systems in a substantial way. 12 For example, healthcare systems influence community settings; community settings influence family units, which in turn influence individuals. As a result, interactions with primary care providers and other members of the care team influence the decision-making processes for African American persons living with ADRD and their family care partners.
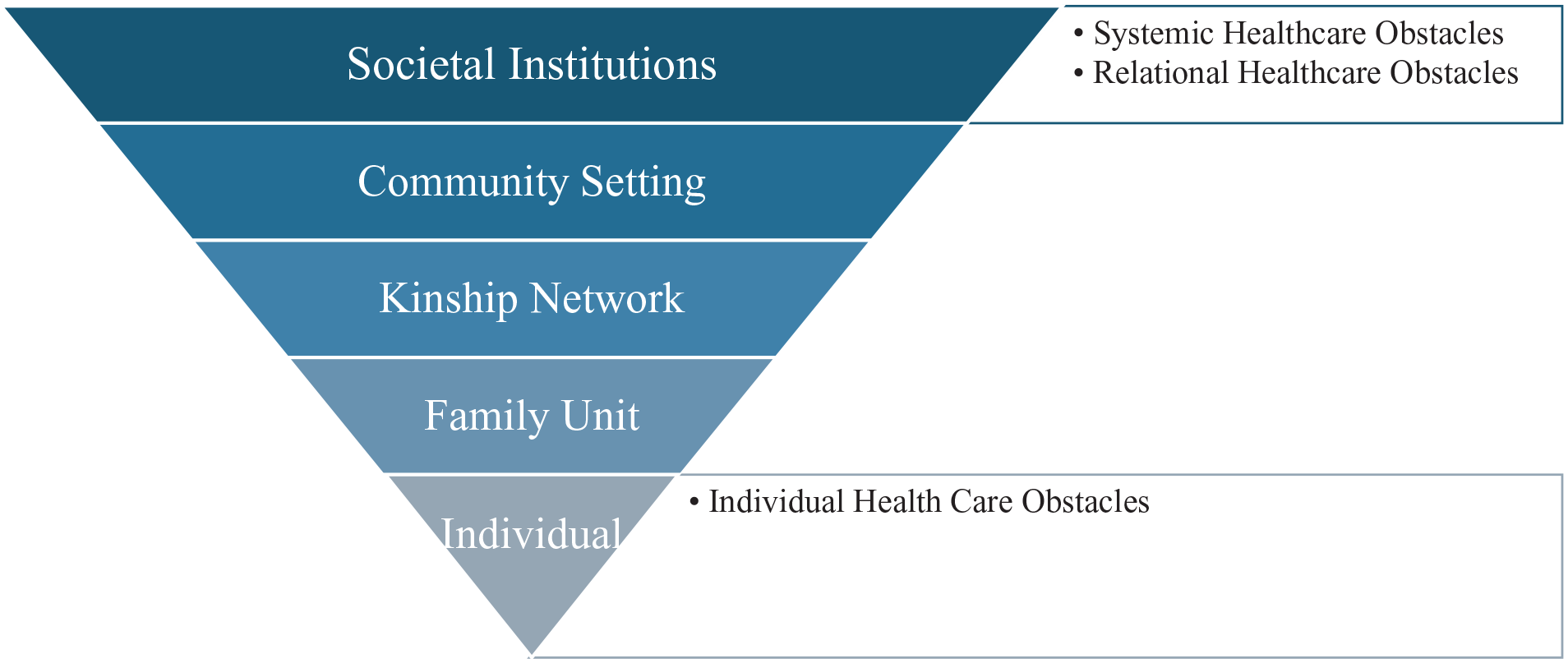
Adapted depiction of the Black Family Socio-Ecological Context Model.
