
Abstract
While the experience of psychological safety among nursing staff has been studied, there needs to be more research on the perceived psychological safety of nurse managers. Generally, nurse managers are committed to their work, but the COVID-19 pandemic increased their intentions to leave. This cross-sectional study investigated the relationships between psychological safety, social support, and commitment among nurse managers. The data were collected in 2023 through a web-based survey from Finnish social and healthcare workers’ trade union members. Of the 4573 participants, this study further focused on 366 nurse managers and are reported in accordance with the STROBE checklist. Findings revealed that nurse managers’ perceived psychological safety was higher than among other workers. Nurse managers in public healthcare perceived lower psychological safety than managers in private and third sectors. A mediation model showed that social support partly mediated the positive effect of psychological safety on commitment. A psychologically safe environment enables more social support, thus enhancing the commitment. Dedicated nurse managers play a crucial role as a fundamental asset within the healthcare system.
Introduction
Patients’ problems are becoming increasingly complex, and the availability and sufficiency of nursing staff remain uncertain, 1 thereby exerting additional pressure on nursing management and leadership. The role of nurse managers is demanding, with studies indicating that up to 27% of nurse managers experience depression. 2 Despite this, there is limited evidence regarding psychological safety, which can substantially contribute to the mental well-being of nurse managers. 3 Investigating the psychological safety of nurse managers is crucial as it provides insights into the psychosocial working conditions of nursing workplaces. This study investigated the role of social support as a mediator between nurse managers’ psychological safety and commitment. The findings can be utilized to improve factors related to the well-being of nurse managers, enabling them to stay in their work. Interestingly, it has been observed that the perception of psychological safety tends to increase with higher positions in the hierarchy of the healthcare organization. 4
Psychological safety was first introduced in the literature over 50 years ago, described as a safe atmosphere where one can take risks and feel secure.5,6 Organizations expect employees to engage in the continuous improvement of processes, which may involve activities such as generating ideas and experimenting with new procedures. Introducing new ideas challenges the culture of tradition and established ways of doing things. At times, new ideas may run counter to the personal interests of employees. Failed improvement efforts can lead to those who proposed them being disfavored, which may affect employees’ willingness to voice areas for development. In a psychologically safe environment, honest feedback is encouraged and provided, collaboration is genuinely fostered, and there is a readiness to experiment with new approaches, even when the outcomes are still unclear. 7 A psychologically safe environment enables effective organizational performance. 8 Associated outcomes of psychological safety in healthcare include improved staff well-being, reduced stress, and commitment to enhancing quality. 3 Interpersonal support within a team, involving support from colleagues or leaders, has been identified as a mediator between psychological safety and well-being. 9
According to Northouse, 10 leadership can be understood as a dynamic process, whereby an individual guides and influences a group of people toward a common goal through the exertion of their authority and influence. Positive leadership styles are linked to psychologically safe workplaces. 7 Leadership dimensions contributing to psychological safety include empathetic interaction with employees and encouraging behavior from leaders, 11 organizational communication openness,12,13 strong leader-employee relationships,11,14 accessibility,15,16 and employees’ perception of being heard 17 and valued. 18 A participative leadership style by nurse managers enhances employees’ psychological safety19–21 and appears to be associated with commitment. 22 A transformational leadership style has also been found to increase employees’ psychological safety.23–25
Psychologically safe workplaces are associated with reduced errors and adverse events,20,26 improved patient safety,12,13,27 and the courage to address concerns.20,28 Such workplaces have been reported to lead to higher job satisfaction,12,29 work engagement,29,30 reduced job burnout,11,17,31 reduced hierarchy,16,32 and faster recovery from work. 33 Moreover, open communication in the workplace, both within the team and client interactions, enhances psychological safety. 13 Social support received from the workplace community,16,34 building relationships with fellow team members,15,34 trust within the team, 28 and ethical behavior 14 are all connected to psychological safety. Furthermore, psychological safety is associated with reduced intention to leave 12 and decreased turnover intentions.12,35
Social support can be defined as assistance and aid provided by others. 36 It can be acquired, for instance, from the work community, one's immediate supervisor, colleagues, or the organization. 37 Social support can be emotional, manifested through attention, trust, empathy, and courtesy. On the other hand, instrumental support may appear as material goods or providing specific assistance. Social support is reciprocal action involving the exchange of resources between at least two employees. 38 In addition to the traditional definition of social support, informal social support has been identified, which may involve, for example, the division of work among family members, enabling nurse managers to focus on their managerial duties. It has been estimated that informal social support is a crucial factor for the retention and future career development of nurse managers. 39 Moreover, social support has been assessed to be particularly significant, especially in the complex leadership work within healthcare, such as in a hospital environment. On the other hand, it is known that, according to the experiences of nurse managers, the support received in managerial roles is often insufficient. 37 In this study, social support encompasses the support provided by the nurse manager's superior, work community, and colleagues.
