
Abstract
Background:
Maternal and child health improved considerably due to the Sustainable Development Goals of the United Nations. However, the rate of preventable death worldwide remains high. Nevertheless, implementation was insufficient in low- and middle-income countries, including Indonesia. The study aims to assess the relationships between continuum of care (CoC) in maternal, neonatal and child health (MNCH) services and levels of care in Indonesia, examine the distribution of utilisation and investigate the associations between CoC in MNCH.
Design and methods:
Data were derived from the recent 2017 Indonesia Demographic and Health Survey. Fieldwork took place from July 24 to September 30, 2017. The sample included ever-married women aged 15–49 years who had given birth in the last 5 years prior to the survey. The total sample size is 15,288.
Results:
Only 52.6% (n = 8038) continued to receive the three levels of MNCH services. Multivariate analysis revealed that variables, such as socioeconomic status, parity and distance from health facilities were statistically significantly associated with the continuum from antenatal to postnatal care (PNC). The use of each level of MNCH care is correlated with the next level of care. Antenatal care is associated with delivery care which is subsequently associated with postnatal care.
Conclusions:
Identifying populations that contribute significantly to overall health inequalities and a well-established follow-up system from pregnancy to PNC may enhance maternal and child health and equity outcomes.
Introduction
Maternal and child health have considerably improved as a result of the Sustainable Development Goals of the United Nations. However, the rate of preventable deaths around the world remains high. New estimates reveal that approximately 290,000 women died due to complications during pregnancy and childbirth in 2017. 1 Despite progress over the past two decades, an estimated 5.3 million children aged under five died mostly from preventable causes in 2018 alone, 1 with nearly 47% dying within the first 28 days of life or during the neonatal period. 2
The United Nations has called for the end of preventable deaths among mothers and children by 2030. 3 Previous studies reported that implementing all levels of care from the antenatal to postnatal periods can reduce neonatal mortality by 36% ± 67%. 4 Moreover, implementing all levels of care were found to reduce three common causes of neonatal mortality: prematurity related deaths were reduced by 58%, intrapartum related deaths decreased by 79% and infection related deaths decreased by 84%. 5 In addition, all stages of care can reduce approximately 15% combined risk of neonatal, perinatal and maternal mortality. 6 Continuum of care (CoC) is an effective approach for improving maternal and child wellbeing. Nevertheless, its implementation in low and lower–middle-income countries 2 was insufficient. Indonesia is one of such countries, where the lowest level of primary care is community-based, located in villages and provides primary health and preventive services. 7
The study focuses on the time of pregnancy, childbirth and early years of newborn life. The programmes are antenatal care (ANC) during pregnancy, the presence of a skilled birth attendant (SBA) during childbirth and postnatal care (PNC) for mothers and newborns. Therefore, recognising the usage behaviour of vital services in the MNCH care system is important not only for reducing health inequity but also for designing and implementing better strategies to improve the overall public health perspective. As advocated by the WHO, pregnant women should have at least four ANC visits during pregnancy. 8 SBAs (i.e. qualified and experienced practitioners, such as physicians, nurses and midwives) are well armed with the medicines and supplies required for effective prevention, diagnosis and referral in the case of obstetrical emergencies. 9 Women will continue to care for themselves and their newborns after childbirth, as the postpartum period is a critical step in avoiding complications that could lead to maternal or newborn mortality. 10 Many studies explored the various factors influencing the use of individual maternal health services, particularly for ANC, SBA and PNC separately.11–13 Nonetheless, the study is special in nature because it focuses on diverse trends in the utilisation of MNCH services. This study aims to examine the relationships within the ANC, SBA, PNC and the distribution of the utilisation of MNCH services in Indonesia.
Design and methods
Data were derived from the recent Indonesia Demographic and Health Survey (IDHS), a nationally representative, large-scale and repeated cross-sectional survey conducted in 2017. Fieldwork took place from July 24 to September 30, 2017. The IDHS sample design utilises two-stage probability sampling within the selected enumeration areas and households. Information on the selected indicators of maternal and child health was taken from 49,627 ever-married women aged 15–49 years who had given birth in the last 5 years prior to the survey and administered a standard self-reported questionnaire. 14 The resulting sample size was 15,288. The reason for selecting women who gave birth in the last 5 years prior to the survey was to prevent bias in the memory recall of mothers.