Methods
Participants
Data were collected between November 2021 and July 2023 via phone calls and Zoom teleconference study visits with 20 healthcare providers or staff who currently or previously worked in primary care. Participants who had previously worked in primary care had done so within the last 4 years of the study visit. The primary care providers included physicians and nurse practitioners while the care team members were nurses and social workers. Participant criteria included: (1) being 18 years or older, (2) having provided or currently providing care for African American persons living with ADRD, (3) participating or having participated in health care decision making for African American persons living with ADRD, (4) ability to read, speak, and understand English, and (5) having access to a computer, tablet, or smartphone with internet or a telephone for the study visit. Participants were recruited via national conferences, flyers posted in magazines and on social media sites, and convenience sampling. Refer to Figure 2 for the flow chart of recruitment. This study was approved by the Institutional Review Board at Emory University.

Study recruitment flowchart.
Procedures and Materials
Over the phone, the first author explained the study, screened potential participants, and scheduled the study visit when appropriate. At the visit, participants were consented and completed a semi-structured interview. All study visits were conducted and recorded via Zoom, except for one due to connectivity issues that was conducted over the phone. A digital device was used to record the interview. On average, interviews lasted 41 min, ranging from 28 to 65 min. At the end of the interview, study-specific demographic data were collected to add context to the interviews. Data collection continued until meaning saturation.13,14 All interviews were digitally recorded, uploaded to a secure server, and transcribed verbatim. The first author and research team compared the recordings and transcripts for accuracy. After each study visit, the first author wrote field notes including detailed descriptions, important topics, and personal reflections.
Qualitative Interviews and Analysis
The investigative team developed semi-structured interview questions guided by the Black Family Social-Ecological Model, 12 the Alzheimer’s Association’s 6 2020 report on discrimination and racism in healthcare, and other research in health care decision making for African American persons living with ADRD. Thus, the participants’ responses about racism were prompted by these questions. We asked additional probing questions to further prompt discussion. Transcripts were stored in MAXQDA, a software program designed to manage qualitative data. 15 Using de-identified transcripts, we used qualitative directed content analysis 16 to address our study aims.
Qualitative data were examined using the following steps. First, the first author read and reviewed all data to gain an understanding of the content related to the study aims. The first author and 3 others independently reviewed the same 3 transcripts, highlighting passages of text that appeared to relate to obstacles in health care decision making. Second, the coders used in-vivo coding on the highlighted text. In vivo coding emphasizes the exact words from participants to prioritize their voice. 17 The coders independently coded the remaining transcripts. Third, once all the transcripts were coded, 2 of the coders clustered the in-vivo codes. These clusters were organized into categories based on whether they “look alike” or “feel alike.” 17 Themes were constructed from these categories and named to capture the essence of the categories. The themes were organized hierarchically based on the Black Family Socio-Ecological Context Model. 12 To assist with quality control, the participants who agreed to be contacted after the study were provided with the codes, categories, and themes for member checking. Those who responded expressed agreement with the results.
Results
Participants included 20 physicians, nurse practitioners, nurses, and social workers who were currently working or had previously worked in primary care practices in the United States. Most were physicians (n = 10) and female (n = 16), and 7 self-identified as non-Hispanic White. Primary care providers and care team members predominantly worked or previously worked at healthcare systems affiliated with large academic institutions (n = 9). Primary care providers and care team members had an average of 14.6 years of experience (ranging from 1 to 37 years) and predominantly worked in the southeast region of the United States with caseloads of 30-50% African American older adults. Refer to Table 1 for all demographic information.
Participant Characteristics.

3 (100%) of Nurse Practitioners, 8 (80%) of Physicians, 2 (67%) of Registered Nurses, 3 (75%) of Social Workers
Indian, South Asian
Salvadorian
Latino
Grenadian, Nigerian.