It has been assessed that nurses’ commitment is associated with a desire, need, or obligation to stay within the organization. 40 In addition to organizational commitment, professional and team commitment have also been identified. 41 Committed nurses are willing to exert effort for the organization, and their values align with the organization's values. 42 Generally, nurse managers are highly committed to their work. 43 However, it is known that the anxiety caused by the COVID-19 pandemic reduced the commitment of nurse managers and increased intentions to leave. 44 On the other hand, the connection between the perceived psychological safety of nurse managers and commitment has not been investigated previously. The subject holds importance due to the pivotal role nurse managers fulfil in the healthcare domain. Dedication to their responsibilities contributes to fostering stability within the workplace environment. Based on the literature mentioned above, we hypothesize that social support mediates the positive relation of psychological safety to commitment among nurse managers.
Aim
The aim of the present study was to test how social support mediates the effect of psychological safety on nurse managers’ commitment. Further research questions were: How does the perceived psychological safety differ between nurse managers and social and healthcare workers? How does perceived psychological safety differ by the background characteristics of nurse managers?
Methods
This was a cross-sectional study, reported following the STROBE checklist.
Sample and data collection
The data were collected through a Webropol online survey in January and February 2023 from members of a social and healthcare workers’ trade union. Participation was voluntary, and the survey link was distributed via a newsletter to approximately 100,000 Finnish-speaking union members. Two reminders were sent out. Out of the union members, 4573 individuals responded to the survey. This study included responses from nurse managers (n = 366) and social and healthcare workers (n = 4207), primarily nurses.
Instruments
Psychological safety was measured with four statements derived from the SCORE survey by Adair et al. 45 Psychological safety was described with the following statements: In this work environment… “I find it difficult to speak up if I notice problems in patient care,” “Staff find it easy to ask questions if they do not understand something,” “It is difficult to discuss mistakes,” and “My suggestions for improving quality are taken into consideration if I communicate them to the management.” Respondents evaluated statements on a 5-point Likert scale (1 = completely disagree, 2 = somewhat disagree, 3 = somewhat agree, somewhat disagree, 4 = somewhat agree, 5 = completely agree). Two of the statements were reverse-coded. A higher score indicated higher perceived psychological safety.
Commitment was measured with two questions: “How committed are you to your current job?” and “How committed are you to your current profession?” on a scale of 0‒10. Job and professional commitment were combined into a sum variable describing commitment. The social support variable was formed from the support provided by immediate supervisors and colleagues. The support provided by immediate supervisors was assessed with four statements: “My immediate supervisor cares about my well-being”; “My immediate supervisor helps and supports me”; “My immediate supervisor helps with the work”; and “My immediate supervisor succeeds in getting employees to work together.” The support provided by colleagues was assessed with the following three statements: “My colleagues are interested in me”; “My colleagues are friendly”; and “My colleagues help with the work.” Respondents assessed the statements on a 4-point Likert scale (4 = strongly agree, 3 = somewhat agree, 2 = somewhat disagree, 1 = strongly disagree). The total score was a mean of all the statements, and a low score indicated weak support, while a high score indicated strong support.
