
Abstract
Background:
While the importance of women’s participation in household decision making in enhancing access to healthcare services is widely acknowledged, limited evidence exists on the link between women’s participation in household decision making and skilled birth attendants (SBA) supervised delivery. This study aims to fill this gap by examining the effects of women’s participation in household decision making on SBA supervised delivery in Bangladesh.
Methods:
Data of 3607 mothers who had given birth within 2 years of the survey date were extracted from the 2022 Bangladesh Demographic and Health Survey (BDHS) and analyzed. The outcome variable considered was SBA supervised delivery, and the primary explanatory variable was a composite index of women’s participation in household decision making generated from their responses regarding decision-making on own healthcare, large household purchases, and visits to their family or relatives. Multi-level mixed-effects logistic regression was used to explore the effects of women’s participation in household decision making on SBA supervised delivery, adjusted for potential confounders.
Results:
The reported prevalence of SBA supervised delivery was 70%. Women lacking participation power and moderately empowerment in household decision-making were 15% (aOR= 0.85, 95% CI: 0.66-1.08) and 20% less likely to had SBA supervised delivery (aOR = 0.80, 95% CI: 0.64-0.99) compared to those with high participation power, respectively. This association remained consistent across all 3 empowerment domains, with lower likelihoods of SBA supervised delivery among women lacking empowerment.
Conclusion:
The findings of this research affirm the positive effects of women’s participation in household decision making on SBA supervised delivery in Bangladesh. Recommendations include increasing women’s empowerment in household decision making and raising awareness and education about the importance of SBA supervised delivery.
Keywords
Introduction
Maternal mortality continues to be a significant global concern, with 287 000 women succumbing to pregnancy-related causes each year. 1 Additionally, 5.4 million children under the age of 5 perish due to preventable reasons, primarily within their first year of life.2,3 The majority of these fatalities occur in low- and middle-income countries (LMICs), placing the heaviest burden on Asian and African nations.1,2 Notably, despite the commendable efforts invested in reducing adverse maternal and child health outcomes during the implementation of the Millenium Development Goals from 2000 to 2015, the prevalence of maternal and child mortality in LMICs persists. Although considerable strides were made, particularly in increasing the uptake of maternal healthcare services such as antenatal, delivery, and post-natal care, success remains modest. 4 Recent evidence reveals that nearly half of deliveries in LMICs lack supervision by skilled healthcare personnel. The complexities underlying this issue are multifaceted, involving factors such as women’s socio-demographic and household characteristics, rural settings, and entrenched social norms.5-7 To address this challenge, the global community has committed to enhancing the uptake of maternal healthcare services, including delivery services, with the aim of achieving universal coverage by 2030, as part of the Sustainable Development Goals. 8
Women’s empowerment in household decision making autonomy plays a pivotal role in shaping healthcare utilization, particularly in the realm of delivery services. 9 Empowered women, equipped with knowledge, autonomy, and decision-making authority regarding their health, are more likely to actively engage with and prioritize maternal healthcare services.9,10 They seek and access antenatal, delivery, and post-natal care, recognizing the crucial role these services play in their well-being and that of their children.9,11 Additionally, empowerment contributes to dismantling barriers associated with traditional norms and societal expectations, fostering a mindset that values and prioritizes women’s health.12,13 As women gain control over reproductive choices and health-related decisions, they navigate healthcare systems more effectively, ensuring timely and adequate care during pregnancy and childbirth.14,15 The connection between women’s empowerment in household decision making and skilled birth attendance (SBA) supervised delivery becomes a critical avenue for addressing maternal and child health challenges, positively impacting both individual well-being and broader community health outcomes. However, studies on this issue are limited in LMICs and insufficient in the context of Bangladesh.16-21 The inconclusive nature of existing research can be attributed to variations in women’s empowerment indicators, small sample sizes collected at the regional level, and imprecise analytical techniques. Furthermore, diverse norms regarding the SBA supervised delivery across countries underscore the need for context-specific understanding. Thus, this study aims to explore the association between women’s participation in household decision making and SBA supervised delivery in Bangladesh.