Our analyses reveal 3 themes that influence or frame decision making processes. These themes were further broken into 9 categories and 2 subcategories. The 3 themes are (1) Systemic Healthcare Obstacles, (2) Relational Healthcare Obstacles, and (3) Individual Health Care Obstacles. The theme Systemic Healthcare Obstacles has 2 categories: (1) Inability to See/Hesitancy to Address Racism and (2) Care Coordination at End of Life. The Relational Healthcare Obstacles theme has 3 categories and 2 subcategories. The categories are (1) Perceived Lack of Trust, (2) Inadequate Answers and Connections, and (3) Uncertainty with Decision Making. The category, Perceived Lack of Trust, has 2 subcategories: (1) Cultural Miscommunication and (2) Time to Build Mutual Understanding. The last theme, Individual Health Care Obstacles, has 4 categories: (1) Racial and Ethnic Identity, (2) Lived Experiences, (3) Definition of a Good Decision, and (4) Hurt Feelings. Our analysis is discussed in more detail below with a clear depiction of the in-vivo codes, categories, subcategories, and themes in Figure 3. In-text quotes from the participant are provided to support the themes, categories, and subcategories.

Codes, categories, subcategories, and themes.
Theme 1: Systemic Healthcare Obstacles
Participants described experiences or situations that were related to the larger healthcare system and have societal implications.
In the category, Inability to See/Hesitancy to Address Racism, there were 3 common responses. Some participants acknowledged that racism existed in healthcare, but they had not witnessed it:
You know, um, I mean, I grew up with, um, three healthcare experiences of rank racism where I lived. . . I think about in the healthcare experience with patients with dementia, I can’t say I’ve seen that level of somebody just flipping out their KKK card (chuckles) or anything like that. Participant 13. non-Hispanic White, male, physician
Other participants shared that they had witnessed racism or racist practices in the healthcare system, but they did not know how to bring up this conversation with African American persons living with ADRD or their African American family care partners:
But, you know, so there are times it’s like, “I wish that they really, really knew that I really am there for them. Like, I really. . . Like, I see the discrimination, I get it, and I, you know (sighs). . . But it’s like, how do I bring that up? Participant 1. non-Hispanic White, female, nurse practitioner
While other participants were unsure if they had witnessed racism but inferred that they had when the situation was compared to that of a non-Hispanic white person living with ADRD:
It seems it happens more frequently in the African American population. . ., you know, and maybe we’re reading it wrong in terms of what it is, but it really does feel like discrimination and racism because we don’t see the same thing happening. . . in, really in, in, in white people, in white patients. Participant 18. White Hispanic, female, physician
These responses were shared by both primary care providers and care team members across all racial and ethnic groups in the study. Participants recognized that encounters like these resulted in substandard care for African American persons living with ADRD (e.g., did not receive “full assessment” or not recommended for health screenings) or a denial of services (e.g., not admitted into a dementia-specific program or referred to a specialist but never seen by the specialist).
In the category, Care Coordination at End of Life, some participants described difficulties with aligning end-of-life decisions among multiple healthcare providers, the person living with ADRD, and their family. This care coordination often required multiple conversations between multiple providers and the care team members, which was time consuming:
Um, the main issue, I think, that was noted is that the family, you know, didn’t know what to do because he [African American person living with ADRD] had been back and forth with many providers outside of the VA System. Participant 9. non-Hispanic Black, female, physician
While end-of-life decision making is challenging regardless of racial identity, participants shared fears about when they recommended stopping or holding treatment that they or their healthcare system might be viewed as racist:
I am very interested in my use of dementia medication that I think they are not appropriate in a lot of people. But I might be more likely to offer it to, to a Black patient. Thinking that if-, worried that if I don’t, that they might think that I am withholding treatment from them. Participant 18. White Hispanic, female, physician
Theme 2: Relational Healthcare Obstacles
Relational healthcare obstacles were considered poor connections or the absence of relatedness between the primary care providers and care team members and the African American persons living with ADRD and their family care partners.
