
Abstract
In Ethiopia, Social Health Insurance (SHI) implementation was delayed repeatedly due to employees’ unwillingness to pay 3% of their monthly salary and fear related to the scheme’s healthcare coverage. However, provisions of comprehensive training for health workers on health insurance and inclusion of healthcare financing methods in health practitioner education curriculum make their level of willingness to pay for SHI schemes uncertain. Thus, this study aimed to assess willingness to pay for the SHI scheme and its determinant factors among Healthcare providers in the Gedeo zone. From July 1 to 15, 2022, we carried out an institution-based cross-sectional study among 430 healthcare providers recruited using a multistage sampling technique. A multivariable logistic regression model was used to determine the factors associated with willingness to pay for Social Health insurance. Adjusted odds ratio (AOR) and P values of <.05 with 95% confidence intervals (CIs) were used to declare statistical significance. Out of 73.4% (95% CI: 68.8%, 77.6%) healthcare providers willing to join the SHI program, only 47.3% (95% CI: 41.5%, 53.2%) were willing to pay for the proposed 3% premium of their monthly salary. Healthcare providers who had >10, 000 Birr monthly salary (AOR = 2.45, 95% CI: 1.14, 5.26), difficulty in paying for healthcare (AOR = 3.55, 95% CI: 1.22, 10.29), history of chronic conditions (AOR = 4.61, 95% CI: 2.41, 8.82), positive attitude (AOR = 3.16, 95% CI: 1.62, 6.18), and good knowledge of the social health insurance scheme (AOR = 2.35, 95% CI: 1.17, 4.72) were more likely to pay for the social health insurance. More than half of the healthcare providers expressed a lack of willingness to pay for the social health insurance scheme. So, the government should provide an awareness creation program on the concepts and principles of the SHI scheme to improve the willingness to pay for the scheme.
Introduction
Modern healthcare services have not been widely used in Low and middle-income (LMIC) countries due to financial barriers at the time of service delivery.1,2 Thus, the World Health Organization (WHO) demanded universal health coverage (UHC) which it defined as “access to adequate health care for all at an affordable price” to be implemented in all health systems.3,4 Despite the WHO plan to make significant progress towards UHC by 2030 to improve health services coverage, the proportion of people who face catastrophic levels of out-of-pocket (OOP) health expenditure has increased. 5 Globally, depending on the poverty line used to evaluate impoverishing health spending, the number of people suffering from financial hardship ranges from 1.4 to 1.9 billion, with approximately a half billion people living in extreme poverty.5,6 Since 2000, Low and middle-income countries (LMICs) including sub-Saharan African countries have significantly improved their UHC service coverage index relative to developed nations, and they have also seen huge rises in catastrophic OOP health spending.5,7 As pre-payment mechanisms are a more efficient and equitable method of financing healthcare, it is advisable to minimize OOP spending in favor of them.6,8 Thus, LMICs have implemented community-based health insurance (CBHI) schemes to mobile resources from households to improve service utilization.9,10 However, the majority of these countries still lack SHI schemes for their workers and use OOP expenses to pay for health care. 11
In Ethiopia, the healthcare system has been characterized by a lack of adequate healthcare financing and personnel resources, as well as a shoddy infrastructure for decades.12,13 In addition, most healthcare expenditures in the country are borne through OOP spending payable by healthcare seekers, accounting for 33.1% of total healthcare expenditure. 14 However, the government has made significant progress recently to make healthcare more efficient and accessible for everybody.13,15 A healthcare financing reform was implemented, resulting in substantial modifications to the financial framework of healthcare facilities and a notable rise in public health spending.16,17 Health insurance (ie, CBHI and SHI) was initiated as components of the healthcare financing reform to increase healthcare utilization, access to medicines, and quality of services in Ethiopia. 15 In 2011, the CBHI program was implemented in Ethiopia as a prepayment method to reduce household dependency on OOP medical expenses and expanded following a successful 3 year pilot program.18,19 On the other hand, SHI was designed by the federal government over 10 years ago, with a plan to cover civil servants, non-governmental organizations, pensioners, and private sector companies workers in the program. 