
Abstract
Maternal waiting homes (MWHs) are structures built near the healthcare facility, which aim to reduce the distance to accessing maternal health services and bring pregnant women closer to the health facility, near the time of delivery. This reduces the risk of pregnancy complications which can cause maternal and neonatal deaths, or low birth weight. Tsholotsho district adopted the use of Maternal waiting homes as there was an increase in pregnancy-related complications and incidents of maternal death. The study aimed to evaluate the effectiveness of maternity waiting homes in reducing pregnancy-related complications in Ward 5, Tsholotsho District. A 1:1 case-control study was used for the study, which recruited 248 women who attended Sipepa clinic. Data was collected using structured questionnaires and analysis for frequencies, means, proportions and odds ratios at 95% CI was done using SPSS version 29. The study established that Maternal waiting home use was a significant factor for reducing pregnancy complications (AOR = 0.16, 95% CI 0.09-0.28). Number of antenatal care visits less than 4 was found to be the significant independent risk factor for pregnancy complications (AOR = 2.9, 95% CI 1.3-6.2). The odds of adequate knowledge of the benefits of maternal waiting homes was 6.9 times higher among women who used MWHs than those who did not (OR = 6.9, 95% CI: 3.9-12.2). The study provides evidence that MWHs can significantly reduce pregnancy-related complications and improve maternal health outcomes in Sipepa, Tsholotsho. However, barriers to non-use of MWHs, such as lack of privacy, no food variety, and no cooking utensils, must be addressed to maximize the effectiveness of this intervention. There is a need for policymakers and healthcare providers to prioritize the implementation and expansion of MWHs in rural areas of Zimbabwe, where they can have the greatest impact on reducing maternal mortality and morbidity.
Introduction
Maternal waiting houses (MWHs) are vital to improving maternal and neonatal health outcomes in low-resource settings. These specially designed buildings are strategically located near healthcare centres, reducing the distance and barriers expectant mothers face when seeking obstetric care. 1 The primary objective of MWHs is to mitigate the risk of maternal complications and stillbirths among women living far from medical institutions. 2 Pregnant women who utilise MWHs are significantly less likely to experience pregnancy-related complications, with a remarkable 80% reduction in mortality rates. 3 Furthermore, the use of MWHs has been linked to a 73% decrease in stillbirths, highlighting the critical role these facilities play in supporting mothers’ and new-borns’ health and well-being. 4 MWHs can enhance health outcomes and save lives by providing a safe space for antenatal and postnatal care for pregnant women. 5
Globally, Maternal Mortality Ratio (MMR) was 158.8 deaths per 100 000 live births in 2021 compared to 157.1 deaths per 100 000 live births in 2020. 6 It is also unacceptably high as about 287 000 women died during and following pregnancy and childbirth in 2020. 5 By 2030, 390 women are expected to die giving birth in sub-Saharan Africa, more than five times higher than the 2030 Sustainable Development Goal of fewer than 70 maternal deaths per 100 000 live births. This figure is also significantly higher than the average of 13 deaths per 100 000 live births observed in Europe in 2017. 5 Zimbabwe’s MMR according to the 2022 housing and population census preliminary report is at 363 per 100 000 live births. 7 Furthermore, complications during pregnancy and childbirth were established to be the leading causes of death and disability among women of reproductive age (15-49 years) in Zimbabwe. 7 In Zimbabwe, the decline in pregnancy-related deaths from indirect causes can be attributed to a decrease in HIV and malaria-related fatalities among pregnant women during childbirth. Similarly, the decline in direct causes of pregnancy deaths is linked to a reduction in obstetric haemorrhage and infections related to pregnancy. 8
Studies on the effectiveness of maternity waiting homes (MWHs) have been conducted in various settings, primarily in resource-limited areas in Ethiopia. 4 A cross-sectional study found that MWH users had a significantly lower number of stillbirths and maternal deaths compared to non-users. 4 Additionally, a prospective cohort study found that MWH users had a lower incidence of adverse pregnancy outcomes, including perinatal death, low birth weight, and preterm birth. 9 Another study found that MWH users were more likely to undergo a caesarean section and had a lower risk of prolonged labour and post-partum haemorrhage. A systematic review and meta-analysis found that MWH users were 80% less likely to die and had a 73% lower occurrence of stillbirth compared to non-users. 10 Studies have suggested that MWHs can be an effective intervention to reduce maternal and perinatal mortality in resource-limited settings.4,9