In the Perceived Lack of Trust category, participants shared what happens within their relationships with families of African American dementia persons living with ADRD. Participants shared how they viewed a lack of trust as negatively influencing their relationships as well as how this lack of trust influenced how the primary care providers participated in health care decision making. The lack of trust was described bidirectionally. The participants felt African American families did not trust them and so the participants often did not know how to establish trust with these patients:
I automatically think they [African American families] don’t trust me. Whether or not that that’s true but that’s what I’m taught (laughs) is to, you know, like, there’s that trust element. And so, I’m always thinking that like what if, is what I’m saying landing in a way that makes them trust me more or less. Participant 18. White Hispanic, female, physician
The lack of trust complicated health care decision making, especially when there was a recommendation that medical treatment be discontinued. Primary care providers were hesitant to stop treatments even when warranted for fear of disappointing either the African American person living with ADRD or their care partner:
I think sometimes, too, along with that type of sentiment, if there’s ever a talk on stopping medicines that may not be beneficial, I think that sometimes if people think that they’re being told that they can’t have something or it’s not beneficial, I’m very conscious of- of- of the feeling that maybe that their loved one’s not getting care. Participant 4. non-Hispanic White, female, nurse practitioner
As a result, participants agreed that the lack of trust in the relationship precipitated miscommunication that was often related to cultural differences:
Because there is a lot of times, there is a cultural divide between the healthcare provider and the patient and so you know. . . so it makes a big influence. Participant 17. non-Hispanic African American, female, social worker
In addition, participants shared that the amount of time it took to build mutual understanding was greater with families of African American persons living with ADRD compared to non-Hispanic White families. Participants admitted that they were likely to be blamed for this increased time because they did not invest in “families as a unit”:
I think barriers to dementia care often, for African American patients, might be that people haven’t done a full assessment of what the situation is and how to provide them the best level of care and support. So, I- I think time and really investment in the patient and family as a- as a unit on what their care. . . I- I- I definitely can see it as a barrier. Participant 4. non-Hispanic White, female, nurse practitioner
In the category, Inadequate Answer or Connections, the participants explained how they try to support African American persons living with ADRD and/or their family care partners but sometimes there are no “good answers.” Depending on other socioeconomic contexts, sometimes there were no perceived viable options and hence decisions that could be made:
In talking with them, particularly about caregiving options and support, right, that tends to be a huge issue across the board. . . Like, there’s not- there’s not any options to make the plan a better plan. You know? Participant 2. non-Hispanic White, female
Uncertainty with Decision Making is the final category in this theme. Participants acknowledged the important health care decisions that need to be made for African American persons living with ADRD. Participants who were nurse practitioners and social workers shared that there was a sense of uncertainty with how to support these decision-making processes. Reasons for this uncertainty seemed to stem from primary care providers’ and care team members’ lack of cultural understanding of variables that are relevant to decision making for African American persons living with ADRD:
But it was just hard to watch because their mom had no quality of life. And I didn’t think it was a good choice for them to be making that, but at the same time, trying to acknowledge that they’re influenced to make these decisions probably based on what they’ve experienced. Participant 1. non-Hispanic White, female, nurse practitioner
Theme 3: Individual Health Care Obstacles
The last theme highlighted the importance of unique, individual characteristics of either the primary care providers, the care team members, the African American persons living with ADRD, or their African American family care partners.
The first category, Racial and Ethnic Identity, described a more internal process of how the participants’ own beliefs about identity influenced health care decisions for African American persons living with ADRD. Half of the participants described their racial and ethnic identity as an obstacle:
I think to be honest from my perspective, I always have this fear of, you know, I’m a, I’m a white clinician coming at you. Participant 18. White Hispanic, female, physician
On the other hand, a few participants described their own racial and ethnic identity as unimportant to the health care decision-making process for African American persons living with ADRD.
I don’t think it [race or ethnicity] influences either way. At least, I have not seen or heard of any indication that that plays a role on how patients’ care is given. Participant 3. Hispanic, male, registered nurse
Of the participants who described racial and ethnic identity as an obstacle, all identified as either non-Hispanic White or non-Hispanic Black females and represented both primary care providers and care team members. The few who felt their racial and ethnic identity were not important identified as Hispanic and Asian men.
