
Abstract
Background:
Inappropriate child feeding practices can have significant negative effects on the well-being and survival of children under two years old. This study was aimed at assessing the minimum acceptable diet (MAD) and associated factors among 6 to 23 months age children in Wondo Genet district, Sidama region, Ethiopia.
Methods:
A community-based cross-sectional study was conducted from 1 to 30 July in 2023 among 422 children aged 6 to 23 months. Multi-stage sampling method was applied to select kebeles and study participants. Trained data collectors gathered data using pretested questionnaire. Data was entered into EPI Info 7 and analyzed using IBM SPSS version 26. MAD as a composite indicator was produced based on the proportion of children aged 6 to 23 months who met the minimum meal frequency (MMF) and minimum dietary diversity (MDD) on the previous day. To assess the factors determining adherence to MAD, multi-variable logistic regression analyses were employed. The outputs were presented using an adjusted odds ratio (AOR) with 95% confidence intervals (CI).
Results:
In this study, 419 mothers/caretakers participated with a response rate of 99.3%. The proportion of children who met the MAD were 26.5% (95% CI: 22.29%, 30.71%). Increased odds of meeting MAD were associated with being from food-secured households (AOR = 2.39, 95% CI: 1.48 to 3.86), utilization of growth monitoring services (AOR = 2.05, 95% CI: 1.23 to 3.39), mother attended formal education (AOR = 1.88, 95% CI: 1.15 to 3.08), and being in age range of 12-23 months (AOR = 2.14, 95% CI: 1.26 to 3.63).
Conclusion:
The prevalence of MAD was very low. Factors associated with a MAD included maternal education, child age, growth monitoring service utilization, and food security. To enhance MAD provision, it is crucial to strengthen child feeding practices tailored to the local context.
Introduction
Infant and young child feeding (IYCF) practices directly impact the health, development, and nutritional well-being of children under 2 years old. These practices also play a significant role in child survival. 1 The first two years of a child’s life are of paramount importance, as ensuring optimal nutrition during this period significantly reduces the risk of illness, mortality rates, and the development of chronic diseases. 2 Enhancing IYCF practices among children aged 6 to 23 months is therefore crucial for promoting better nutrition, health, and overall development. 3
From around 6 months of age, infants require more energy and nutrients than what breast milk alone can provide. 4 Therefore, the introduction of complementary foods becomes essential to fulfil their growing needs, playing a vital role in determining the nutritional well-being of children from this age onwards.5,6 The introduction of complementary foods should ensure continued breastfeeding, introduce foods around six months of age, include dairy products, diversify nutrient-rich foods, avoid unhealthy foods and beverages, provide nutrient supplements, and practice responsive feeding.7,8
Dietary diversity, a key component among the main indicators of IYCF practices, assesses the range of foods consumed by children, indicating their access to a variety of food options. 1 The guiding principles for feeding both breastfed and non-breastfed children emphasize that children between the ages of 6 to 23 months should consume a minimum diversified diet comprising at least five out of the eight food groups. 9 As for MMF, the guidelines suggest that breastfed infants and children aged 6 to 8 months should be given complementary foods 2 to 3 times per day, while those aged 9 to 23 months should receive them 3 to 4 times per day. In addition, nutritious snacks should be provided 1 to 2 times per day. For non-breastfed children, the same guidelines recommend 4 to 5 meals per day. 10 The concept of a MAD combines MDD and MMF to form a composite indicator. 9
In low-income countries, several factors such as poverty, limited maternal education, a high burden of disease, and inadequate feeding practices contribute to an elevated risk of poor nutrition among children.11-15 Child feeding practices are influenced by cultural factors, including the choice of low-quality complementary foods, adherence to food taboos, restrictive traditional beliefs, as well as social factors like caregivers’ limited knowledge about nutrition and insufficient awareness of the variety of food options available. 16 These combined factors result in low dietary diversity, infrequent feeding, and inadequate food and energy intake for children. 15
In Ethiopia, limited food variety, inadequate quantities, poor quality, and suboptimal feeding practices 17 increase the risk of micronutrient deficiencies, 1 impacting children’s physical and cognitive development18,6 with long-term consequences. 19 Under-nutrition is a significant challenge, requiring continuous monitoring of child feeding practices. Previous surveys provide limited insights on factors like meal frequency, diet diversity, and adherence,20-22 influenced by media exposure, maternal dietary knowledge, education of mother, income, and family size.18,23-31 To address these gaps, this study aims to assess factors determining adherence to MAD among children aged 6 to 23 months in the Wondo Genet District, Sidama Region, Ethiopia.