The study outcome variables refer to the ANC, SBA and PNC of the MNCH systems. The independent variables are determinants relevant to the individual characteristics of reproductive status, such as age of respondents, age at first birth, level of education, employment status, parity and autonomy in healthcare decision making. Data on family factors were measured through the level of education and employment status of spouses, wealth quintiles and mass media consumption (i.e. frequency of reading newspapers, watching television or listening to the radio). Finally, the community context consists of the form of geographical division of respondents into urban and rural areas and distance from health facilities.
Data were analysed using SPSS version 25. Descriptive statistics in the form of frequencies and percentages were used to report the results of MNCH services at ANC, SBA and PNC. Simple bivariate and multivariate analyses of logistic regression were used to define the relationship between factors at the three levels, odds ratio (OR), adjusted odds ratio (aOR), 95% confidence intervals (95% CI) and p-values with a level of significance at p ≤ 0.05.
Respondents read a written informed consent statement before each interview is conducted. Procedures and survey protocols are reviewed and approved by the Inner City Fund International Inc., Fairfax, VA, USA (ICF) Institutional Review Board (IRB). After authorisation to use the dataset was obtained from the DHS, additional ethical review approval was obtained from the IRB in Indonesia (575/UN2.F10.D11/PPM.00.02/2020), at Universitas Indonesia.
Results
Table 1 provides the descriptive measures of CoC coverage among respondents of reproductive age. ANC4+ coverage, SBA utilisation and PNC coverage are 88.4%, 83.4% and 66.9%, respectively. Despite the high ANC4+ coverage, the number of mothers who had ANC4+ and received assistance from an SBA at delivery dropped to 76%, followed by a dramatic decrease to 52.6% of mothers who received continued care at all three levels (i.e. ANC4+, SBA and PNC). Data indicate that the highest discontinuation rate occurred at the PNC stage.
Measures to describe CoC for MNCH services.

Table 2 indicates that in comparison with <4 ANC visits, 51.9% of mothers aged 25–34 years old, who had their first birth at age 20–29 years (66.5%) or >29 years (6.5%), who achieved secondary (57.4%) or higher education (18.3%), had husbands with secondary (57.9%) or higher (15.7%) education, are employed (54.1%), has an employed husband (99.3%), who experienced less than two pregnancies (67.8%), has autonomy in health decision making (44.2%), were exposed to two (28%) or more (27.7%) mass media platforms, has a high household income (Q3: 19.5%; Q4: 19.2%; Q5: 18.4%), had no issue with distance from health facilities (89.3%) and who lives in urban areas (51.4%) were more likely to have complete four ANC visits during pregnancy. Similar patterns and significance results were also observed in the non-SBA-assisted delivery group and those who did not seek PNC.
Association of three levels of CoC for MNCH with various key determinants.

Table 3 demonstrates that in comparison with the group with discontinued care at postpartum, 52.8% of mothers aged 25–34 years old, had their first birth at age 20–29 years (69.1%), achieved secondary (59%) or higher education (20.7%), had husbands with secondary (59.7%) or higher (17.8%) education, are employed (55.6%), experienced less than two pregnancies (70%), has autonomy in healthcare decision making (45.1%), exposed to two (29.7%) or more (29.6%) mass media platforms, has a high household income (Q3: 21.2%; Q4: 21%; Q5: 20.7%), without issues regarding distance from health facilities (91%) and live in urban areas (54.8%) were more likely to complete PNC.
Association of three levels of CoC with various key determinants.