20 However, its implementation was delayed repeatedly due to civil servants’ unwillingness to pay 3% of their monthly salary and fear related to the scheme’s healthcare coverage.16,20,21 Few studies conducted in Ethiopia indicated varying level of willingness to pay(WTP), which was 74.9% in North Ethiopia, 22 62% in Gondar Town, 23 and 32% in Northwest Ethiopia. 24 In addition, studies performed in Mekelle, 25 Addis Ababa City, 26 and Wolaita Sodo town 27 revealed that WTP for the SHI scheme was 85.3%, 28.7%, and 74.4% respectively. From previous studies, factors considered as determinants for WTP for the SHI scheme include sociodemographic and economic factors, health and health-related factors, knowledge, and attitude towards the SHI scheme.22-24,28 Currently, ensuring financial risk protection for the front-line healthcare providers by availing health insurance is among the federal Ministry of Health’s priorities. Thus, provision of comprehensive training on health insurance and inclusion of healthcare financing in the health practitioner educational curriculum was performed, which might have a direct or indirect impact on their WTP for the SHI scheme. As a result, despite the fact that few studies were conducted to evaluate WTP for the SHI scheme in Ethiopia, there is a lack of information on the magnitude of WTP for the SHI scheme among Healthcare providers. Thus, this study aimed to determine the magnitude of WTP for the SHI scheme and its determinants among healthcare workers in the Gedeo Zone of Southern Ethiopia.
Methods and Materials
Study setting, design, and period
From July 1 to 15, 2022, an institution-based cross-sectional design study was carried out. The study was carried out among healthcare providers in the Gedeo zone, which is located 365 kilometers away from Ethiopia’s capital, Addis Ababa. The zone has a population of about 1 694 868 and is divided into 6 districts and 2 town administrations. There are 146 Health posts, 38 Health centers, 3 primary hospitals, and 1 referral hospital, serving population from 22 urban and 133 rural kebeles (the smallest administrative unit) in this zone. A report from the zonal health office revealed that approximately 2301 healthcare workers are employed in the zone at different levels of the healthcare system.
Study population and eligibility criteria
All healthcare providers working in public health institutions in the Gedeo zone were considered as the source population. The study population consists of all healthcare providers in randomly selected public health institutions in the Gedeo zone. Healthcare providers who were permanently employed and presented during the study period were included in the study. Healthcare professionals who were severely ill, working for an apprenticeship, on sick leave, giving birth, or absent from work during data collection were excluded.
Sample size determination and sampling procedure
Using the single population proportion formula, we calculated a sample size of 472, taking the proportion of WTP for the SHI program (P = 28.7%), 26 confidence level of 95%, margin of error of 5%, design effect of 1.5, and an expected non-response rate of 10%. Since the number of health workers in the Gedeo zone is less than 10 000, the final sample of 430 is determined using a correction formula. A multi-stage sampling method was used to select the study participants. In the first stage, 3 districts and 1 town administration were selected randomly from 2 town administrations and 6 districts in the zone. In the second stage, 8 health facilities were randomly selected and the sample was proportionally distributed among selected health facilities in the selected districts or town administration. Finally, using the sampling frame prepared for this study from each facility, systematic random sampling was used to interview the respondents.
Study variables
Dependent variable
Willingness to pay for Social Health Insurance.
Independent variables
Socioeconomic factors
Age, gender, family size, marital status, monthly income, occupation, and education.
Health and health related factors
Getting diseases in the last 6 months, presence of chronic conditions, difficulty paying medical costs, perceived quality of healthcare, and health status.
Social health insurance variables
Attitude and knowledge about the SHI program.