Participants highlighted their lived experiences in childhood and adulthood were different from most of the African American persons living with ADRD whom they supported:
Um, I mean, I’m not African American, and I, I don’t share that same background in that way. . . I acknowledge that there are things that exist that I’m just not clued into. Participant 14. non-Hispanic White, female, physician
This finding resonated with participants from across all healthcare roles and across a few racial and ethnic groups (i.e., non-Hispanic African American, non-Hispanic White, and Asian). As a result, some of the participants felt less qualified to support these African American persons living with ADRD and their family care partners.
For participants who shared similar lived experiences, their current role in the healthcare system was a barrier:
You know, there are families who, ‘Okay, social worker. . .’ They forget about the medical. They see a social worker, they think I’m coming in and trying to control or take away their independence or force them into placement. Participant 20. non-Hispanic African American, male, social worker
In the next category, Definition of a Good Decision, participants explained that a good decision was one that was supported by their clinical expertise, often supported by research, and that would have a positive outcome for the African American person living with ADRD. However, there were times when what the African American persons living with ADRD and/or their family care partner wanted did not align with how the participants defined a good decision (e.g., tube feeding placement near end of life):
And I think that oftentimes patient choice is really kind of eliminated from all of that [health care decision making] . . . a lot of times what we want is well- intentioned, but, um, you know, it’s- it’s frustrating in that it’s not what she [African American persons living with ADRD] wants. Participant 1. non-Hispanic White, female, nurse practitioner
One participant added more nuance to the discussion by sharing that he believed many African American family care partners viewed “death as a failure”:
And, um, and it was about two or three days of everybody thinking through [end-of-life decision making] and then the angry, lead person that was kind of like, you know, conscientiously, frankly, but viewed death as a failure. . . Participant 13. non-Hispanic White, male, physician
Lastly, these health care decision-making processes were not without hurt feelings. Hurt feelings seemed to be a byproduct of perceived failure in best outcomes for the African American person living with ADRD. Participants expressed hurt feelings and moral distress. These feelings were expressed by the care team members and not the primary care providers:
And, you know, when you have, in a service position like this like it’s like we always get our feelings hurt. . . I can’t do anything [to move the decision-making process forward] because I’m not your legal guardian. Participant 17. non-Hispanic African American, female, social worker
Discussion and Conclusions
In this study, we identified 3 themes, 9 categories, and 2 subcategories regarding obstacles that influence health care decision making for African American persons living with ADRD in primary care settings. While some of these topics have been identified in previous research, this study is one of few in which the perspectives of physicians, nurse practitioners, nurses, and social workers are the subject matter. Our findings suggests the stated desire of primary care providers and care team members to positively influence health care decision making for African American persons living with ADRD is thwarted by (1) structural norms and systems that were never designed to meet the needs of African American persons living with ADRD, (2) perceived relational obstacles and little framework, mechanisms or intentional tools to dismantle such obstacles, and (3) limited individual empowerment and skill in identifying and navigating individual factors for all stakeholders in a constructive manner.
Addressing Systemic Factors in Primary Care
To better understand how to address racism in healthcare, we must recognize how it works and how it is operationalized at the level of the healthcare system. Structural racism operates at the level of society within the United States,18,19 which is directly related to the United States being founded on both ideals of freedom for non-Hispanic white persons and the enslavement of African American persons. 20 Aside from interpersonal and intrapersonal perpetuation, racism has been embedded in institutions, social structures, and processes that have resulted in inequities in resources, power, and lived experiences. 21 Since the era of Jim Crow laws (1875-1968), 22 racism has played a fundamental role in the United States government’s structuring of the healthcare system. 23 For example, The Hill-Burton Act of 1946 was enacted to provide grants to modernize public hospitals and long-term care facilities. 24 Although the act decreed healthcare facilities to be made available to anyone regardless of race, it allowed states to develop racially segregated and unequal facilities that were under resourced due to the denial of grant funding. 24 Thus, the healthcare systems in which African American persons living with ADRD seek to receive health care and make health care decisions were not established or designed with intention to meet the culturally-specific needs of African American persons living with ADRD.