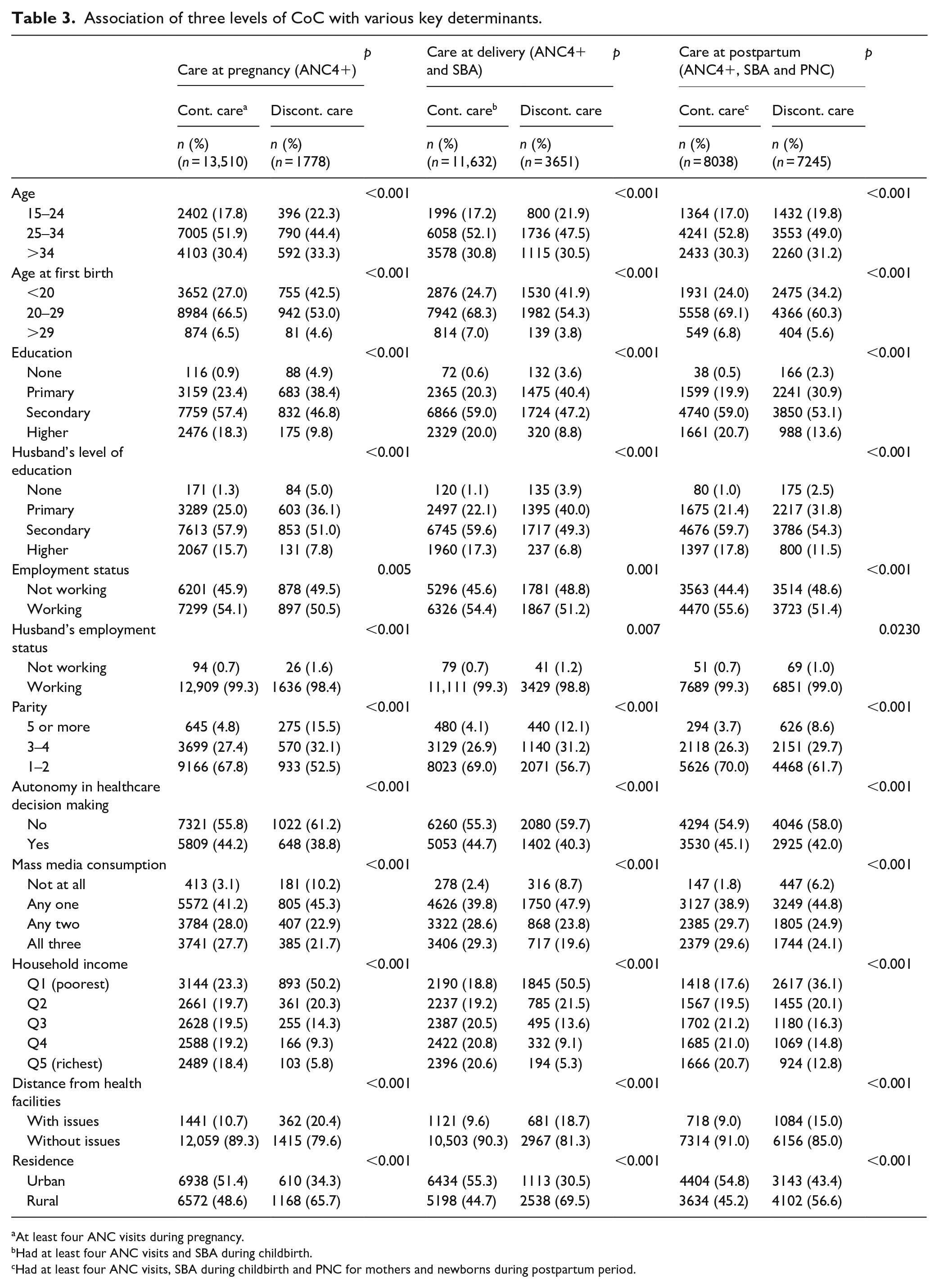
At least four ANC visits during pregnancy.
Had at least four ANC visits and SBA during childbirth.
Had at least four ANC visits, SBA during childbirth and PNC for mothers and newborns during postpartum period.
Table 4 illustrates that mothers aged 25–34 years (AOR 1.12; 95% CI: 1.01–1.24) and over 34 years (AOR 1.28; 95% CI: 1.12–1.45), who first gave birth at 20–29 years old (AOR 1.22; 95% CI: 1.12–1.32), has completed secondary (AOR 2.21; 95% CI: 1.49–3.26) or higher (AOR 2.07; 95% CI: 1.38–3.10) education, are employed (AOR 1.14; 95% CI: 1.07–1.23), experienced 1–2 pregnancies (AOR 2.11; 95% CI: 1.78–2.51) or 3–4 pregnancies (AOR 1.65; 95% CI: 1.4–1.94), has autonomy in decision making (AOR 1.08; 95% CI: 1.01–1.15), exposed to higher mass media consumption (AOR 1.77 95% CI: 1.43–2.21), higher household income (AOR 2.07; 95% CI: 1.81–2.36) and had no issues with distance from health facilities (AOR 1.36; 95% CI: 1.22–1.52) were more likely to complete all stages of continued care.