Methods and Materials
Study setting, study design, and study period
A community-based cross-sectional study was conducted in Wondo Genet district, Sidama region, Ethiopia, between July 1 to 30, 2023. Wondo Genet is one of the 30 rural districts within the region. It is positioned 24 kilometers to the east of Hawassa City and 270 kilometers south of Addis Ababa, the capital of the country. Administratively, the district is divided into 13 rural kebeles. In terms of agro-ecological zones, Wondo Genet has two: woina-dega and dega. Farming is the primary livelihood for over 85% of the population. The major crops cultivated in the area include enset (kocho), maize, barley, cabbage, tomatoes, and potatoes. The total population of the district is approximately 160,536, comprising 32,762 households and 5,733 children aged 6 to 23 months. With a population density of 768 people per square kilometer, the district has three health centers and 13 operational health posts to cater to the healthcare needs of its residents. 32
Study population and their eligibility criteria
The study included all children aged 6 to 23 months and their mothers/caregivers from the Wondo Genet district as the source population. The study population consisted of selected children and their mothers/caregivers who lived in the district during the study period. Mothers or caretakers who had lived in the selected kebeles for the past 6 months were included in the study. Those mothers or caregivers unable to participate due to illness, and children who were ill the day before or in recovery, were not included in the study.
Sample size calculation
To assess the adequacy of the sample size for estimating the magnitude of MAD, a single population proportion formula was employed. The assumptions considered were a 5% margin of error and a 95% confidence level. Based on a previous study that reported a proportion of 13.8% of children aged 6 to 23 months meeting the MAD, 33 the sample size calculation incorporated a design effect of 1.5 and accounted for a 10% nonresponse rate. Consequently, a sample size of 301 was determined.
The sample size for the associated factors of meeting the MAD was calculated using the double population proportion formula in the Epi InfoTM 7 statistical package. In a previous study, the provision of food preparation training to mothers/caregivers of children aged 6 to 23 months was identified as an associated factor of meeting the MAD. 33 The inputs for this calculation included a 95% confidence level, 80% power, a 1:1 ratio between subjects who met and did not meet the MAD, an outcome of 45.3% in the unexposed group, an odds ratio (OR) of 2.1, and a design effect of 1.5. Taking all these factors into account, a sample size of 422 was calculated. Consequently, the final sample size for the study was determined to be 422.
Sampling procedure
This study followed a multi-stage sampling method. The selection of kebeles (the smallest administrative unit in Ethiopia) and study participants was carried out using the simple random sampling method. Out of the thirteen kebeles in the district, six kebeles (Yuwo, Aruma, Baja Fabrica, Abbaye, Wosha Soyama, and Wotera Gando) were randomly chosen. Lists of children 6 to 23 months of age, along with their mothers or caregivers were obtained for each kebele, and study participants were selected through simple random sampling. For households with multiple children aged between 6 and 23 months, such as twins, the lottery technique was applied to randomly select one child for inclusion in the study. To ensure representation, the sample size was proportionally allocated to the selected kebeles based on the number of mothers/caregivers with children aged 6 to 23 months in each kebele.
Data collection tool preparation
A well-structured, pretested and interviewer-administered questionnaire was used to collect data. The questionnaire was developed based on the objectives of the study after thoroughly reviewing different literature.29,34-37 The tools for assessing dietary diversity and meal frequency were adapted from the World Health Organization (WHO) standardized questionnaire for Infant and Young Child Complementary Feeding practices, with necessary adjustments made to suit the local context. 1 The tool was initially developed in English and translated into Sidamu Afoo by a proficient bilingual professional. It was subsequently back-translated into English by another language expert.