Despite the efforts put in by the Government of Zimbabwe, to ensure that women overcome the delay of accessing health facilities through the introduction of waiting homes, pregnancy complication cases are still high in Ward 5, Tsholotsho district as shown by the district statistics as presented in Table 1. In a bid to reverse the worrying maternal mortality rates, the Result Based Program used the construction of maternal homes as an example of prioritising women’s health in Zimbabwe. 11 The national maternal mortality ratio is at 363 per 100 000 live births and Matabeleland North province stands at 366 per 100 000 as projected by the 2022 population and housing census preliminary results report. The greater parts of the district experience network challenges and the state of the roads is bad thus making it difficult to attend all maternal emergencies from 23 health care facilities. This prompted the adoption of maternal homes however; statistics show alarming trends of pregnancy-related complications including maternal death. While maternal waiting homes have been established to reduce delays in accessing healthcare, there is insufficient evidence on their actual effectiveness in lowering pregnancy-related complications specifically in Ward 5, Tsholotsho district. Therefore, this research aims to establish the extent at which the MWHs have influenced the reduction of maternal complications in Sipepa Ward 5, Tsholotsho District.
Pregnancy related complications in Ward 5, Tsholotsho District.

Source: Sipepa Rural Hospital records (2022).
Methods
Description of study area
The research was conducted in Sipepa in Ward 5 Tsholotsho District, in Matabeleland North Province, Zimbabwe. The district covers 7844 km2 with a population of 119 681 and a density of 16 persons/km2. Literature notes that Sipepa ward 5 has an estimated population of 4771 people (2267 are males and 2504 female), with 1161 households and an average household size of 4. 12 The study area map showing major healthcare facilities is shown in Figure 1.

Study area map of Tsholotsho with major healthcare facilities.
Study design
A 1:1 unmatched case-control study design was utilized to assess the effectiveness of waiting homes. This design compared two groups: those who gave birth without using waiting homes and those who gave birth after staying in waiting homes. An unmatched case-control study is a type of observational study often employed to examine factors associated with diseases or specific outcomes.
Target population and case definition
The target population for this study was all the women of childbearing age who had given birth at least once before data collection in Ward 5 between 2018 and 2022. According to the Zimbabwe 2022 Population and Housing Census preliminary report the district has 2504 females. 13
Inclusion criteria
The inclusion criteria were as follows:
(1) Pregnant women aged 15 to 49 years who gave birth between 2018 and 2022
(2) Women residing in Ward 5, Tsholotsho District.
Exclusion criteria
The exclusion criteria were as follows:
(1) Pregnant women residing outside Ward 5, Tsholotsho District.
(2) Women with pre-existing medical conditions that may complicate pregnancies
Case definition
(1) A case in this study was a woman of reproductive age from Ward 5, Sipepa, who gave birth and had maternal complications from the year 2018 to 2022
(2) A control was a woman of reproductive age from Ward 5, Sipepa, who gave birth and did not have maternal complications from the year 2018 to 2022
Dependent variable
The dependent variable for the study was maternal complication or no maternal complication.
Independent variables
The independent variables that were used in the study were measured as shown in Table 2:
Measurement of independent variables at Sipepa Rural Hospital.

Sampling technique
The study used a convenience sampling technique. The method enabled the researcher to sample from a larger population, selecting participants who met the inclusion criteria of cases and controls who visited the health care facility for any medical health service. A sample of 248 (124 cases and 124 controls) was sampled from a target population of 2504 females of childbearing age (ZIMSTAT12,13). The sample size was calculated using the Stat Calc tool in Epi Info 7.8.5, which used a two-sided confidence interval of 95% and 80% power. For the sample size calculation, estimates were based on the proportion of women who did not use maternal waiting homes and experienced pregnancy-related complications, specifically premature rupture of membranes, which was reported at 10.8% in a related study conducted in Ethiopia. 14 The Odds Ratio was 5.64 from the same research, hence it was adopted to calculate the sample size.