Data analysis
The normal distribution of the data was assessed using Kolmogorov–Smirnov and Shapiro–Wilk tests, which indicated that the data followed a normal distribution. The missing observation values were coded to match group means. Descriptive statistics were used to analyze participants’ background characteristics. An independent samples t-test was employed to investigate differences in perceived psychological safety between nurse managers and social and healthcare workers. The psychological safety levels were compared by nurse managers’ background characteristics using one-way analysis of variance (ANOVA) if the variable had more than two categories. As there are only two categories for the job level of nurse managers, the statistical difference between groups was examined using an independent samples t-test. The relationship between psychological safety, social support, and commitment of nurse managers was examined using Pearson's correlation coefficient. The mediation model was tested with Hayes’ PROCESS macro for SPSS. 46 Statistical significance was set at p < 0.05. Statistical analyses of the data were performed using SPSS software version 27.0.
Ethical considerations
The original data collection was conducted following Finnish legislation. Since it was an anonymous Internet survey without vulnerable participants and sensitive issues, it did not require ethical approval. The Institutional Review Board of the trade union granted permission for the study and distributed the survey to its members. Each participant in the study read a briefing stating that participation was voluntary and that responding was considered to be giving informed consent. Participants responded to the survey anonymously, and their identities were not disclosed to the researchers at any point. If desired, respondents had the option to discontinue their participation in the study before submitting the survey questionnaire. Participants had the opportunity to review the privacy policy if they wished to. The original data collected from the survey have been stored securely with password protection and have been handled with particular care. The Helsinki Declaration was taken into consideration in conducting the research. 47
Results
Of the respondents, 8% (n = 366) were nurse managers. Most managers (n = 332, 91%) worked as immediate supervisors, such as ward managers. About 8% (n = 30) of nurse managers worked at middle or senior management levels. Nearly all (n = 345, 95%) of the managers were women aged 26–67 years (mean 49.25, SD 9.33). Work experience varied from 6 months to 45 years (mean 17.00, SD 11.70). The most common highest educational attainment for nurse managers was a vocational or bachelor's degree, held by 56% (n = 205). A master's degree or higher had been obtained by 41% (n = 149) of nurse managers. The majority of nurse managers (n = 258, 71%) worked in the public sector, 26% (n = 94) in the private sector, and a minority, 3% (n = 12), worked in the third sector. Most nurse managers, 45% (n = 164), worked in health centers, residential or home care services. In the study, 40% (n = 143) of the participants worked in hospitals, while 8% (n = 30) worked as entrepreneurs or in private companies. In addition, 5% (n = 17) were employed in social services, and 2% (n = 7) worked in other areas, such as government or universities.
Nurse managers rated their psychological safety with a mean of 4.01 (SD 0.67), while social and healthcare workers rated it with a mean of 3.53 (SD 0.81) (Table 1). The difference in the total score for psychological safety between nurse managers and social and healthcare workers was statistically significant (p < 0.001), indicating that nurse managers’ perception of psychological safety is better across all aspects of psychological safety.
Perceived psychological safety of nurse managers (n = 364) and social and healthcare workers (n = 4178).
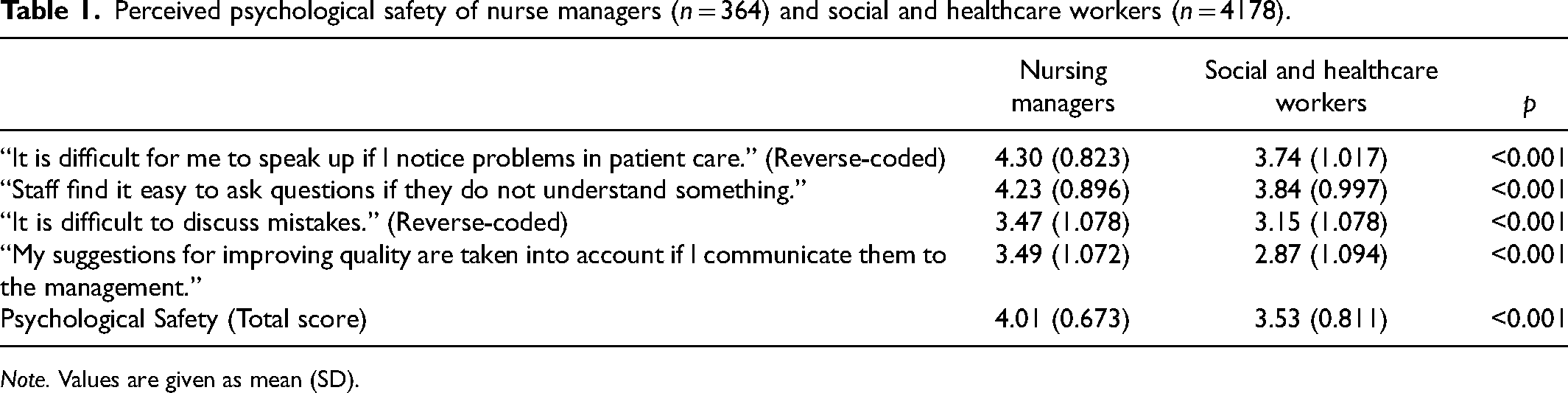
Note. Values are given as mean (SD).