While the clinical encounter between primary care providers and African American dementia dyads may not be the appropriate place to confront structural racism head on, it is the place where health care decisions for African American persons living with ADRD are often made. Therefore, primary care providers and staff play a major role in addressing racism in primary care. 25 The point at which health care teams and patients interact may be the optimal place for developing and implementing interventions that begin to unravel and disentangle structural racism. These interventions may also need to consider the gender of the primary care providers and care team members as racial and ethnic identity seemed to resonate as an obstacle with the female participants. The male participants did not think their race or ethnicity influenced their encounters with African American persons living with ADRD and their family care partners. Further research is necessary to begin to tease out the nuances of identity with addressing racism and whether perceived versus actual racial biases in care exist in these clinical interactions, which may affect outcomes for African American persons living with ADRD and their family care partners.
Primary care providers and their care team members direct the care of their patients across multiple healthcare settings and with other healthcare professionals (e.g., specialists). This organization and coordination of care is time-consuming and can result in important factors being missed or ignored. Having systems and processes in place to help with this coordination is necessary. Direct communication channels to a care team member or the use of voicemail systems that allow persons living with ADRD, their family care partners, and other healthcare professionals who are a part of the care team to leave pertinent information may show promise. 26 Such systems need to recognize that African American persons living with ADRD (and other families) may have multiple care partners who need to be included in their health care decisions, particularly regarding end-of-life decisions. Finding ways to organize information and sharing it with all interested parties remains a work in progress.
Relationship and Individual Factors in Primary Care
Both relationship and individual factors may influence primary care decision making with African American persons living with ADRD and their family care partners. First, participants shared that the differences in their own identity and lived experiences negatively influenced decision making for African American persons living with ADRD. Second, participants believed a lack of trust precipitated miscommunication related to cultural differences. Third, participants perceived more time was needed to build mutual understanding with African American persons living with dementia and their family care partners compared with persons living with ADRD and their family care partners who were non-Hispanic White. Taken together, these findings highlight areas of improvement and opportunities to intervene with primary care providers and their care teams to develop their abilities as guides, advocates, and vested stakeholders in the decision-making process for African American families of persons living with ADRD. Tools and protocols to clarify health outcomes and cultural beliefs are needed.
One approach that might reinforce these efforts is the use of interventions framed by the Relationship Management Theory. 26 This theory was used to unders-tand patient-provider relationships of low-income African American patients and their primary care providers through understanding common interests and shared goals. 26 Using this theory to develop protocols that help primary care providers and care team members identify commonalities and important variables African American families consider when making health care decisions may hold promise. Another approach involves utilizing a conceptual model that outlines the general process of how provider-to-provider trust is built. 27 This conceptual model suggests that provider-to-provider trust building is required to assist patients with receiving the care that they need from other providers. The primary care provider’s ability to follow up and follow through with other providers builds trust. Families can depend on the provider to deliver for them, even when challenges such as having multiple care providers are apparent. This, in turn, can build rapport, helping to alleviate factors such as perceived lack of trust and limited access. Using this conceptual model might be helpful with navigating care coordination at the end of life, when the possibility of multiple providers is common.
Primary care providers often share that their role allows access to build rapport with their patients over the years. 28 Thus, insights may also be gained from the participants in the study who had both the ability to see and address racism that was encountered by African American persons living with ADRD and/or their family care partners. For many of the African American and Black American participants, their shared lived experiences or shared phenotypic traits with the African American persons living with ADRD and/or their family care partners allowed for a shared understanding of structural racism. For the participants who did not identify as African American or Black American, their approaches were as follows: (1) a willingness to take the necessary time to slowly build rapport with the African American dementia dyads and (2) an acknowledgement of the role of systemic racism in exacerbating the challenges of health care decision making for African American persons living with ADRD.