Data collection
A pre-tested structured questionnaire was used for the cases and controls to evaluate the effectiveness of Maternity waiting homes in reducing pregnancy related complications in ward 5, Tsholotsho District. A Kobo Collect Toolbox was used for data collection and storage as used by other authors for quantitative studies. 15 Kobo Collect Toolbox is a tool for collecting, managing, and analysing data in quantitative studies. 16 It is an offline mobile data collection platform that allows researchers to design, deploy, and manage surveys and other data collection instruments. 17 This data collection tool replaces the traditional way of collecting data by using mobile devices linked to a private online server only accessible by the researchers. The questionnaire comprised of three sections that is socio demographic characteristics, pregnancy related complications and factors influencing decisions and abilities to use MWHs. The tool was developed in English and then later translated to Ndebele and Shona.
Data analysis
The data collected using Kobo collect tool was exported to Statistical Package for the Social Sciences (SPSS) for further analysis from the administered questionnaires. Cross tabulations on socio-demographic characteristics and outcome of interest, (maternal complications) were done using chi-square odds ratios, and p values at 95% confidence intervals. Descriptive statistics on the nature of maternal complications was also done. A chi-squared test was used to check for an association between maternal waiting home use and maternal complications. These statistical analyses were done using SPSS at 95% CI. Logistic Regression Analysis was used for controlling confounders in this study by using several independent variables that could influence the outcome. In the same breadth, it was also used to adjust the odds ratio.
Results
Socio-demographic characteristics of study participants in Sipepa, Tsholotsho District
A total of 124 cases and 124 controls participated in the study. The median age of study participants was 29 years. Women who were aged 35 years and above were at a higher risk from maternal complications compared to those who were aged below 35 years (OR 1.5, CI (0.8-2.8)), however, this was statistically insignificant. Moreover, those who had children with an age gap of less than 18 months were 1.2 times more likely to have maternal complications compared to those with more than 18 months (95% CI 0.6-2.4). Other socio-demographic characteristics of the participants are presented in Table 3.
Cross tabulation between socio-demographic characteristics and outcome variable (maternal complications) of study participants in Sipepa, Tsholotsho District.

Maternal complications being experienced by pregnant women in ward 5, Tsholotsho District
The study assessed the frequency maternal complications in ward 5 Sipepa who were the cases. From the results in Table 4, 124 (50%) of the 248 study participants had pregnancy-related complications. The highest form of maternal complications was Antepartum haemorrhage which had 27 (10.9%) followed by obstructed labour (6.9%), while early separation of the placenta and low birth weight of the baby had the least frequency (2.4%). Use of the maternity waiting home by pregnant mothers was found to be 85% protective from maternal complications and was statistically significant (OR = 0.15, 95% CI 0.09-0.26) as shown in Table 5.
Maternal complications being experienced by pregnant women in ward 5, Tsholotsho District.

Association between maternity waiting home use and number of ANC visits with maternity complications by pregnant women in Ward 5 Sipepa.