Methods
Study design and sampling technique
We conducted an analysis using nationally representative households survey data extracted from the 2022 Bangladesh Demographic and Health Survey (BDHS). This survey was conducted by the National Institute of Population Research and Training (NIPORT) as part of the Demographic and Health Survey Program of the USA, supervised by the Ministry of Health and Family Welfare of Bangladesh. Employing a multi-stage stratified sampling method, nationally representative households were selected in 2 stages. Initially, 675 clusters (237 in urban areas and 438 in rural areas) were randomly chosen from a list of 296718 clusters in Bangladesh, based on the 2011 National Population Census conducted by the Bangladesh Bureau of Statistics. Of them, data were collected from 674 clusters, with one remaining cluster excluded due to security concerns located in Cos’x Bazar, Chattogram. In the second stage, an average of 45 households per cluster were selected through systematic random sampling, totaling 30 330 households with 30 358 eligible reproductive-aged women (15-49 years). The eligibility criteria required women to be formally married and usual residents of the selected households or have spent the most recent night in the household before the survey. The survey excluded unpartnered women (those who have children without a formal partner) as such cases are rarely reported in Bangladesh due to cultural prohibitions. Among these women, data were collected from 30 078 with a response rate of 99.1%. The details procedure of this survey has been published elsewhere. 22
Analytical sample
We analyzed data of 3607 women extracted from the main survey. The sample was selected based on specific inclusion criteria: (i) women of reproductive age who reported at least 1 live birth within 2 years of the survey, (ii) women who reported details information about the individuals assisting them during delivery, and (iii) women for whom data on women’s empowerment regarding household decision making autonomy were available.
Outcome variable
The outcome variable in this study was SBA supervised delivery. Women were queried about the providers of delivery healthcare services, asking, “Who assisted the delivery of (NAME)?” The response choices included various healthcare providers, such as qualified doctors, nurses, midwives, paramedics, family welfare visitors, community skilled birth attendants, sub-assistant community medical officers, community healthcare providers, family welfare assistants, trained traditional birth attendants (TBAs), untrained TBAs, etc. We categorized these responses to generate a dichotomous variable on SBA supervised delivery. According to the definition of BDHS, SBA was defined who reported births were supported by qualified doctors, nurses, midwives, or paramedics; family welfare visitors (FWVs); community skilled birth attendants (CSBAs); and sub-assistant community medical officers (SACMOs) and coded as “1,” otherwise defined as unskilled birth attendants and coded as “0”. 22
Explanatory variable
The primary explanatory variable in this study was women’s empowerment regarding the participation in household decision making autonomy. We derived this variable from women’s responses regarding their participation in own healthcare decision-making, significant household purchases, and visits to their families or relatives’ homes. To gather data on their involvement, women were posed with the following questions: “Who usually makes decisions about making major household purchases?” and “Who usually makes decisions about health care for yourself?” Additionally, they were asked, “Who usually makes decisions about visits to family or relatives?” Women provided responses choosing from options such as respondent alone, husband alone, respondent and husband jointly, someone else, or others. We reclassified these responses as “not empowered” if women did not make decisions by sloely alone or jointly with husband in any of the 3 areas mentioned, “moderately empowered” if they reported involvement either alone or jointly with husband in at least 1 of the 3, and “highly empowered” if they reported participation in all 3 areas either alone or jointly with husband.
Potential confounders
Several potential confounding variables were incorporated in the examination of the association of the outcome variable with explanatory variables. The selection of these factors was identified by a thorough review of previous literature from Bangladesh and other LMICs.9,12,23-25 These chosen variables were subsequently categorized into individual, household, and community-level factors. Individual-level factors encompassed mother’s age at birth (⩽19, 20-34, and ⩾35 years), education (no formal education, primary, secondary, and higher), employment status (no/yes), antenatal care visits from medically trained providers (no visits, 1-3 visits, and 4 and more visits), number of total children ever born (1-2 children, >2 children), and exposure to mass media (not exposed, moderately exposed, and highly exposed). At the household level, factors included partner’s education (no formal education, primary, secondary, and higher), occupation (agricultural worker, non-agricultural worker, services, business, and others), and household wealth status (poorest, poorer, middle, richer, and richest). Major community-level factors considered were place of residence (urban or rural) and administrative divisions (Barishal, Chattogram, Dhaka, Khulna, Rajshahi, Rangpur, and Sylhet).