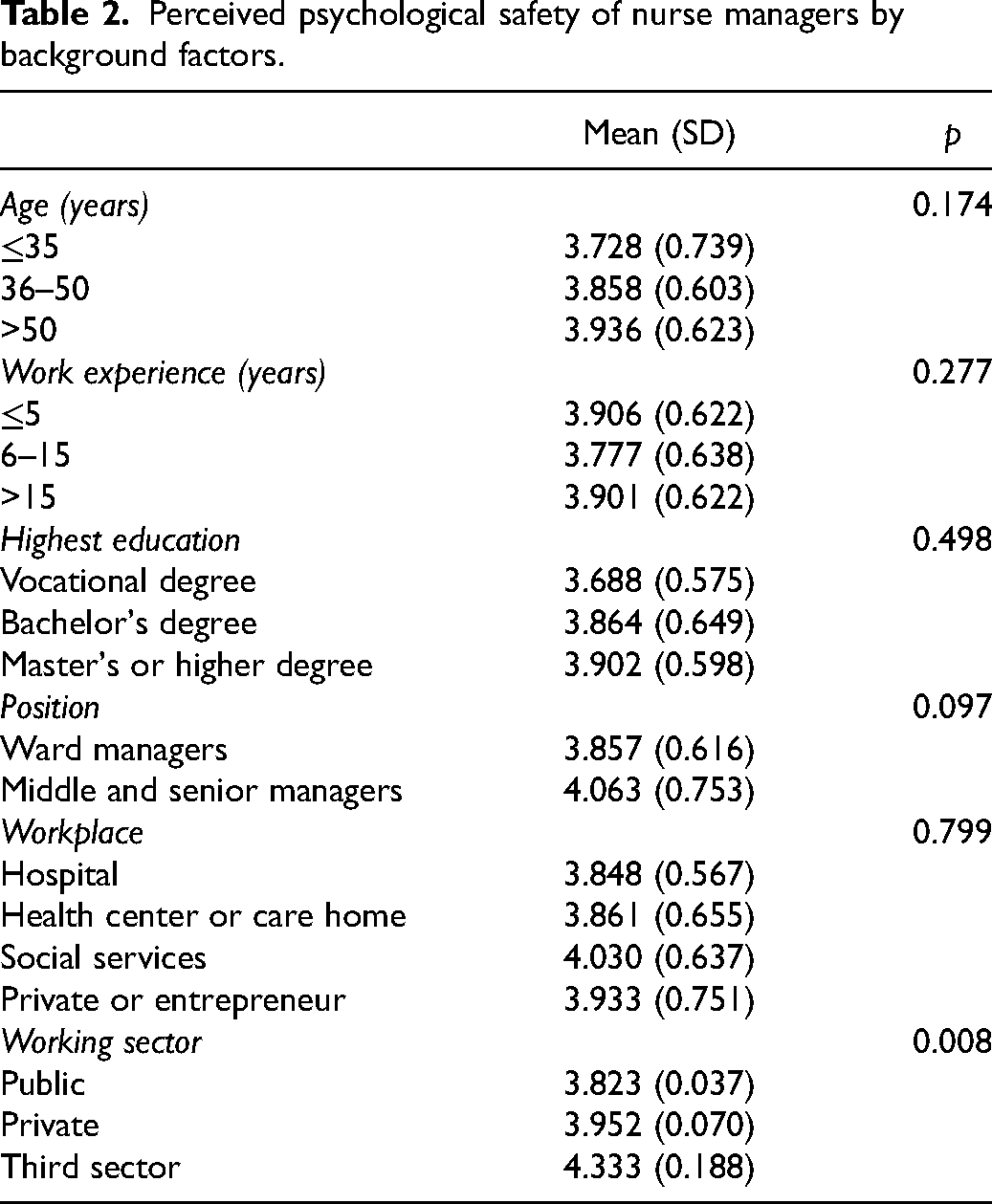
In the group of nurse managers aged over 51 years, the perceived psychological safety (3.94) was higher than in the younger age groups. The average psychological safety of ward managers was 3.86, whereas for middle and senior managers, it was 4.06. The highest reported psychological safety was among those working in social services (4.03). The lowest psychological safety was among those working elsewhere, such as in government or university (3.82). The psychological safety of nursing managers was lowest in the public sector (3.82) and highest in the third sector (4.33), and the difference was statistically significant (Table 2).