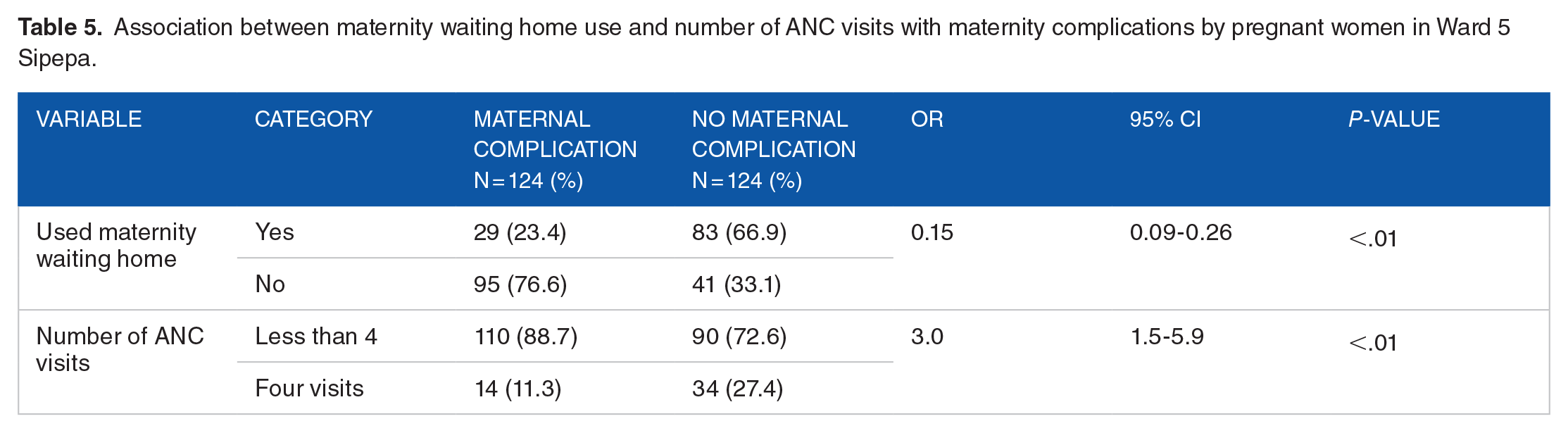
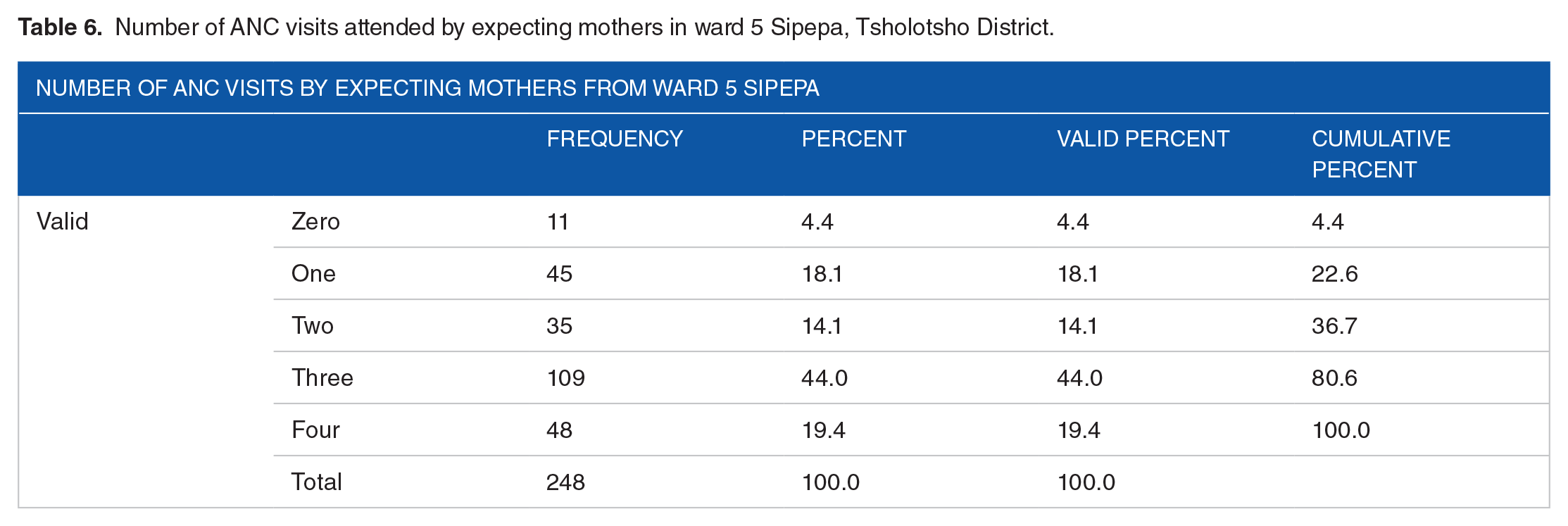
The study also assessed the frequency of Antenatal Care visits (ANC) of expecting mothers in ward 5 Sipepa as it influences maternal complications. The expected number of ANC visits by expecting mothers should be four before she gives birth. According to the results in Table 6, the highest frequency of ANC visits was three where 109 (44%) of the women attended while 11 (4.4%) did not attend any ANC visit. The study also established that those who had less than four ANC visits were three times more likely to have maternal complications compared to those who had at least four ANC visits. These findings are presented in Table 5.