Statistical analysis
Descriptive statistics were employed to summarize the characteristics of the respondents. Multi-level mixed-effects logistic regression were utilized to assess the association between the explanatory and outcome variables, adjusting for confounding factors. The rationale for employing multi-level regression models stemmed from the hierarchical structure of the data, where individuals were nested within households, and households were nested within clusters. Previous studies have indicated that a simple logistic regression model yields less accurate findings in such hierarchical data compared to a multilevel model. 26 A total of 5 models were run. The initial model, referred to as the null model, solely included the variable for SBA supervised delivery. In Model 2, the analysis incorporated individual-level variables along with women’s empowerment. Models 3 and 4 integrated women’s empowerment with household and community-level factors, respectively. Model 5 represents the comprehensive model where all variables were simultaneously considered. Multicollinearity checked before running each model. Variables showing multicollinearity were excluded from the model. Sampling weight was considered in all analyses. Results were reported as odds ratios (ORs) with their corresponding 95% confidence intervals (CIs). Statistical analyses were conducted using Stata (version 17.0).
Results
Background characteristics of the respondents
Table 1 presents the background characteristics of the respondents. A significant portion, 71% of the total sampled mother, were aged between 20 and 34 years at the time of their most recent births. Approximately half of the respondents had completed secondary-level education. Of the total respondents, 38.4% received 4 or more antenatal care services from medically trained providers. Nearly 72% of the mother’s had 1 to 2 children at the time of the survey. Regarding exposure to mass media, 43.5% reported no exposure to any form of mass media. In terms of household wealth status, 20.1% of the respondents belonged to the poorest wealth quintile. Geographically, approximately 73.2% of the total mother’s resided in rural areas. Moreover, 25.1% of the respondents reported living in Dhaka as their administrative division.
Background characteristics of the respondents, BDHS, 2022 (N = 3607).

Women’s empowerment regarding participation in household decision making in Bangladesh and the SBA supervised delivery across various empowerment indicators
Table 2 presents the distribution of women’s participation in household decision making autonomy indicators. Approximately 7.6% of women reported making sole decisions for own healthcare services uptake, 2.4% for significant household purchases, and 5.1% for visits to family or relatives. When considering all 3 indicators collectively, 54.8% of women were classified as highly empowered in major household decisions, followed by 26.5% as moderately empowered, and 18.7% as not empowered. The uptake of SBA-supervised delivery was reported by 69.9%. This percentage decreased to 65.3% among women who lacked decision-making autonomy either alone or jointly with husband in all 3 aspects of the household decisions (Table 3).
Distribution of mothers’ empowerment indicators in Bangladesh.

Distribution of SBA supervised delivery across mothers’ empowerment indicators in Bangladesh.

Presented row percentages.
SBA supervised delivery and its distribution across mother’s individual, household, and community-level factors
Table 4 presents the percentage of SBA supervised delivery across mother’s individual, household, and community-level factors. The highest prevalence of SBA supervised delivery was 71.1 (95% CI: 67.4-74.6) among mother’s aged ⩽ 19 years at birth. The utilization of SBA supervised delivery was notably higher among mother who received 4 or more antenatal care services (85.7%). Conversely, utilization of SBA supervised delivery was lower among mother with no formal education, while the highest rates were observed among those with higher education. Among the total sampled mothers, those whose husbands had higher-level education and were employed in services exhibited a higher utilization of SBA supervised delivery services uptake. Furthermore, mother’s residing in wealthier households and urban areas demonstrated a higher rate of SBA uptake.