Recruitment of data collectors and supervisors
Data collectors and supervisors were selected through a public announcement inviting applications that met specific criteria, including academic qualifications, prior experience in data collection, and familiarity with the language, culture, and customs of the community. Four nutritionists with a bachelor’s degree in sciences were enlisted to collect quantitative data using structured questionnaires through individual interviews conducted at the participants’ home. Two supervisors with a Master’s degree in Science in Applied Human Nutrition were responsible for overseeing the entire data collection process.
Data collection
The study utilized a WHO standardized questionnaire to evaluate dietary diversity and meal frequency. 1 The socio-demographic and economic aspects of the respondents were also examined. This included gathering information on the age and gender of the child, the age of the mother or caretaker, the educational status and employment status of the mothers, the number of under-five age children, the size of the family, monthly income, place of residence, maternal involvement in household decision making, and home gardening. 37
Another important aspect of the assessment was the obstetric and health service utilization of the mothers or caretakers. This involved collecting data on antenatal care visits, place of delivery, and growth monitoring. Furthermore, the study considered the mothers’ or caretakers’ exposure to various media outlets such as radio, television, and newspapers and training on food preparation. Additionally, information on any illnesses the child had experienced in the week leading up to the data collection period was also obtained. 37
The Household Food Insecurity Access Scale (HFIAS) was used to assess household food insecurity status by examining nine related events over the past 30 days. The questions covered three domains: food access anxiety (1 question), insufficient food quality (3 questions), and insufficient food intake (5 questions). Responses determined a binary outcome of food security or insecurity, with households classified as mildly, moderately, or severely food insecure grouped as food insecure. 38
Data quality assurance
To ensure the data quality, several steps were taken. The data collection tool was designed in a clear and easily comprehensible manner. The data collection tool was pre-tested on 5% (21 respondents) of the sample in the unselected kebele, and based on feedback, necessary modifications were made. Data collectors and supervisors received 3 days of training to enhance their skills. Strict supervision was maintained throughout the data collection process. In the evening meeting sessions, each completed questionnaire was carefully reviewed on a daily basis, and valuable feedback was provided to the collectors and supervisors.
Study variables
The outcome variable of interest was MAD. On other hand eleven independent variables were considered for the study. These were: (1) child’s sex, (2) child’s age, (3) mother/caretaker education level, (4) mother/care taker involvement in decision making, (5) ANC visit, (6) utilization of GMP service, (7) household food security, (8) monthly income, (9) family size, (10) mother/caretaker age, and (11) recent illness history.
Operational definition
Minimum dietary diversity
The proportion of children between the ages of 6 and 23 months who consumed foods from five or more out of the eight (1. breast milk; 2. grains, roots, tubers and plantains; 3. pulses (beans, peas, lentils), nuts and seeds; 4. dairy products (milk, infant formula, yogurt, cheese); 5. flesh foods (meat, fish, poultry, organ meats); 6. eggs; 7. vitamin-A rich fruits and vegetables; and 8. other fruits and vegetables) recommended food groups. 1
Minimum meal frequency
The proportion of children aged 6 to 23 months, both breastfed and non-breastfed, who consumed solid, semisolid, or soft foods (including milk feeds for non-breastfed children) at least 2 to 4 times for breastfed infants and children, and 4 to 5 times for non-breastfed infants and children within the same age range. 1
Data management and analysis
The collected data underwent thorough checks for completeness and consistency before being processed. It was then cleaned, coded, and entered into Epi Info 7. The data was subsequently exported to SPSS Version 26.0 for analysis. Descriptive statistics, such as mean, standard deviation, frequency, percentage, and graphs, were employed to describe socio-demographic/economic factors and other related variables.
Bi-variable logistic regression analyses were conducted to determine the association between independent variables and the outcome variable. To account for confounding variables, the multivariable model included variables from the bivariable model with a p-value of less than .25. The model’s fitness was assessed using the Hosmer and Lemeshow tests, and the presence of multicollinearity was examined using the variance inflation factor (VIF). In the multivariable analysis, a p-value of less than .05 was considered statistically significant. The findings were presented using adjusted odds ratios (AOR) along with 95% confidence intervals (CI).