Number of ANC visits attended by expecting mothers in ward 5 Sipepa, Tsholotsho District.
Factors influencing women’s decisions and abilities to use maternal waiting home
The study determined the factors influencing women’s decisions and abilities to use Maternal Waiting Home/s (MWH) in Sipepa.
Knowledge of the benefits of MWH by expecting mothers in Ward 5 Sipepa
The knowledge of the benefits of MWH by the 248 (100%) mothers from Sipepa was assessed. It was established that 100 (40%) of the women knew the benefits of MWH compared to 148 (60%). In addition, the odds of adequate knowledge of the benefits of MWHs was 6.9 times higher among women who used MWHs than those who did not (OR = 6.9, 95% CI: 3.9-12.2). These findings are presented in Table 7.
Knowledge of the benefits of MWH by expecting mothers in Ward 5 Sipepa.

Decision on the use of maternal waiting home
The study determined the decision-making for the use of the MWH, and it was established that 218 (87.9%) stated that they made individual decisions on the use of the facility, while 22 (8.9%) affirmed that they made the decision with their husbands or partners. However, 8 (3.2%) of the women said that it was their husbands or partners who made the decision to attend the facility.
History of maternal home use by mothers in Sipepa
The study established that 112 (45.2%) of the 248 women previously used the MWH before giving birth while 136 (54.8%) of the 248 women did not use the MWH before giving birth.
General condition of MWH used by pregnant mothers in Sipepa
The general condition of the MWH used by pregnant mothers in Sipepa was assessed as it influenced women’s decisions to use the MWH. 56 (22.6%) out of 112 (45.2%) of the women who previously used the MWH rated the general condition of the facility as fair, while 9 (3.6%) perceived the general condition of the MWH as poor. However, 47 (19%) of the women rated the general condition of the MWH as good.
Availability of adequate water supply at MWH in Sipepa
Availability of adequate water supply was one of the factors that influences women’s decisions to use the MWH. From the results, 96 (38.7%) out of 112 (45.2%) of the women who previously used the MWH reported that there was adequate water supply at the MWH, while 16 (6.5%) stated that there was no adequate water supply at the MWH as poor.
Availability of adequate lighting in MWH
Availability of lighting at the MWH was one of the environmental variables that was assessed for the study as it facilitates the use of the facility as it was one of the factors that influences women’s decisions to use the MWH. The study established that 72 (29%) out of 112 (45.2%) of the women who previously used the MWH at Sipepa reported that there was adequate natural and artificial lighting at the MWH, while 40 (16.1%) stated that there was no adequate lighting at the MWH.
Condition of sanitary facilities at MWH
Participants in the study were asked to evaluate the condition of the toilets at the Maternity Waiting Home (MWH), as this is a significant factor influencing women’s decisions to use the facility. The results revealed that 67 out of 112 women (approximately 27%) who previously utilized the MWH at Sipepa rated the condition of the toilets as good. In contrast, 15 women (about 6%) indicated that the sanitary facilities were in poor condition.
Separate bathing facilities for expecting mothers
The availability of separate bathing facilities for expecting mothers was another variable that was assessed as it influences the decision of women to use the MWH as it enables privacy. According to the results, 27 (10.9%) out of 112 (45.2%) of the women who previously used the MWH at Sipepa reported that the MWH had separate bathing facilities for expecting mothers, while 85 (34.3%) reported that the MWH did not have separate bathing facilities for expecting mothers.