Skilled birth attendant supervised delivery across mothers’ individual, household, and community level factors, BDHS, 2022 (N = 3607).

Presented as row percentages. P-values are obtained from Pearson Chi-square test.
Association between women’s empowerment regarding the participation in household decision making and SBA supervised delivery in Bangladesh
The results of the multi-level mixed-effects logistic regression, examining the association between the women’s participation in household decision making index and the uptake of SBA while adjusting for individual, household, and community-level factors, are detailed in Table 5. The association between indicators of women’s participation in major household decisions and SBA supervised delivery is presented in Supplemental Table 1. We ran a total of 5 models to explore the association between outcome and explanatory variables, and the best model was determined based on the lowest values of ICC, AIC, and BIC. The full model met these conditions, with the ICC of the null model at 28.78%, reducing to 12.71% in the full model after accounting for individual, household, and community-level factors.
Multilevel mixed-effects logistics regression assessing the association between women’s participation in household decision making autonomy and uptake of SBA in Bangladesh, 2022.
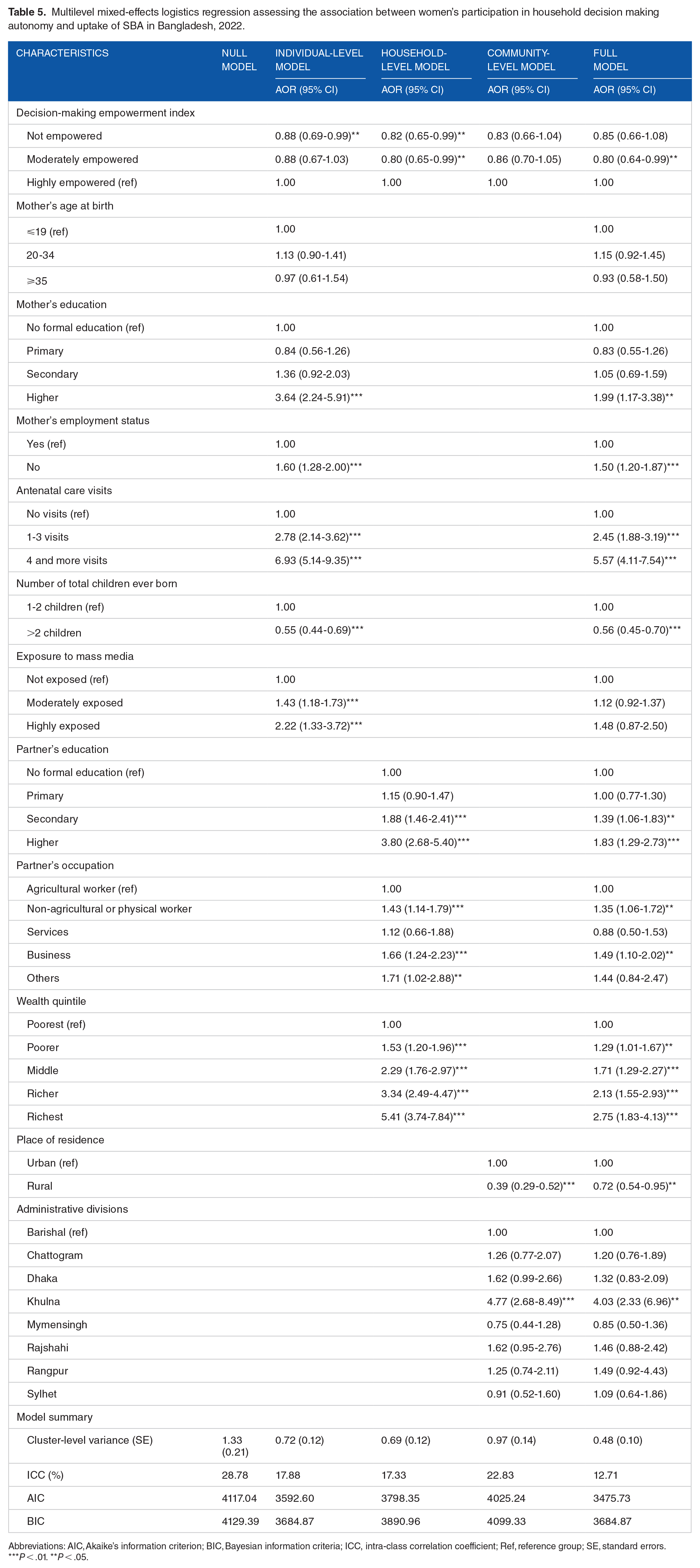
Abbreviations: AIC, Akaike’s information criterion; BIC, Bayesian information criteria; ICC, intra-class correlation coefficient; Ref, reference group; SE, standard errors.