Ethical clearance
Ethical clearance was obtained from the Institutional Review Board of Yirgalem Hospital Medical College (IRB Protocol Number-YHMC/IRB/067). Written informed consent was obtained from each respondent (mothers or caretakers of children aged 6 to 23 months) after explaining the study objectives.
Results
Socio-demographic characteristics of the respondents
In this study, 419 mothers/caretakers participated with a response rate of 99.3%. The mean (±standard deviation) age of the mothers/caretakers was 26.1 ± 5.1 years, and for the children, it was 13.7 ± 5 months. Over half of the children (54.9%), were aged 12 to 23 months. More than half of the children (52.3%) were females. Nearly half of the mothers or caretakers (51.1%) had not attended formal education, while 59.9% were housewives. The vast majority (98.3%) of the children's mothers or caregivers were married or in a union. The mean (±standard deviation) monthly income of the respondents was 3,440 ± 1409 Ethiopian Birr. Three hundred seventy-five (89.5%) of the children’s families were protestant religion followers. More than half of mothers/caretakers (59.4%) reported having one child under the age of five years in their family, while about two-thirds of the children’s families (67.3%) had less than five members. Less than half (47.5%) of children’s families were food secured (Table 1).
Socio-demographic/economic characteristics of mothers/caretaker’s infant and young children aged 6 to 23 months, Wondo Genet District, July 2023.

Maternal health service utilization
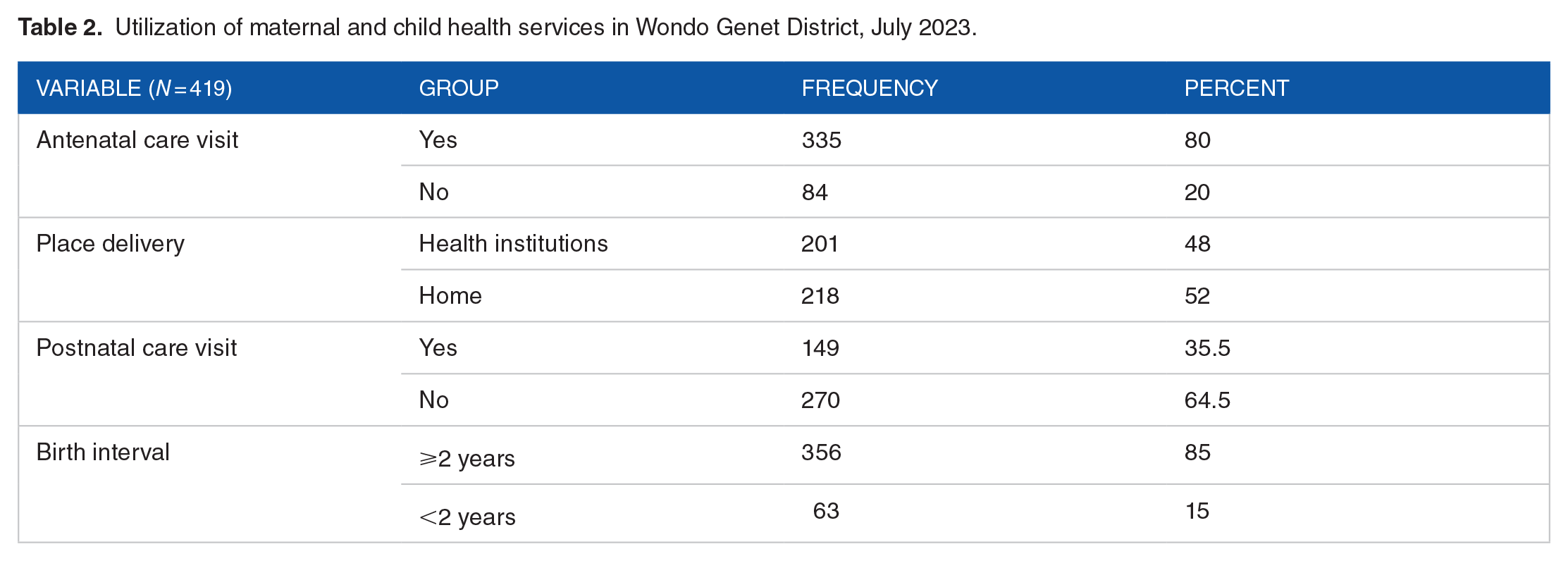
Four-fourths (80%) of mother/caretaker had attended antenatal care visits before their most recent birth, while near to half (48%), gave birth at a healthcare facility. Nearly one-third of women (35.5%), visited a healthcare institution within a month after giving birth for postnatal care. Regarding birth interval, majority of the respondents (85%) reported that they had a birth interval of greater than or equal 2 years as shown on Table 2.