Provision of bedding linen for expecting mothers at MWH
The availability of bedding linen for expecting mothers was another variable that was assessed as it influences the decision by women to use the MWH as it enables privacy. According to the results, 11 (4.4%) out of 112 (45.2%) of the women who previously used the MWH at Sipepa reported that there was provision of bedding linen at the MWH for expecting mothers, while 101 (40.7%) reported that there was no provision of bedding linen at MWH and they had to bring their personal linen.
Determinants of pregnancy-related complications in Sipepa
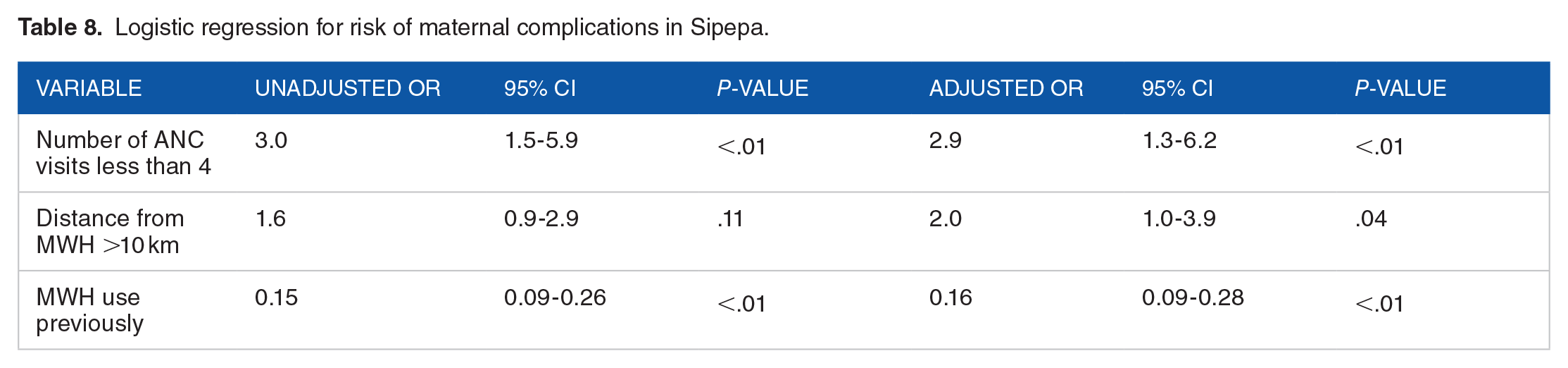
Forward stepwise logistic regression was used to determine independent risk factors for pregnancy complications in ward 5, Sipepa. Also, it was done to control confounding variables and show effect modification. The variables which were put into the model to predict the outcome variable which was pregnancy or non-pregnancy complications were; age in years, marital status, distance from clinic, highest level of education, age gap between first and last born, number of ANC visits and use of maternal waiting home previously. Variables that were eliminated by the model were; age in years, marital status, highest education level and age gap between first and last-born. The significant independent risk factor for pregnancy complications were Number of ANC visits less than 4 (AOR = 2.9, 95% CI 1.3-6.2). Distance from the MWH of more-than 10 km was included in the model, however, it was not significant as the confidence interval includes one. Maternal waiting home use was a significant independent risk factor for reducing pregnancy complications as it was 84% protective (AOR = 0.16, 95% CI 0.09-0.28). The results are shown in Table 8.
Logistic regression for risk of maternal complications in Sipepa.
Discussion
Women in Sipepa, in Tsholotsho district, saw distance from the MWH facility as a contributory factor to utilisation of MWH. Those who lived near the clinic (distance of less than 5 km) did not use the MWH as they thought that they can safely arrive in time for delivery and that it was beneficial to those women who stay more than 10 km from the facility. This was consistent with findings by other scholars who found out that pregnant women who had more travelling time due to distance from their place of residence to the health care for maternity health services were more likely to use MWH services unlike those who stay nearby. 10 Moreover, pregnant women who live further away or take time to travel to the health facility are at a higher risk of adverse birth outcomes such as low-birth weight. 18 Due to financial challenges faced by some women and the condition of the Maternal Waiting Homes (MWHs), not all women are likely to use them, which increases the risk of pregnancy-related complications.