P < .01. **P < .05.
The full model analysis revealed several significant findings. Moderately empowered individuals had a lower likelihood of SBA supervised delivery (aOR: 0.80, 95% CI: 0.64-0.99) compared to those who were highly empowered. In terms of maternal education, mothers with higher education had a significantly increased likelihood of SBA supervised delivery (aOR: 1.99, 95% CI: 1.17-3.38) compared to those with no formal education. Unemployed mothers showed higher odds of SBA supervised delivery (aOR: 1.50, 95% CI: 1.20-1.87) compared to employed mothers. Antenatal care visits were strongly associated with increased odds; mothers with 1 to 3 visits had an aOR of 2.45 (95% CI: 1.88-3.19), and those with 4 or more visits had an aOR of 5.57 (95% CI: 4.11-7.54) of SBA supervised delivery, compared to those with no visits. Mothers with more than 2 children had lower odds of SBA supervised delivery (aOR: 0.56, 95% CI: 0.45-0.70) compared to those with 1 to 2 children. For partner’s education, those with secondary education (aOR: 1.39, 95% CI: 1.06-1.83) and higher education (aOR: 1.83, 95% CI: 1.29-2.73) had significantly increased odds of SBA supervised delivery compared to those with no formal education. Partners working in non-agricultural or physical labor (aOR: 1.35, 95% CI: 1.06-1.72) and business (aOR: 1.49, 95% CI: 1.10-2.02) had higher odds of SBA supervised delivery compared to agricultural workers. Wealth quintile analysis showed a gradient effect, with poorer (aOR: 1.29, 95% CI: 1.01-1.67), middle (aOR: 1.71, 95% CI: 1.29-2.27), richer (aOR: 2.13, 95% CI: 1.55-2.93), and richest (aOR: 2.75, 95% CI: 1.83-4.13) households having significantly higher odds of SBA supervised delivery compared to the poorest households. Rural residence was associated with lower odds of SBA supervised delivery (aOR: 0.72, 95% CI: 0.54-0.95) compared to urban residents. Among administrative divisions, mothers from Khulna had significantly higher odds of SBA supervised delivery (aOR: 4.03, 95% CI: 2.33-6.96) compared to those from Barishal.
Upon analyzing the individual components of the composite index for mothers’ participation in household decision-making autonomy, we found that mothers who made healthcare decisions jointly with their husbands had a 1.20 times higher likelihood (95% CI: 1.01-1.47) of utilizing SBA-supervised delivery compared to those whose healthcare decisions were made solely by their husbands or other relatives (Supplemental Table 1). Similarly, mothers who independently made decisions on large household purchases had a 1.05 times higher likelihood (95% CI: 1.09-1.90), and those who decided on visits to family or relatives on their own showed a 1.22 times higher likelihood (95% CI: 1.19-2.63) of utilizing SBA-supervised delivery compared to their counterparts.