Perceived psychological safety of nurse managers by background factors.
Psychological safety, social support, and commitment were all statistically significantly related to each other (p < 0.001). The strongest correlation was between social support and commitment (r = 0.388), while the weakest was between psychological safety and commitment (r = 0.228) (Table 3).
Correlation coefficients between the study variables.
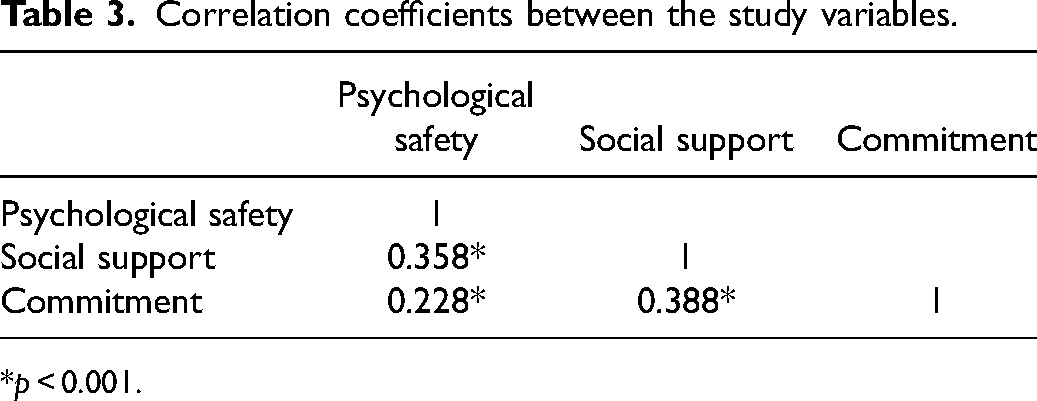
p < 0.001.
Social support acts as a mediator between psychological safety and commitment. The direct effect of psychological safety on commitment (β = 0.46) was statistically significant, and the total effect mediated by social support increased up to β = 0.99. In addition, psychological safety was significantly associated with social support (β = 0.44) and social support was significantly associated with commitment (β = 1.21) (Figure 1).