Utilization of maternal and child health services in Wondo Genet District, July 2023.
Infant and young child feeding practices
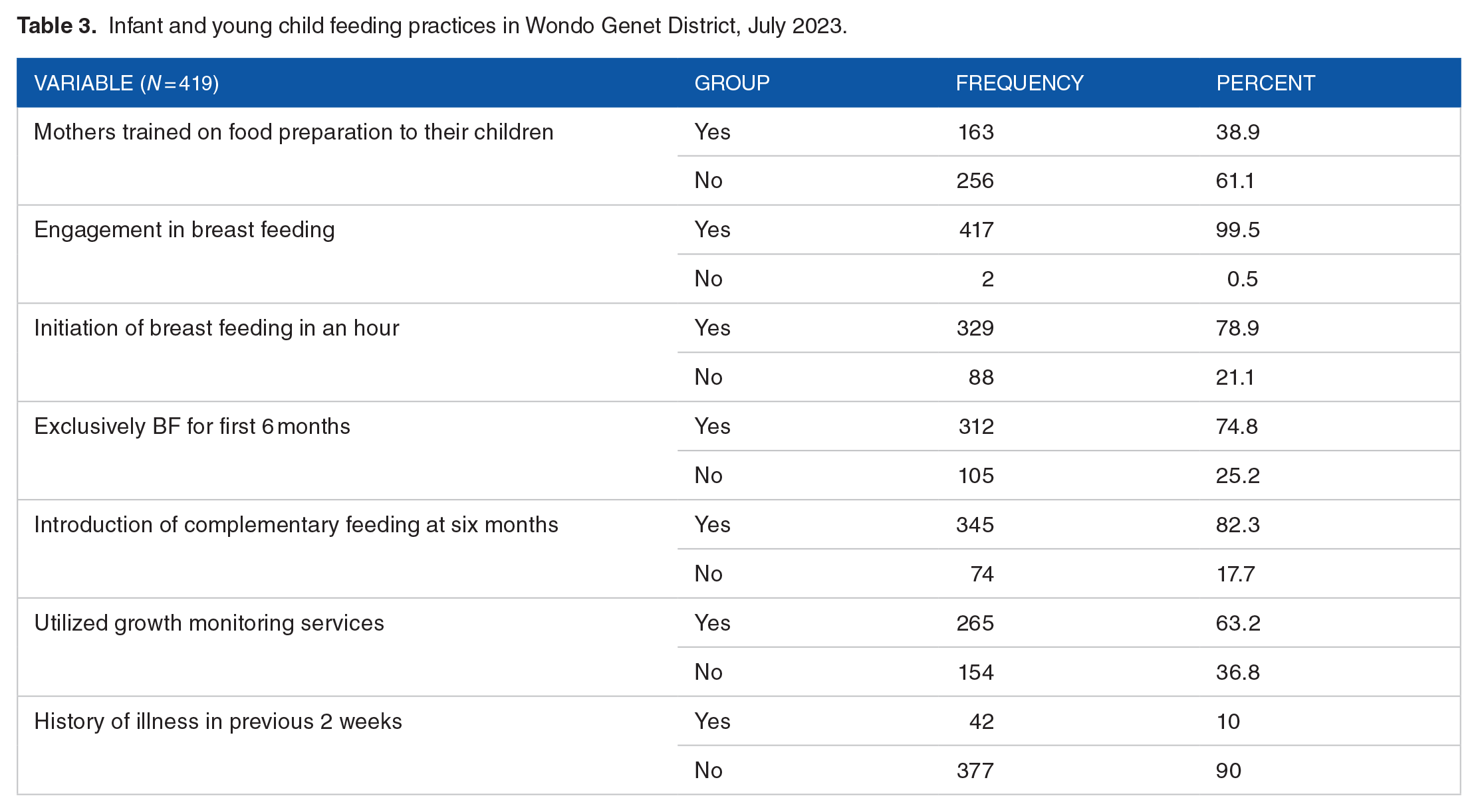
Three in five mothers/caretakers (61.1%) did not receive food preparation training from health extension workers. Nearly all (99.5%) of mothers/caretakers reported engaging in breastfeeding, with 329(78.9%) initiating breastfeeding within an hour after birth. About three-fourth (74.8%) of mothers reported exclusively breastfeeding their infants for up to 6 months, while around 82.3% of mothers initiated complementary foods at the six-month mark. Slightly greater than one third (36.8%) of the infants and young children did not utilize growth monitoring services. Out of every ten infants and children aged 6 to 23 months, one (10%) had a reported history of illness in the two weeks prior to the survey as shown on Table 3.
Infant and young child feeding practices in Wondo Genet District, July 2023.
Minimum dietary diversity, minimum meal frequency and minimum acceptable diet practices
The percentages of children meeting the MDD, MMF, and MAD criteria were 38.2% (95% CI: 33.58%, 42.81%), 70.4% (95% CL: 66.1%, 74.7%), and 26.5% (95% CI: 22.29%, 30.71%) respectively as shown on Figure 1.

Minimum dietary diversity, minimum meal frequency and minimum acceptable diet practices among 6 to 23 months Children in Wondo Genet district, July 2023.
Associated factors of minimum acceptable diet
To determine factors associated with a MAD, bivariable, and multivariable logistic regression were done. A total of eleven independent variables that showed a p-value less than .25 in bivariable analyses were considered as candidate variables for the multivariable model. In the multivariable logistic regression analysis, maternal/caretaker education level, age of the children, utilization of growth monitoring services, and household food security were significantly associated (p < .05) with MAD.