Operational definition
Willingness to join
This is described as the willingness of healthcare providers to enroll in social health insurance to receive benefits from the scheme, regardless of the payment amount. It is measured using closed questions after explaining how the system works. 29
Willingness to pay
It is described as the health care provider’s willingness to pay 3% of the gross monthly salary that has been set by the government for the proposed SHI system in Ethiopia.29-31
Knowledge of the SHI scheme
Knowledge of the SHI scheme was determined by 13 yes/no questions about the principles of SHI and the benefits to insureds under the scheme. Respondents who scored 60% or more on the overall knowledge score were considered to have a good understanding. 32
Attitude toward the SHI scheme
A 6-item question having a 5-point Likert scale ranging from strongly disagree to strongly agree was used to determine participants’ attitudes toward the SHI program. A “positive attitude” towards the SHI scheme was indicated by respondents with a score of 60% or more on the total attitude measurement scale, while a “negative attitude” was indicated by respondents with a score of less than 60%.22,23
Data collection procedures and quality management
A structured interviewer-administered questionnaire was developed to collect data from the participants based on a review of relevant studies.22-24 The tools consist of demographic and socioeconomic factors, health and health-related factors, and social health insurance-related factors (ie, level of WTP for SHI scheme, knowledge and attitude towards SHI scheme). The questionnaire was prepared in English, translated into the local language (Gedeu’ffa) to ensure consistency, and finally returned to English. Three graduate health workers and 1 senior health worker collected the data after 2 days of training. A pre-test was conducted on 5% of the sample at Chuko Health Center and necessary adjustments were made based on the results of the pre-test before actual data collection began using the data collection tool. Supervisors visited the data collection process daily, and the principal investigator checked daily for data consistency and completeness.
Data analysis
