
Abstract
Background:
Early identification of people living with hepatitis B virus infection is required to initiate treatment and care, prevent community transmission, and expand vaccination. However, only an estimated 10% of people living with chronic hepatitis B infection are diagnosed, and only 2% are on treatment globally. This study aimed to assess the prevalence of hepatitis B virus infection and its associated factors among high school students in Shinshicho Town, southern Ethiopia.
Methods:
An institutional-based cross-sectional study was conducted among 380 high school students in Shinshicho Town, southern Ethiopia, from September to October 2022. A laboratory investigation of hepatitis B surface antigen was done to determine infection status. An odds ratio with a 95% confidence interval was used to declare statistical significance.
Results:
The prevalence of hepatitis B virus infection among high school students in Shinshicho town was observed to be 7.6% (95% CI: 5.5, 10.5%). Age 20 to 24 years [AOR: 2.7; 95% CI: (1.0-7.0)], rural residence [AOR: 3.4; 95% CI: (1.3-8.9)], and history of unprotected drug injection [AOR: 11.3; 95% CI: (3.7-34.8)] were independently associated with hepatitis B virus infection.
Conclusion:
A high prevalence of hepatitis B virus infection was observed among high school students in this study. Therefore, strengthening the school-based screen-and-treat program, especially targeting students from rural areas and young adults, and conducting awareness campaigns about the importance of practicing safe behaviors, such as avoiding unprotected drug injections, could contribute to the prevention and control of hepatitis B virus infection among high school students.
Keywords
Background
The hepatitis B virus is a highly infectious and life-threatening virus that attacks the liver. 1 The virus can be transmitted through exposure to infected blood and body fluids, sharing contaminated needles, syringes, or sharp objects, and mother-to-child contact during birth. 2 Due to the development of hepatitis B gene mutations, health system barriers, and social inequalities, infection with the virus continues to be a major public health priority. 3 Consequently, the patients may suffer from a poor prognosis, a high rate of mortality, and increased catastrophic costs. 4 Globally, there were an estimated 300 million people living with chronic hepatitis B infection and one million deaths annually. The Sub-Saharan Africa and Western Pacific regions together carry more than two-thirds (68%) of the global burden. 5
The World Health Organization (WHO) has set a strategy to eliminate viral hepatitis as a public health threat by 2030. The strategic targets were defined as a 90% reduction in new infections, 90% of infected people being diagnosed, 80% of eligible individuals receiving appropriate treatment, and a 65% reduction in mortality compared with the 2015 baseline. 6 To achieve these, it is recommended that all adults living in settings with an intermediate prevalence (⩾2%) or a high prevalence (⩾5%) of hepatitis B surface antigen (HBsAg) in the general population have access to and be offered HBsAg serological testing with linkage to treatment, care, and prevention services. 2 However, only an estimated 10% of people living with chronic hepatitis B infection are diagnosed and only 2% are on treatment globally. These imply that public health decision-makers and practitioners are facing practical challenges in preventing community transmission of the virus and treating the late complications, like liver cirrhosis, fibrosis, and hepatocellular carcinoma. Low- and middle-income countries share the majority of the problems, possibly due to limited access to laboratory infrastructure, antiviral therapies, diagnostic assays, low community awareness, and poor living conditions. 7
Hepatitis B virus infection is an endemic health problem in Ethiopia. 8 Therefore, early identification of people living with hepatitis B virus infection is required to initiate treatment and care, prevent community transmission, and expand vaccination. 9 Most of the previous studies were conducted among pregnant mothers, healthcare workers, blood donors, and college medical students. However, there is a paucity of information that clarifies the epidemiology of hepatitis B virus infection among high school students. This study aimed to assess the prevalence of hepatitis B virus infection and its associated factors among high school students (from 9-12 grades) in Shinshicho Town, southern Ethiopia. The findings may serve as a guide for public health authorities and healthcare providers in planning and implementing hepatitis B virus testing, treatment, and care services in schools.
Materials and Methods
Study design, area, and period
This institutional-based cross-sectional study was conducted among high school students in Shinshicho Town, southern Ethiopia, from September to October 2022. The town is located at a latitude and longitude of 7°12′N 37°46′E. The town has 3 high schools, namely Shinshicho, Metoma, and Kidus Antonios. 10
Participants and exclusion criteria
The study included all randomly selected students aged 15 years and older from the 3 high schools. Students who reported being on the hepatitis B virus vaccine were excluded from the study as the HBsAg result could turn out to be positive during the study period. Moreover, a few students who were unable to participate in the study due to different reasons were also excluded from this study.