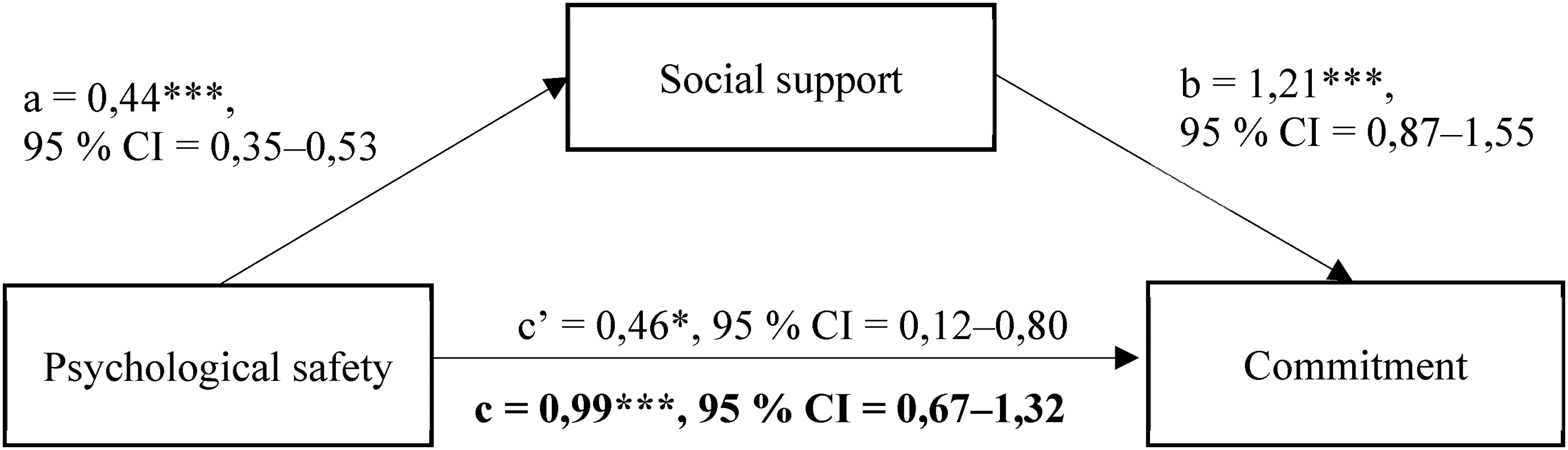
Conceptual and statistical model of the effects of psychological safety and social support on commitment among nurse managers. *p < 0.05, ***p < 0.001, c' = direct effect, c = total effect.
Discussion
This study investigated the psychological safety and associated workplace factors – commitment and social support – among nurse managers. It was found that psychological safety was significantly associated with the commitment of nurse managers, an association that, to our knowledge, has not been previously demonstrated. Furthermore, it was shown that social support is an important mediator by strengthening the relationship. Interestingly, nurse managers’ psychological safety was higher than that of social and healthcare workers, a finding that aligns with the results of Edmondson et al. 4 In the healthcare sector, employees who are closest to clients or patients often face significant expectations amid limited resources and top-down control. These employees frequently experience pressure, distress, and uncertainty, 4 diminishing their perception of psychological safety. Conversely, nurse managers typically engage less, if at all, in direct client work, with their roles being more focused on organization and administration. 48 This difference in roles and responsibilities may contribute to the observed disparity in psychological safety between these two groups.
This study revealed that the only background characteristic that significantly influenced nurse managers’ psychological safety was their employment sector. The reasons for the higher psychological safety of nurse managers in the third sector remain unclear. It can be speculated that the work pace in the third sector might be less intense than in the public sector, and there could be more autonomy over the work and its content. In addition, organizational structures in the third sector might be less hierarchical.
Previous research has suggested that individuals in higher organizational positions experience greater psychological safety. 4 Although this study found that nurse managers in higher-level managerial positions reported better psychological safety than immediate supervisors, the result was not statistically significant. This could be due to the relatively low number of respondents in middle and top-level leadership positions. Further research is needed to explore the impact of background characteristics on the manifestation of psychological safety. This will help deepen the understanding of the factors contributing to psychological safety in different workplace settings and roles.
Recently, the interplay between psychological safety, commitment, and social support has been observed in healthcare, even though not previously among nurse managers. The participative leadership style has been linked to psychological safety and commitment, as demonstrated by Qasim et al. 22 Furthermore, the role of social support from team members as a mediator for psychological safety has been highlighted. 9 Research conducted outside the healthcare context has identified social support and social capital as crucial elements for psychological safety at both team and organizational levels. The importance of rewarding relationships with colleagues and effective teamwork in fostering commitment and promoting psychological safety has been underscored by Newman et al. 7 In nursing, nurse managers are generally recognized for their commitment to work. 43 Moreover, psychological safety has been associated with reduced intentions to leave the job.12,35 This highlights the importance of these interconnected factors in maintaining a stable and committed workforce in healthcare settings.