Logistic regression models of achievement of continued care at pregnancy, continued care at delivery and complete continued care with various determinants.
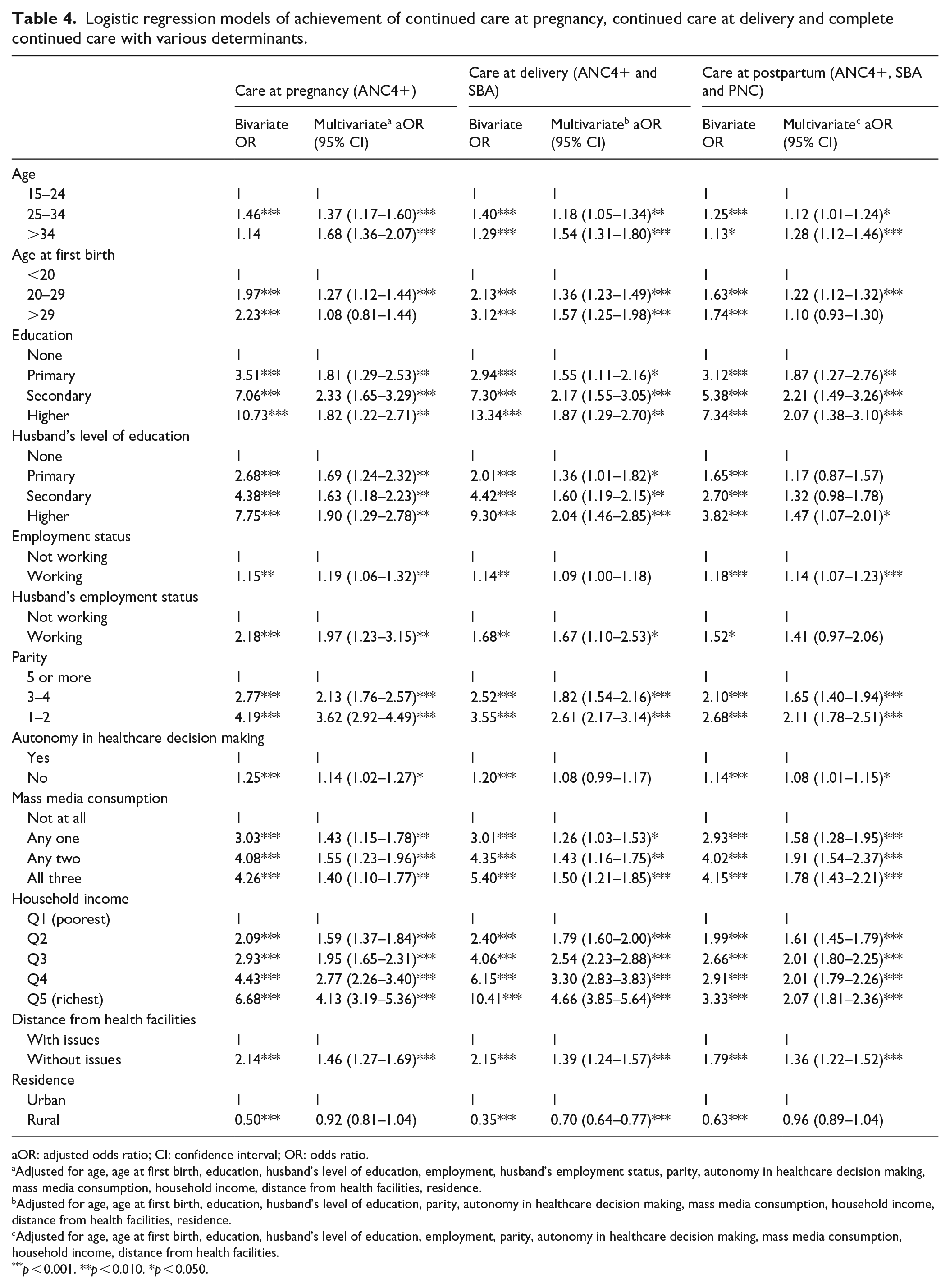
aOR: adjusted odds ratio; CI: confidence interval; OR: odds ratio.