The study findings revealed that the number of Antenatal care (ANC) visits less than four were significantly associated with pregnancy-related complications in Sipepa. The study findings demonstrate a strong link between ANC attendance and reduced risks of pregnancy-related complications. This finding was also consistent with one by Kassa et al, 10 who established in their study that attending ANC was significantly associated with utilising MWHs and also reducing the risk of pregnancy-related complications. Non-attendance of ANC visits could have increased the risk of pregnancy-related complications as women in the study made most of the decisions by themselves. The study reported less involvement of their husbands or male partners who would not come with them to the ANC clinics. Healthcare providers should prioritize increasing male involvement in ANC, through strategies such as educating men about the importance of ANC and involving them in the decision-making process. Healthcare providers should also consider providing alternative ANC services that are more convenient and accessible for women, such as mobile ANC services or ANC services that can be conducted at home, to reduce the barriers to attendance.
Use of the maternal waiting home in Ward 5 Sipepa was significantly protective in lowering the risk of pregnancy-related complications in the study setting. This implies that the intervention is effective if it is used by women of childbearing age. However, the effectiveness of the intervention is affected by socio-demographic, religious and cultural factors presented in the study results. The study results were consistent with those found by Dadi et al, 9 who also found that the use of MWH in developing countries significantly reduces the risk of pregnancy-related complications by 77% and 80% respectively compared to non-users. The study findings revealed that maternal complications in the ward 5 Sipepa was found to be lower than that of the national data as reported by Lokken et al, 19 who established that the pooled prevalence for gestational hypertension in Zimbabwe was 16.5% (95% CI 6.5-29.9). Although it was lower compared to the national prevalence, it remains a public health issue of concern as there could be some women who fail to have access to the maternal health facility due to reasons such as lack of money to travel, hence putting their life and that of the unborn child at risk to maternal and neonatal death. The findings from the study were contrary to those found by Semasaka Sengoma et al, 20 who found that Pre-eclampsia or eclampsia, postpartum haemorrhage and prolonged labour and dystocia were accountable to pregnancy complications of study participants in a health facility study done in Rwanda, yet the highest frequency of pregnancy-related complications in Sipepa was antepartum haemorrhage.
The study established that the odds of adequate knowledge of the benefits of MWHs were higher among women who used MWHs than those who did not. Other studies also reported that the odds of adequate knowledge of the MWHs was higher (AOR = 5.13; 95% CI: 3.60-7.30) among women and influenced them to use the facility. 21 There is also evidence that shows that women’s decisions were an important factor in MWH utilisation 22 and in turn, has a significant effect on the knowledge of women about MWHs. 21 Healthcare providers must prioritize educating women about the benefits of using MWHs, particularly those who are at risk of pregnancy-related complications. This can be done through community-based programs, social media campaigns, and other outreach initiatives.
The study findings revealed that food adequacy influenced utilisation of the MWH. Some women were reported not to prefer MWH because they would not be able to go to the facility as they could not share the little food, they had with their families. Lack of privacy was also reported to influence use of MWH, women revealed that they could not bring their husbands to stay with them at the facility because bathing facilities were not separate. These findings were consistent with other literature which reported that factors that deter women from utilising the MWHs were lack of food supplies and poor infrastructure.23,24 Kapesa, 25 and Sialubanje et al, 26 reported that lack of privacy for the women to stay with their partners and lack of cooking utensils made the intervention ineffective due to low utilisation by the women. A private and comfortable environment helps to reduce stress and anxiety, which are known factors to exacerbate pregnancy-related complications.