The enhancement of psychological safety within organizations can be achieved through various initiatives such as reducing hierarchical structures, fostering openness, ensuring employee accessibility, and building trust. These measures have been found to increased team support and commitment.26,28,49 It is also imperative for leaders to receive adequate support from their supervisors. 50 Participative leadership styles19–21 and transformational leadership have been found to enhance psychological safety.23–25 Therefore, in the context of healthcare leadership, these styles should be prioritized to foster a psychologically safe environment, which can lead to increased team support and commitment.
Psychological safety and social support are factors that positively correlate with commitment. Existing literature has established a connection between psychological safety and reduced intentions to leave one's job or workplace.12,35 However, to our knowledge, the combined influence of psychological safety and social support on commitment has not been specifically examined within the healthcare sector despite general research on the relationship. 7 In the context of nursing, one of the responsibilities of a nurse manager is to provide support to the staff. 48 However, it is equally important for nurse managers to receive adequate support to effectively fulfil their roles. 50
Commitment plays a pivotal role in the healthcare sector. The World Health Organization (WHO) has projected a global shortage of 5.7 million nurses by 2030. 51 As per the data from Statistics Finland, 52 a significant proportion (76%) of chief nurses fall between the ages of 45‒74 years, with 37% aged 55‒64 years. These statistics indicate that many nurse managers are approaching the end of their professional careers. Therefore, to ensure the availability of committed managers in the healthcare sector, it is imperative to foster new leaders and maintain the commitment of current managers for an extended duration. Achieving this requires the creation of psychologically safe and supportive environments within organizations and teams. This approach not only aids in retaining existing staff but also attracts new talent, thereby addressing the shortage in the nursing workforce.
Strengths and limitations
The present study has several strengths and limitations. The research methodology employed in this study utilized validated measures, including those related to psychological safety. In the original study by Adair et al., 45 Cronbach's alpha (α) for the six-item Psychological Safety Scale was 0.8. In this study, a composite variable for psychological safety was created from the four statements, with a Cronbach's alpha (α) of 0.7. Variables describing commitment had a Cronbach’s alpha (α) of 0.76. Moreover, the social support questions were derived from the European Working Conditions Survey by the EU. Cronbach's alpha (α) for the social support composite variable was 0.85. Harman's single-factor test was conducted to examine common method variance (CMV). According to the test results, the first factor accounts for only 32.2% of the total variance in the data, indicating that the underlying assumptions were not met. No single common factor emerged, and the first factor did not account for the majority of the variance, indicating that CMV did not occur. 53
The data were collected in early 2023 from members of a largest Finnish social and healthcare workers’ trade union. These recent data encompass nurse managers working in various organizations across different regions in Finland. However, it is important to note that the results may not represent all Finnish nurse managers, as the survey was only distributed among union members. Despite this, it has been estimated that the rate of union membership, particularly among women in the healthcare sector, is high. 54 Given these factors, it can be cautiously concluded that the results provide an indicative snapshot of the situation of nurse managers in Finland in 2023. The primary limitation of this study is its cross-sectional design, which prevents the possibility of making causal inferences or drawing conclusions based on such relationships.
Conclusion
Social support and psychological safety are associated with the commitment of nurse managers. The future of healthcare will necessitate nurse managers who are deeply committed to their roles. Effective leadership has an impact on staff retention, and healthcare requires an adequate number of skilled workers to function. Enhancing the commitment of nurse managers can be achieved by fostering psychological safety and social support within work units. The significance of teamwork and peer support should be underscored in basic nursing and nursing leadership education. Learning environments should be designed to be psychologically safe, offering opportunities for growth in a secure and permissive setting with the backing of peers. Students accustomed to collaboration and mutual support during their studies are likely to be the ones who also provide assistance and support to others in the professional setting. Nursing leadership education should emphasize positive leadership approaches, such as participative and transformational leadership. In the future, it would be beneficial to explore the commitment of nurse managers through longitudinal research designs and intervention studies. This would provide a more comprehensive understanding of the dynamics of commitment in the nursing profession and inform strategies to enhance it.
Footnotes
Author contributions
MH, JH, and AH designed the study. MH collected the data. The data were analyzed by JH, MH, and all the authors participated in manuscript preparation. All the authors meet the criteria for authorship, and they have approved the content of the manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.