Infants and young children whose mothers attained primary education and above had 1.88 times higher odds (AOR = 1.88, 95% CI: 1.15 to 3.08) of meeting MAD. Similarly, being in age range of 12 to 23 months was twice as likely (AOR = 2.14, 95% CI: 1.26 to 3.63) to meet MAD compared to those infants who were in age range between 6 to 11 months. Likewise, mothers who participated in growth monitoring programs were about twice as likely (AOR = 2.05, 95% CI: 1.23 to 3.39) to satisfy MAD to their infant and young children compared to those who did not participate. Furthermore, mothers/caretakers from food-secured households had 2.39 times higher odds (AOR = 2.39, 95% CI: 1.48 to 3.86) of providing MAD to their infants and young children compared to mothers/caretakers from food-insecure households (Table 4).
Multivariable analysis of associated factors of MAD in Wondo Genet District, July 2023.

NB: 1$USD =55.45 Ethiopian Birr; * = Significantly associated variable.
Discussion
A community-based approach was utilized to assess the associated factors of the MAD among infants and young children aged 6 to 23 months in the Wondo Genet district. Out of the children surveyed, 38.2% attained the recommended minimum dietary diversity, 70.4% met the recommended meal frequency, and 26.5% adhered to the MAD. Factors determined adherence to the MAD in this age group included maternal education, age of the children, utilization of growth monitoring services, and households’ food security level within the Wondo Genet district.
This study found a prevalence rate of 26.5% for children meeting the MAD. Other study conducted in selected urban slums in the Oromia region of Ethiopia also reported comparable result (23.2%). 36 However, studies conducted in the Aleta Wondo district of Sidama region (13.8%), 33 North Shoa of Oromia region (13.3%), 40 and a multilevel analysis of Ethiopian Mini-Demographic and Health Survey of 2019 (11.3%) 36 reported poorer MAD practice. In contrast, studies conducted in Mareka district of southern Ethiopia (35.5%) 34 and Amhara region (31.6%) 14 reported relatively improved MAD practice. These variations could be attributed to differences in factors such as seasonal variation, study time, sample sizes, study settings, study designs, and cultural influences.