Discussion
This study explored the association between mothers’ empowerment regarding their participation in household decision making autonomy and SBA supervised delivery in Bangladesh. We found that 70% of the total mother’s in Bangladesh uptake SBA supervised delivery services, which was observed to decrease to 65.3% among mother’s lacking decision-making autonomy in all 3 aspects of the household decisions, namely decisions on large household purchases, own healthcare and visits to family or relatives. We found that mothers who had made all their decisions either alone or jointly with their husband had a higher likelihood of uptaking SBA supervised delivery services. These findings are robust as they are derived from a nationally representative survey with substantial sample sizes and have been adjusted for a wide array of covariates. The outcomes underscore the fact that mothers with no decision-making autonomy in Bangladesh exhibit lower utilization of SBA supervised delivery services. This inability to make decisions on the uptake of SBA supervised delivery places an immense burden on mothers, particularly increasing the risk of adverse maternal and child health outcomes, including maternal and child mortality.
We found that around 28% of highly empowered mothers did not utilize SBA-supervised delivery services. However, when calculating likelihoods, mothers lacking decision-making autonomy were significantly less likely to use SBA services, aligning with findings from previous studies in LMICs and Bangladesh.15,27-30 While the reasons for mothers without decision-making autonomy not accessing SBA services are clear, the lower uptake among highly empowered mothers may be attributed to social norms and family restrictions.31,32 Mothers without decision-making empowerment in LMICs, including Bangladesh, face various barriers to accessing maternal healthcare services, such as lower awareness about the importance of SBA services uptake and misconceptions.31,32 These barriers are notably higher among illiterate mothers with poor economic status and rural mothers, consistent with the findings of this study and other available research.9,31,33 Furthermore, these barriers impede their empowerment, leaving them uninformed about the significance of reproductive healthcare, which, in turn, hinders their utilization of maternal healthcare services, including the uptake of SBA supervised delivery services. 25 Additionally, socio-demographic factors and educational limitations of mothers without decision-making autonomy restrict their mobility and ability to access maternal delivery healthcare services. 34
Mothers lacking formal employment status were found to be more likely to report the uptake of SBA supervised delivery services—a finding opposite to previous studies in LMICs and Bangladesh.12,18,21 The reasons for such an association are difficult to explain; however, it is plausible that mothers in informal employment settings benefit from robust informal support networks, community-based interventions, and cultural norms that prioritize maternal health. 18 Additionally, the accessibility and availability of healthcare services, as well as targeted health education initiatives, may play pivotal roles in influencing the health-seeking behavior of mothers without formal employment. 30 Government policies and interventions addressing maternal healthcare might have specifically targeted this demographic, contributing to the observed trend. 20 Nevertheless, the unexpected findings necessitate comprehensive and context-specific research methodologies to unravel the nuanced factors shaping this association and the multi-faceted determinants influencing such associations in diverse socio-economic contexts.
Moreover, we observed a higher likelihood of SBA services among mothers whose husbands were employed in business holders. This finding could be attributed to several reasons. Firstly, husbands in businiss may have better economic stability, providing families with the financial means to afford SBA during delivery. Additionally, such husbands may have access to information and resources that enable them to prioritize and advocate for their wives’ reproductive health. Furthermore, business-sector employment often correlates with higher education levels, and educated husbands are more likely to understand the importance of delivery care aided by SBA supervised delivery and encourage their wives to seek such services.
We observed positive influential effects of antenatal healthcare services uptake on the utilization of delivery healthcare services aided by SBA, a finding consistent with previous studies conducted in LMICs and Bangladesh.18,20,25 The correlation between antenatal care utilization and SBA supervised delivery can be attributed to several factors. Firstly, mothers who attend antenatal care sessions are more likely to receive information about the importance of skilled delivery care and the associated health benefits, thereby increasing their likelihood of seeking such services. 18 Antenatal care provides an opportunity for healthcare professionals to educate mothers on safe delivery practices and encourages them to opt for delivery care by SBA during childbirth. 14 Additionally, mothers who prioritize antenatal care may be more health-conscious and proactive in seeking comprehensive maternal healthcare services, including skilled delivery care. 32 Moreover, mothers accessing antenatal care may also have higher empowerment, which leads them to access such services. 33 This empowerment, coupled with the awareness mothers receive by accessing antenatal healthcare services, leads them to uptake delivery healthcare services aided by SBA.