Adjusted for age, age at first birth, education, husband’s level of education, employment, husband’s employment status, parity, autonomy in healthcare decision making, mass media consumption, household income, distance from health facilities, residence.
Adjusted for age, age at first birth, education, husband’s level of education, parity, autonomy in healthcare decision making, mass media consumption, household income, distance from health facilities, residence.
Adjusted for age, age at first birth, education, husband’s level of education, employment, parity, autonomy in healthcare decision making, mass media consumption, household income, distance from health facilities.
p < 0.001. **p < 0.010. *p < 0.050.
Discussion
CoC framework is essentially the most effective strategy for improving maternal and neonatal health, 15 by focusing on time and place (levels of care) that determine the health, MNCH service utilisation and overall healthcare-seeking behaviour by pregnant women. Overall, the CoC is completed along a path from pregnancy to childbirth to postpartum, where each stage contributes to bettering the health of expectant mothers and their babies. The CoC must be improved if maternal and neonatal mortality is to be reduced. Besides, the availability of antenatal care and skilled birth attendants will be improved by reducing inequities. The study demonstrated important findings as the uptake of maternal and newborn health services in Indonesia and highlighted several significant predictors of CoC. All expectant women should receive appropriate and high-quality ANC throughout their pregnancies. Regular ANC visits and its related information assist women prepare for childbirth by letting them to detect and cure illnesses during pregnancy as well as access medical facilities for emergency obstetric care. Prenatal care is thought to be an important predictor of later need for skilled assistance during birth. Women who receive high-quality ANC care are more knowledgeable about pregnancy and more likely to grasp the importance of SBA and PNC.
Our findings regarding maternal age and maternal age at first birth are consistent with the previous study in Asia.16–18 Respondents aged 30–39 years old are twice more likely to continue maternal care compared with those aged <20 years. 19 However, the present study found several results contradicting the current findings. A study in Kenya found that older women (>35 years old) are less likely to receive continued care at pregnancy and delivery, whereas young mothers were compliant towards maternal healthcare guidelines. 20 In addition, mothers in Uganda aged >20 years old are twice more likely to receive continued care at delivery. 21
Maternal education, as a strong predictor of CoC completion, is in line with several studies conducted in other lower–middle-income countries.16,19,22–26 Education is frequently associated with high levels of literacy and better economic opportunities; thus, women with high levels of education tend to gain better access to information and modern cultural perspective that encourages CoC completion. Contrary to our study, several studies indicated that maternal employment was non-significantly associated with any stages of continued care.16,19 However, a study in Ethiopia, showed that maternal employment increased the chances of continued care at pregnancy by 10% but was non-significantly associated with continued care at delivery and PNC. 25 Women earning money through employment can afford health services; thus, they are less likely to entirely depend on spouses for expenses regarding maternal healthcare.