Primary care providers and their care teams may be unable to instinctively anticipate the health care decisions of African American dementia dyads. Participants discussed how hard it can be emotionally when patients made decisions that contrasted with their initial plan. Emotional distress can lead to provider burnout and poor mental health, which can further influence the diminished quality of care that is delivered to patients, particularly racially and ethnically underrepresented ones. One study found that resident physicians’ negative emotional states had been shown to be associated with greater explicit racial bias in medical decision making. 29 As such, primary care providers and their care team members may need a place where they can share their feelings, so they are better equipped to support African American persons living with ADRD and their family care partners. Meanwhile, African American persons living with ADRD and their family care partners may need additional time to process the decisions that they need to make and to include additional family members when making these decisions. 30
Limitations and Future Directions
The current study had notable limitations. First, the sample size of nurse practitioners, nurses, and social workers was small, limiting the ability to fully capture the distinct perspectives of each profession. Future studies should recruit larger, profession-specific samples to better understand the unique insights that arise from their distinct responsibilities and scopes of practice. Second, many of the participants were female, which limited our ability to capture perspective from males who remain the predominant gender of physicians providing primary care. 31 Third, while the participants were asked to describe their experiences with African American families, “African American” was not operationalized during the interview. As a result, participants may have referenced individuals from the larger Black diaspora who may not identify as African American. Having a clear description and shared understanding during interviews may be needed in future studies. Fourth, most of the participants were living in the southeastern region of the United States, which may introduce regional bias into the findings of our study. Future studies should try to have a similar number of participants from all 5 regions of the United States. Fifth, all the interviews were conducted by the first author, who identifies as an African American woman. The first author’s headshot was on the recruitment flyer, and she conducted the recruitment efforts at national conferences. Thus, the transparency of her phenotypic trait (i.e., skin color) was apparent for most of the participants who contacted the study regarding participation. Participants did not verbally or physically display any discomfort with discussing race or racism in their health care practices and were forthcoming with information during the interviews. Fifth, the interviews were conducted shortly after the social unrest of 2020 related to the United States’ reckoning with racism due to the murder of George Floyd, which may have heightened open acknowledgment of structural racism.
Despite these limitations, this study captures the voices of healthcare professionals caring for African American persons living with ADRD and the obstacles faced with navigating health care decisions. The main strength of this study is the use of qualitative methods. As recommended during the 2023 Dementia Care Summit, 32 our study aligns with 1 of the new 8 milestones, which suggests the use of “qualitative, mixed methods, and design thinking approaches for advancing equitable care and caregiving research.” Findings from this study elucidate obstacles that impede families of African American persons living with ADRD from effectively making health care decisions. Future research should focus on methods and interventions that foster successful health care decision making for these families.
Footnotes
Acknowledgements
The authors want to thank undergraduate students, Jessica Arciniegas, Faith Mason, Srinidhi Prasad, and master’s student, Kennedy Payne, for help with coding the transcripts, reviewing comments and organizing the references, respectively. The authors also want to thank the participants and the community advisory board, especially Dr. Karin Small Wurapa, who generously donated their time and openly shared their experiences.
Ethical Considerations
Emory University’s Institutional Review Board approved the study (IRB#: STUDY00003022).
Consent to Participate
All participants provided informed consent.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The views expressed in written training materials or publications and by speakers and moderators do not necessarily reflect the official policies of the Department of Health and Human Services; nor does mention of trade names, commercial practices, or organizations imply endorsement by the U.S. government. Partially funded through the National Institutes of Health National Institute on Aging grant number [K23AG073516 and K07AG076616] for Dr. Bonds Johnson; and National Institute on Aging grant number [R01AG054079] for Dr. Hepburn. Drs. Johnson and Hepburn both receive support from the US Health Resources and Services Administration [HRSA 1U1QHP53036]. This content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or HRSA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The first author will share upon reasonable request.