According to the study, food secured households were found to have a higher likelihood of meeting the MAD for their children compared to food insecured households. This finding aligns with studies conducted in Zambia, 42 Bangladesh, 43 East Africa countries. 44 The reason behind this association is likely the fact that food-secure households have easier access to an adequate food supply for their children, enabling them to meet the requirements of a MAD. By having reliable and consistent access to food, these households can ensure that their children receive the necessary nutrients and meet the recommended MAD.
The utilization of GMP services was also showed significant association with meeting recommended MAD. Children who received GMP services were more likely to meet the MAD compared to children who did not access these services. This finding is consistent with studies conducted in the Mareka district, southern Ethiopia, 41 north Shewa, Oromia region 40 and Amhara region. 14 This association may be attributed to the fact that healthcare institutions implement the WHO GMP chart as per the standard guidelines, allowing healthcare professionals to monitor children’s growth and development using standardized GMP charts and provide nutrition counseling to mothers or caregivers.
Similarly, the current study assessed the educational background of mothers and found a significant association with meeting the recommended MAD. Compared to mothers/caretakers without formal education, those with a formal education had a higher likelihood of their children receiving the recommended MAD. This finding aligns with previous studies,31,44-47 indicating that educated mothers are better able to comprehend the educational messages conveyed by healthcare professionals during antenatal and postnatal care, as well as through various mass media channels such as radio or newspapers. The increase in understanding and engagement empowers educated mothers to successfully ensure their children’s adherence to the recommended MAD.
The current study has also identified children’s age as one of the associated factors. It was observed that children in the 12 to 23-month age group were more likely to meet MAD compared to those aged between 6 and 11 months. This finding is consistent with previous studies conducted in Ethiopia14,21,28, Kenya, 48 East Africa Countries Demographic Health Survey Analysis 44 and Nepal. 13 . The possible explanation for this could be mothers might perceive that the intestines of young children are not yet capable of digesting solid or semi-solid foods. They may also be concerned that introducing bulky foods could increase the risk of infections in their children.
Limitation of the study
The following limitations need to be considered while interpreting the findings of the study. Recall and social desirability biases may have influenced the findings due to the use of 24-hour dietary recall data for assessing dietary diversity and meal frequency. The quantitative nature of the study hindered in-depth exploration of mothers/caregivers’ perceptions and barriers. We did not investigate the association between MAD and child nutritional status. In addition, inclusion of in-depth interviews or focus groups would enhance understanding of women’s perceptions and barriers for meeting MAD.
Conclusion and Recommendation
The proportion of 6 to 23 months age children that met MAD was very low. Household food security, utilization of GMP services, maternal education, and children’s age determined adherence to MAD. These results highlight the need for policymakers to prioritize enhancing complementary feeding practices for children, addressing issues related to food security, maternal and child health services utilization, and improving the socioeconomic status of households.
Footnotes
Acknowledgements
We express our gratitude to Yirgalem Hospital Medical College for generously funding this study. Additionally, we would like to extend our sincere appreciation to the health extension workers of each selected kebele, the study participants, and the dedicated data collectors and supervisors who made this research possible.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study received financial support from Yirgalem Hospital Medical College.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Abbreviations
ANC: Antenatal Care; AOR: Adjusted Odds Ratio; CI: Confidence Intervals; COR: Crude Odds Ratio; GMP: Growth Monitoring and Promotion; IYCF: Infant and young child feeding; MAD: Minimum Acceptable Diet; MDD: Minimum Dietary Diversity; MMF: Minimum Meal Frequency SD: Standard Deviation; WHO: World Health Organization.
Author contributions
Both of the authors equally participated in study conceptualization, formal analysis, writing original draft and review and editing.
Data availability
The data collection tool used in this study is available in the supplementary material of this article.