Greater parity poses a barrier towards seeking continued care and CoC completion among mothers.17,22,25,27,28 Multipara mothers tend to be self-confident based on their past childbirth experience, which diminishes the need to check with a healthcare professional.25,27,28 Meanwhile, first-time mothers are typically fearful of pregnancy complications and are thus more dependent on healthcare professionals and their support system on infant care.22,25 High-parity women experience difficulties in accessing MNCH services due to time constraints related to childcare. 27 Other studies conducted in Pakistan and Ethiopia also indicated that autonomy is a factor significantly associated with continued care at pregnancy and CoC completion.16,22,25 Autonomy is associated with education and urban residence, where both factors are likely to increase the chances of utilising maternal health services. 25
Mass media brings positive effects on healthcare-seeking behaviour and it is consistent with those of studies in Nepal, 29 Pakistan, 16 Ethiopia, 25 and Bangladesh. 18 Government, non-government bodies and healthcare practitioners have used mass media to promote maternal and child health-related messages. Women with high household incomes can afford medical expenses as well as other indirect costs associated with neonatal care.16–19,25,28 The Indonesian government has introduced a National Health Insurance programme that aims to cover the entire population and reduce financial barriers in seeking healthcare, which has contributed to increased birth in health facilities. However, other studies argued that indirect financial barriers remain an issue for women from poor households in terms of seeking healthcare facilities. Indirect costs include, but are not limited to, time and travel costs. 30
Short or accessible distances to health facilities are enabling factors for mothers to seek MNCH services, as proposed by previous studies on lower–middle-income countries.22,24,31 A study in Burkina Faso found that every 1-km increase in distance from a health facility decreases the chance of a mother to receive more than four ANC visits by 5% and to deliver at a health facility or be assisted by SBAs by 27%. 31 Indonesia is still facing a poor distribution of skilled healthcare practitioners. In the most remote areas in the country, mothers have to travel extremely long distances with severe geographical and infrastructure challenges to reach a health facility. Public transportation availability and cost of public transportation remain the largest obstacles to reaching health facilities. 30
The current study used a large sample size that is representative of the Indonesian population. Secondary data applied standard procedures and measurement units for the selection of primary sampling units, household strata and respondents, which thus increased the generalisability of the findings. The 2017 IDHS is the most recent data issued, which minimised potential bias associated with time effects. Nevertheless, the study highlights several limitations; thus, the results must be interpreted with caution. Data were derived from a retrospective cross-sectional survey. Hence, the causal relationships between variables could not be established. Data used a self-reported questionnaire are subject to recall bias. For future studies, a prospective study or a randomised controlled trial is needed to evaluate the cause and effect relationships between individual characteristics, family factors, community context and CoC in Indonesia. Additionally, exploring cultural influence and other unidentified barriers to the utilisation of MNCH services for women in disadvantaged groups is important for the planning of intervention.
In conclusion, the study demonstrated the coverage rate of ANC4+ (88.4%), SBA utilisation (83.4%) and PNC (66.9%) in Indonesia and highlighted that the CoC completion rate reached 52.6% among the respondents. The largest gap in discontinued care occurred between delivery and PNC. Other gaps within the MNCH services and healthcare system should be addressed to continually reduce maternal mortality. The quality of ANC should be prioritised because it is related to a mother’s subsequent use of MNCH services. A multisectoral approach (i.e. the synergies of specific interventions in the health sector and sensitive interventions in the non-health sector) and future intervention, such as community mobilisation and empowerment, and health provider capacity building should be highlighted to improve MNCH service availability and accessibility as well as to boost the CoC completion rate for socioeconomically disadvantaged women, especially those who live considerably far from health facilities.
Footnotes
Acknowledgements
The authors would like to acknowledge the Indonesian Demographic and Health Surveys (IDHS) Programme for the access to the data used in this study. This study was supported by the research grant from the Directorate of Research and Community Engagement of Universitas Indonesia. The funders had no role in the design of the study and collection, analysis and interpretation of data and in writing the manuscript.
Author contributions
HA, conceptualisation; SDR and VN, data acquisition and curation; HA and AS, methodology; HA, software; SDR and VN, formal analysis; HA, SDR, VN, AS, interpretation; HA, manuscript drafting; HA, VDR, VN, AS, manuscript review and editing. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Directorate of Research and Community Engagement of Universitas Indonesia, grant number NKB-773/UN2.RST/HKP.05.00/2020. The funders had no role in the design of the study; in the collection, analyses or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Institutional Review Board
The Institutional Review Board (IRB) of the Inner City Fund International Inc., Fairfax, VA, USA reviewed and approved the study procedures and survey protocols. After obtaining authorisation from the IDHS to use the dataset, the IRB of Universitas Indonesia provided further ethical review approval (575/UN2.F10.D11/PPM.00.02/2020).
Informed consent
Informed consent was obtained from all subjects involved in the study.
Significance for public health
Continuum of care (CoC) pertains to the utilisation of all levels of care from the antenatal to postpartum periods to ensure the reduction of neonatal and maternal mortality, as an essential and effective approach for improving and supporting maternal well-being. Our study analysed the diverse trends in maternal, newborn and child health service utilisation. A notable finding is that the most significant gap in discontinued care occurred between delivery and postnatal care. A wide range of representative populations raises the generalisability of results.
Availability of data and materials
Data are available upon request.