Data were coded, entered, and analyzed using Statistical Package for Social Sciences (SPSS) version 25. Descriptive statistics such as mean, standard deviation, frequency, and percentage were used to present the results. Associations between independent variables and willingness to pay for the SHI scheme were assessed using multivariate logistic regression analyses. Independent variables with P values <.25 in bivariable logistic regression were entered into multivariable logistic regression for analysis. Adjusted odds ratios (AORs) and 95% confidence intervals were computed, and a P-value <.05 was considered statistically significant. Meanwhile, the Hosmer-Lemeshow goodness of fit test was used to evaluate the model fitness.
Results
Socio-demographic characteristics of the respondents
Of the 406 study participants, 256 (63.1%) were male and 268 (66.0%) were in the 20 to 29 age group with a mean (SD) age of 32 (+3.60) years. Only 174 (42.9%) of the study participants had a BSC degree, 154 (37.9%) were nursing professionals, and 197 (48.5%) were Orthodox Christians. In addition, 289 (71.2%) of the respondents had a family size of <5 (Table 1).
Sociodemographic characteristics of respondents in Gedeo zone, Southern, Ethiopia, 2022.
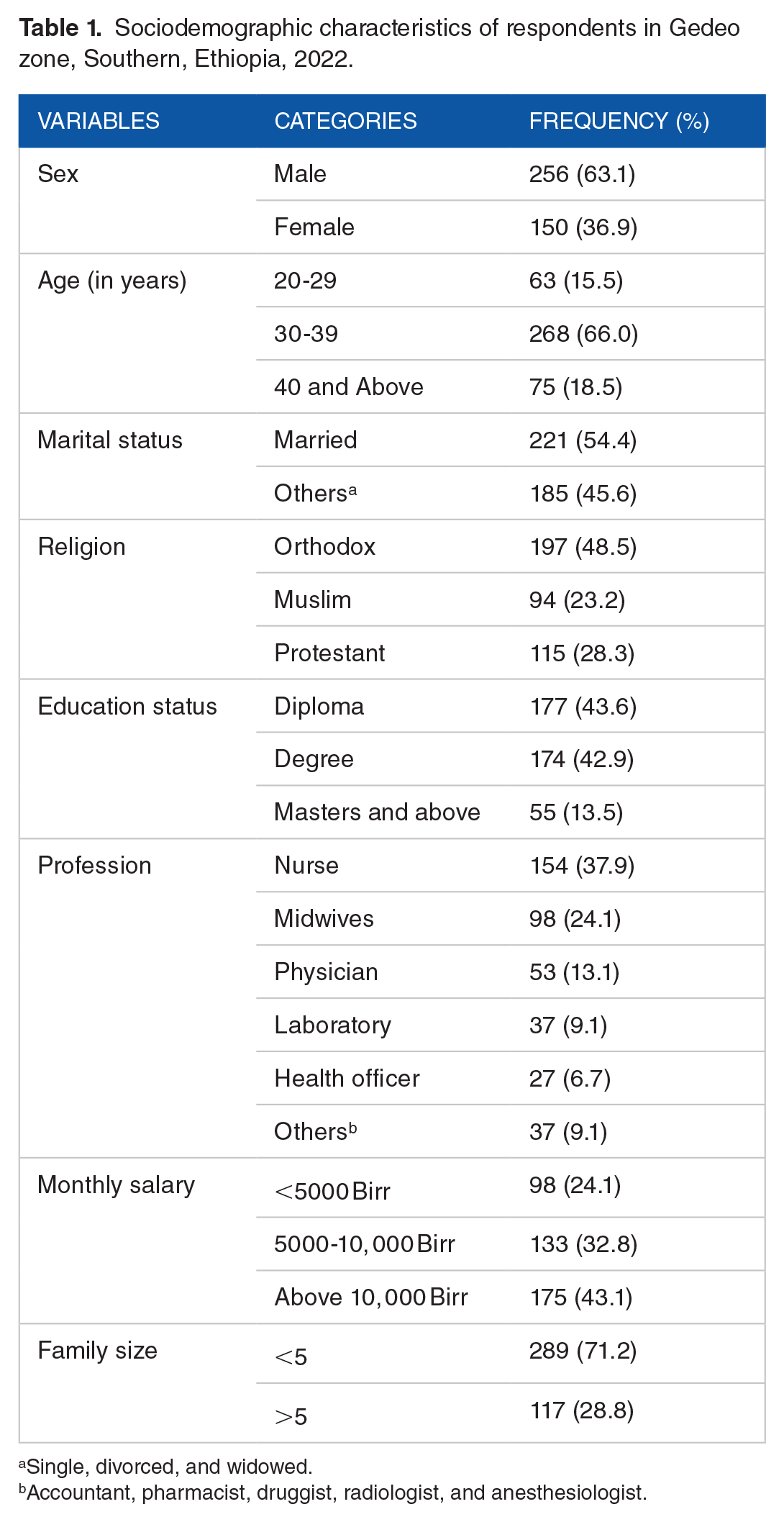
Single, divorced, and widowed.
Accountant, pharmacist, druggist, radiologist, and anesthesiologist.
Health and healthcare-related characteristics of participants
Of the 406 participants interviewed, 104 (25.6%) had a chronic illness, and 96 (23.6%) of them experienced an illness within 6 months. Among those who had experienced an illness in the past 6 months, 56 (62.2%) and 39 (43.3%) of them reported having difficulty managing their illness and satisfaction with the cost of treatment (Table 2).
Health and healthcare characteristics of respondents in Gedeo zone, Southern Ethiopia, 2022.

Multiple response is possible.
Respondent’s awareness and attitude towards Social Health Insurance scheme
Of the 406 study participants, 315 (77.6%) had heard of the SHI program. The main sources of information about the SHI program were health workers in health facilities, 184 (58.4%), and friends 54 (17.1%). Regarding the overall knowledge of the SHI program, 283 (69.7%) respondents had sufficient information about the structure of the SHI program, its benefits, and the basic principles of the program (Table 3).
Respondents’ attitude and knowledge of a social health insurance scheme in Gedeo Zone, Southern Ethiopia, 2022.

Multiple responses are possible.