Lack of money to travel and to pay for food and user fees to access MWHs was seen as a barrier to utilising MWHs, therefore women would go to deliver to the clinic when they are due instead of going to the MWH. The majority of women in this study had a monthly income of less than 50 USD, which is below the poverty datum line. These findings were also found by Sialubanje et al 26 who also found that some women in rural Zambia were having challenges with accessing MWHs due to financial constraints hence not utilising the facility and exposing themselves to the risk of pregnancy-related complications. Similarly, a study by Kurji et al, 4 found that costs incurred in transport, purchase of food and accommodating accompanying relatives made some not to use MWHs. However, these findings contradict to the Zimbabwean policy on maternal waiting homes. The maternity waiting homes are financed by the Results Based Finance Programme in Zimbabwe, which has a mandate to reverse the terrible trend of maternal mortality due to pregnancy complications. 11
Limitations
The study design used was a case-control, which made it difficult to establish the temporal sequence of events. Therefore, it was difficult to ascertain whether non-utilisation of MWHs was the cause for pregnancy-related complications. There was also a possibility of recall bias by the study participants considering the time lapsed when they gave birth, hence giving information that would overestimate or underestimate the strength of association in some variables. In addition, the study did not use key informants to give more information on the contributory factors for the utilisation of maternity waiting home and the pregnancy-related complications. The study specifically examined women of childbearing age living in a rural area. Therefore, the findings may not be directly applicable to urban populations or regions with different healthcare infrastructures. Additionally, the cultural and social factors influencing maternal health in the Tsholotsho District may vary from those in other regions.
Conclusions
Maternity waiting homes effectively reduced the risk of pregnancy-related complications, as the association was statistically significant. Factors that increased the risk of pregnancy complications were the number of ANC visits less than four and distance of more than 10 km. In addition, the maternity waiting homes were not equipped fully with cooking utensils; there was limited privacy and inadequate variety of food. Women using maternity health services, especially those living further away from the health facility should be given sufficient money from the donor to attend MWH. The MWH should have a variety of food apart from nutrition gardens to enable women who will be waiting to deliver to stay there. Male partner involvement is also crucial hence; health promotion should be intensified on the importance of pregnant women to seek appropriate maternal health care to reduce the risk of pregnancy-related complications, which may lead to maternal and neonatal deaths. The findings of this study provide valuable insights into the effectiveness of maternal waiting homes in reducing pregnancy-related complications within Sipepa Ward 5, Tsholotsho District. However, the generalizability of these results may be influenced by several factors. The study focused specifically on women of childbearing age residing in a rural context. As such, the findings may not be directly applicable to urban populations or regions with different healthcare infrastructures. The cultural and social factors influencing maternal health in Tsholotsho District may differ from those in other regions. Therefore, while the results are relevant to similar rural settings. In conclusion, while the study offers important evidence regarding the role of maternal waiting homes in improving maternal health outcomes, further research in diverse settings and populations is necessary to enhance the generalizability of these findings. Future studies should consider longitudinal designs and multi-site approaches to validate and extend the results across different contexts.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
SN conceptualised the research idea and drafted the manuscript. PLM and MWM coordinated the manuscript writing process, guided the manuscript writing process and revised the draft manuscript. All the authors read and approved the manuscript.
Author Information’s
SN is a BSc Public Health student at the National University of Science and Technology in Zimbabwe. This paper was part of the research project that was partial fulfilment of the BSc in Public Health. PLM is a Master of Science Degree in Environmental Health holder at the National University of Science and Technology in Zimbabwe. The Author is a Lecturer in the Department of Environmental Health in the Faculty of Environmental Science at the National University of Science and Technology. MWM is an MSc Epidemiology and Biostatistics holder at Midlands State University. The author is also a Lecturer in the Department of Environmental Health in the Faculty of Environmental Science at the National University of Science and Technology. PLM and MWM co-supervised the student.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the National University Science and Technology’s department of Environmental Health. Permission to proceed was sought from the District Medical officer in Tsholotsho. Informed written consent was obtained from the study participants to whom the research objectives, procedure, and benefits were explained. The written consent form was given to the participants to read and sign. Confidentiality and anonymity was maintained throughout the study. No names or any form of identity were required from the respondents. Participants had the right to withdraw from the study at any stage if they no longer feel comfortable to proceed.