This study possesses several strengths as well as a few limitations. Firstly, we analyzed most recent nationally representative datasets with a large sample size. The response rate among the selected households and women within these households was notably high, suggesting that unknown factors, such as power dynamics, did not influence the sample we analyzed. Utilizing advanced statistical modeling, we adjusted for a wide range of confounding factors at the individual, household, and community levels. Therefore, the study’s findings are more likely to be generalizable not only to Bangladesh but also to other LMICs. However, it’s crucial to note that the reported association is correlational rather than causal, given the cross-sectional nature of the data analyzed in this study. Additionally, all data were self-reported, and respondents were required to recall information about previous events, introducing the potential for recall bias. Nevertheless, any biases are likely to be random. Moreover, the availability of SBAs in the area and across the country, along with their readiness to provide services within the community, can significantly influence access to SBA services. These factors are, therefore, critical to consider in the model. However, we were unable to include them in the analysis due to the absence of relevant variables in the survey. Despite conducting a thorough search across multiple databases, we could not identify any data that could serve as a suitable background to justify this study. Despite these limitations, the study’s findings, derived from analyzing data extracted from such a large, nationally representative sample of newborns, are anticipated to contribute significantly to the existing knowledge. We recommend exploring this issue further through prospective cohort data for future studies.
Conclusion
We observed that 70% of women in Bangladesh accessed skilled delivery healthcare services aided by SBA, this percentage decreased to 65.3% among women lacking decision-making autonomy regarding the participation in household decision making autonomy. Women who independently or jointly with their husband made all their decisions exhibited a higher likelihood of utilizing SBA services. Additionally, various socio-demographic characteristics of women were found to be associated with the uptake of SBA during childbirth. To enhance women’s empowerment, policies and programs are essential, emphasizing increased education and raising awareness among women regarding the significance of maternal healthcare services. Furthermore, promoting the uptake of antenatal healthcare services is crucial for increasing the utilization of skilled delivery care services. Efforts should be made to document the number of SBAs available in the country, as well as those currently providing delivery healthcare services, given that a significant number of SBAs transition out of their profession. This information would help assess the current status of SBAs in Bangladesh and inform relevant policies and programs.
Supplemental Material
sj-docx-1-his-10.1177_11786329251316674 – Supplemental material for Effects of Women’s Participation in Household Decision Making on Skilled Birth Attendants Supervised Delivery in Bangladesh
Supplemental material, sj-docx-1-his-10.1177_11786329251316674 for Effects of Women’s Participation in Household Decision Making on Skilled Birth Attendants Supervised Delivery in Bangladesh by Md Badsha Alam, Shimlin Jahan Khanam, Md Awal Kabir, Atika Rahman Chowdhury, Tahir Ahmed Hassen, Susmita Das and Md Nuruzzaman Khan in Health Services Insights
Footnotes
Acknowledgements
The authors thank the MEASURE DHS for granting access to the 2017/18 BDHS data. Moreover, we also acknowledge to Department of Population science, Jatiya Kabi Kazi Nazrul Islam University, Bangladesh where the study was undertaken. We also acknowledge to the Maternal and Child Health Division of icddr,b, which acknowledges the support of the Governments of Bangladesh and Canada for providing core/unrestricted support for its operations and research.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Alam MB and Khanam SJ designed the study, performed the data analysis, and wrote the first draft of this manuscript. Chowdhury AR, Kabir MA, Hassen TA, Das S, and Khan MN critically reviewed and edited the previous versions of this manuscript. All authors approved this final version of the manuscript.
Ethical Considerations
This study analyzed secondary data publicly available. Ethical approval for this survey was provided by the Bangladesh Medical research counsel and Demographic and Health Survey Program of the USA. No additional ethical approval is required to conduct this study.
Consent to Participate
Informed written consent was obtained from all participants.
Consent for Publication
Informed written consent was obtained from all participants.
Data Availability
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.