Willingness to pay for the Social Health Insurance scheme
Two hundred ninety-eight (73.4%) healthcare providers were willing to participate in the proposed SHI scheme. Of participants willing to participate in the SHI program, 47.3% (95% CI: 41.7%, 53.0%) were willing to pay for the program. Of the respondents who were willing to pay the first offer, 33 (23.4%) were also willing to pay the next highest offer. Also, among participants who were unwilling to pay the first offer, 113 (72%) of them were willing to pay the next lowest offer. The overall mean amount of premium the healthcare providers were willing to pay was 2.47% (95% CI: 2.30, 2.64) of their gross monthly wages (Table 4). Of the 108 respondents who were unwilling to join the SHI scheme; 33 (30.6%), and 28 (25.9%) were not willing to participate due to the unaffordability of 3% premium and poorly service quality of health care in public health facilities respectively (Figure 1).
Willingness to pay for social health insurance among health workers in Gedeo zone, Southern Ethiopia, 2022.


Reasons for not willing to join the Social Health insurance scheme.
Factors associated with willingness to pay for SHI scheme
Factors such as age, sex, education, family size, monthly income, presence of chronic disease, history of disease in the last 6 months, difficulty in covering medical costs, knowledge, and attitude towards the SHI program were moved to multivariate logistic regression analysis (P < .25). However, in multivariate logistic regression analysis, only monthly income, presence of chronic disease, difficulty in covering medical costs, knowledge, and attitude towards the SHI scheme remained associated with WTP for the SHI scheme. Workers with a monthly income of more than 10 000 Birr were 2.45 times more likely to be willing to pay for an SHI scheme than workers with a monthly income of less than 5000 Birr (AOR = 2.45; 95% CI: 1.14, 5.26). Respondents with chronic conditions were nearly 5 times more likely to pay for an SHI program than respondents with no underlying conditions (AOR = 4.61; 95% CI: 2.41, 8.82). Workers who had difficulty paying for health care were nearly 4 times more likely to pay for an SHI program than their counterparts (AOR = 3.55; 95% CI: 1.22, 10.29). The likelihood of paying for the SHI scheme was 2.35 times higher among respondents who had good knowledge of the SHI scheme compared to respondents with poor knowledge (AOR = 2.35; 95% CI: 1.17, 4.72). In addition, the odds of paying for the SHI scheme were almost 3 times higher among workers who had positive attitudes towards the SHI programs than workers with negative attitudes toward SHI programs (AOR = 3.16, 95% CI: 1.62, 6.18) (Table 5).
Factors associated with willingness to Pay for Social Health Insurance Scheme among health workers in Gedeo zone, Southern Ethiopia, 2022.
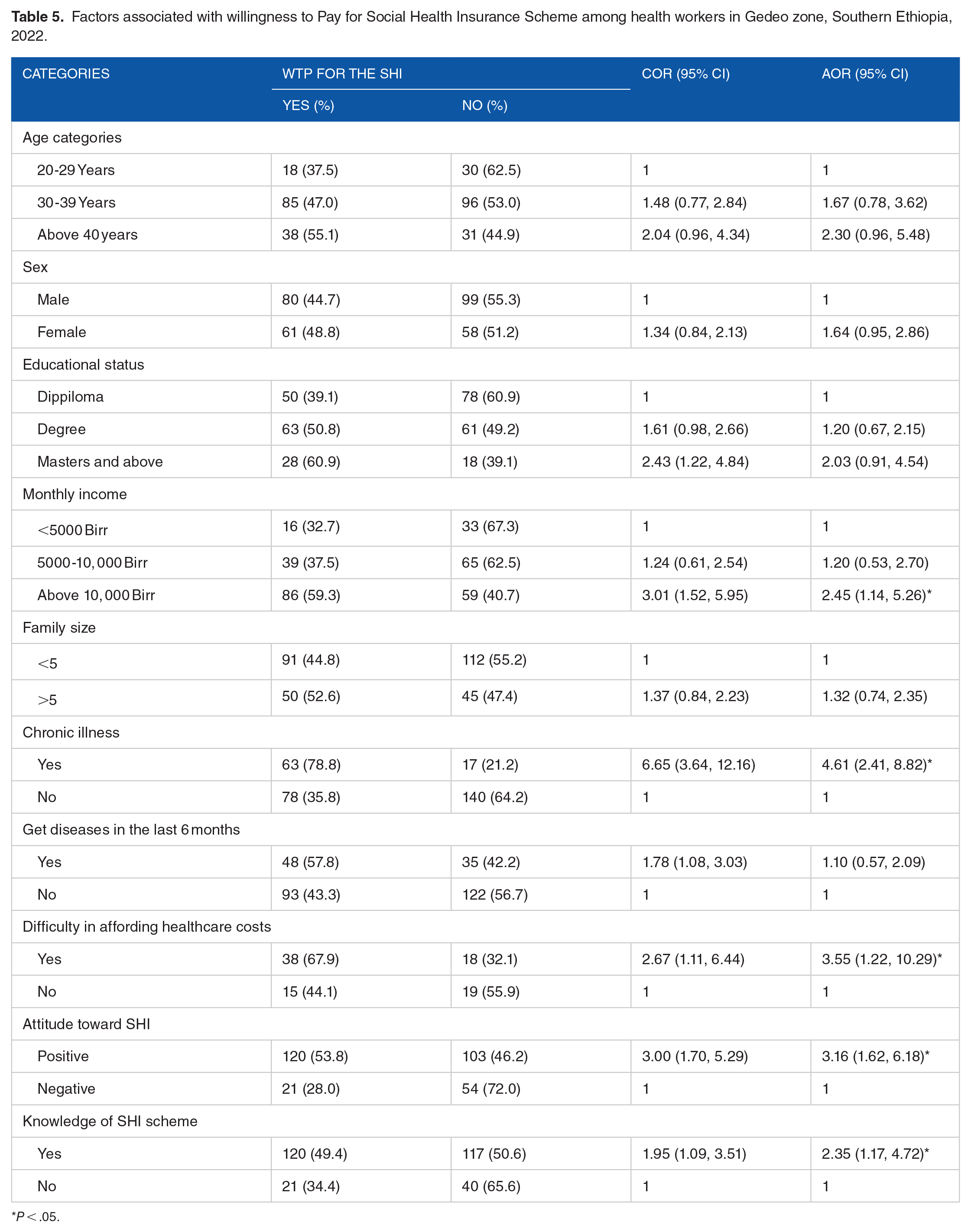
P < .05.
Discussion
Many developing countries including Ethiopia struggled to raise the required funds to deliver health services. Thus, there is interest in introducing the SHI scheme as a means of mobilizing more resources from the formal economy.8,33,34 Therefore, this study aimed to assess the determinants of willingness to pay for the SHI scheme among Healthcare providers in the Gedeo zone, Southern Ethiopia. This study revealed that 47.3% of healthcare providers were willing to pay the 3% monthly premium proposed for the SHI, which is in line with the findings of a study performed in South Sudan, 52%. 35 However, it is lower than studies conducted in Bangladesh, 80.1%, 36 Saudi Arabia, 77.9%, 37 Vietnam, 71.6%, 32 Nigeria, 82%, 38 and Mekele City, Ethiopia, 85.3%. 25 In addition, this study’s finding is higher than the studies performed in Malaysia, 33.2%, 39 Addis Ababa, Ethiopia, 28.7%, 26 Mujatown, Ethiopia, 37.6%, 31 and North Tigray, Ethiopia, 35.5%. 40 The possible reason for this variation might be related to differences in the study period, the study area, the population of the study, and the level of awareness, and perception of the SHI program. In this study, the overall mean amount of contribution the healthcare providers were willing to pay was 2.47% of their gross monthly wages. This finding is almost comparable with a study done in Addis Ababa, 2.5%, 30 and lower than the study conducted in Mekele Mekele City, Ethiopia, 3.6%. 25 The probable explanation for this difference might be due to the difference in socioeconomic factors, and methodology used to measure the level of contribution.
The economic status of respondents was a significant factor influencing the willingness to pay for the SHI program. Those healthcare providers who had a monthly income of greater than 10 000 Birr were almost 3 times more likely to pay for the SHI scheme compared to their counterparts. This finding is supported by studies conducted in India, 41 Nigeria, 42 Sierra Leone, 43 and Ethiopia, 22 which found increasing monthly salary has a significant relationship with WTP for the SHI schemes. This may be explained by the fact that healthcare providers with a rich wealth index can contribute to the SHI scheme at any price without difficulty. The odds of willingness to pay for the SHI scheme were almost 5 times higher among respondents who had chronic conditions compared to their counterparts. This finding is in line with a study done in Vietnam. 32 This is because respondents with a chronic illness may suffer from catastrophic medical expenses due to recurrent illnesses and willing to pay for the SHI. In this study, difficulty of covering costs of illness has a significantly positive relationship with WTP for the SHI program. The likelihood of paying for the SHI program were almost 4 times higher among healthcare providers who had difficulty paying for healthcare costs than their counterparts. This finding is supported by the findings of previous studies.22,24,27 This can be explained by the fact that people who have difficulty paying for medical care are more likely to pay for the SHI program because they fear catastrophic healthcare costs at the point of service.
The odds of willingness to pay for the SHI scheme were almost 2 times higher among respondents who had good knowledge of the SHI program than their counterparts. This is consistent with the results of studies conducted in Vietnam, 32 Mekele City, Ethiopia, 22 and Wolaita Sodo City, Ethiopia. 27 This can be explained by the fact that individuals who are knowledgeable about the SHI program can understand the benefits of supporting the SHI program to avoid catastrophic medical expenses.22,23 Those respondents who had a positive attitude towards the SHI program were almost 3 times more likely to pay for the SHI scheme compared to their counterparts. This finding was supported by studies conducted in Mekele, Ethiopia 22 and Gondar Town, Ethiopia. 23 This may be because workers with a positive attitude towards the SHI scheme have a better understanding of the concept and principles of the SHI scheme, which contributes to their WTP for the scheme.22,44
Study limitations
Although our study had a high response rate, there are several limitations. First, our study was not supported by qualitative methods to explore different determinants of WTP for the SHI program. Second, this study utilized a small sample size and was conducted only among public health workers, which may limit the generalizability of the findings to other employees.
Conclusions
More than half of healthcare providers surveyed were unwilling to pay for the SHI program. This study also found that respondents with higher monthly income, chronic diseases, difficulty paying medical bills, better knowledge, and positive attitudes towards the SHI program were significantly associated with WTP for the SHI scheme. Therefore, the health facility leadership should provide awareness creation on the benefits packages, concepts, and principles of the SHI program to increase the level of WTP for the program. In addition, the government should also improve the quality of healthcare services to improve the uptake of the SHI scheme.
Footnotes
Acknowledgements
We are deeply grateful to the Department of Public Health, College of Medicine and Health Sciences, Dilla University, for providing institutional ethical approval to conduct this study. Our appreciation also goes to the Gedeo Zone Health office, selected districts’ health offices, and the data collectors for their efforts and support during data collection.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AWK, GWO, MM, and GAZ designed the study. AWK, AKT, GWO, and MM prepared the data collection tools and trained the data collectors. AWK, GA, MM, and AH analyzed the data, interpreted the results, and wrote the manuscript and the final version of the manuscript. All authors read and approved the final manuscript.
Consent for Publication
Not applicable.
Ethical Consideration
This study was conducted in accordance with the principles of the Declaration of Helsinki and in accordance with the Ethiopian National Health Research Policy and Ethical Guidelines. We received ethical approval from the Institutional Review Board of the College of Medicine and Health Science, Dilla University (Ref no: duchm/irb/0109/2022). In addition, the purpose of the research was explained to the respondents and written consent was obtained before the interview. We have ensured the confidentiality of participant information by using a coding system and removing potentially personally identifiable information.
Availability of Data and Material
The datasets used or analyzed during this study were available from the corresponding authors upon reasonable request.