Sample size and sampling procedure
Epi Info version 7 was used to determine the sample size of 400 by taking the 18.4% expected proportion of chronic hepatitis B virus infection, 11 4% margin of error, 95% confidence level, and 10% non-response rate. The 3 schools were stratified into 4 strata by grade level. Then, a total of 400 samples were proportionally allocated to each grade (ie, Shinshicho high school: grade 9 (50 from 190 students), grade 10 (39 from 150 students), grade 11 (78 from 296 students), and grade 12 (87 from 330 students), Metoma high school: grade 9 (42 from 160 students), grade 10 (43 from 162 students), grade 11 (15 from 58 students), and grade 12 (14 from 54 students), and Kidus Antonios high school: grade 9 (13 from 50 students), grade 10 (9 from 34 students), and grade 11 (10 from 40 students). The data were collected from every fourth student in the sampling frame.
Data collection and laboratory procedure
Data on sociodemographic characteristics, risky behaviors, and histories of sexual and reproductive health were collected by 2 laboratory technicians using a pre-tested questionnaire. After completing the interview questionnaire, HBsAg laboratory investigation was done to determine the status of the hepatitis B virus infection. The 3 ml of whole blood were collected through a needle puncture of the vein with a sterile syringe. The whole blood sample was collected in an EDTA test tube and transported in an ice bag. Plasma was separated by a centrifuge force of 3000 RPM for 5 minutes. Then, 3 drops (120 µl) of plasma were taken and added to the Advanced Quality™ 1 step HBsAg test kit (InTec Products, Xiamen, China). The test has 100% sensitivity, 99.4% specificity, and 98.6% positive predictive value. The result was read after 15 to 30 minutes. The intensity of the color in the test line region (T) varied depending on the concentration of HBsAg present in the specimen. Therefore, any shade of color in the test region (T) was considered positive. 12
Data quality control
The questionnaire was translated into Amharic, the official language, and back to English. Pre-testing of the questionnaire was done on 21 students at Lesho High School who had characteristics nearly similar to those of high schools in Shinshicho town. Training was given to data collectors and supervisors on how to obtain ethical consent, conduct interviews, collect sample blood, perform laboratory procedures, and keep records. Confirmatory laboratory tests were done for all test results by using known negative and positive controls. The data’s completeness and consistency were checked on a daily basis.
Data management and statistical analyses
The data were entered into EpiData version 4.6 and analyzed on SPSS version 25. Frequency and percentage were used to present the findings. All independent variables were fitted separately into a bivariate logistic model to estimate the degree of association with hepatitis B virus infection among students. Then, variables with a P-value ⩽.25 were fitted into a multivariable logistic model to control for confounders. The statistical significance was declared by using an odds ratio (OR) with a 95% confidence interval.
Operational definitions
Hepatitis B surface antigen (HBsAg): refers to a protein on the surface of the hepatitis B virus whose presence in the serum indicated that the student was infected with the hepatitis B virus.
HBsAg positive: if 2 distinct red bands appeared in the test region and another in the control region, then it indicated that the student was infected with the hepatitis B virus.
HBsAg negative: if a single red band appeared in the control region and no apparent red or pink band in the test region, then it indicated that the student was not infected with the hepatitis B virus.
HBsAg invalid: if the control band failed to appear due to improper testing procedures or deterioration of reagents, then the test was repeated because it was difficult to conclude the status of the hepatitis B virus.
History of unprotected drug injection: refers to the history of drug administration by an unskilled person with an unsterile procedure.
Results
Sociodemographic characteristics
In this study, data were collected from 380 students, giving a response rate of 95%. Of these, 55.8% were female, and 69.2% were in the age group 15 to 19 years. The mean age of the students was 18.5 years, with a standard deviation of 2. About 94.5% were from the Kembata ethnic group, 73.7% were protestant religion followers, 93.7% were single by marital status, 26.3% were in grade 9, and 66.6% were urban residents. The majority (61%) of students’ families earned a monthly income of Birr 600 to 5000 [USD 11.3-94.1] (Table 1).
Sociodemographic characteristics of high school students in Shinshicho Town, southern Ethiopia, 2022.

History of sexual and reproductive health
About 11.8% of students had a history of sexual practice (heterosexual intercourse). Of female students, 44.2% had a history of genital mutilation, and 3.9% had a history of abortion.
Risky behaviors
A total of 50 students (13.2%) had body tattooing, 55.5% pierced their ears and/or bodies, 7.4% injected unprotected drugs, 16.3% had a history of tooth extraction in traditional ways, 2.1% had a history of contact with a hepatitis B virus-infected person, 37.6% shared sharp instruments, and 97.4% did not have a test for the hepatitis B virus in the past year.
Magnitude of hepatitis B virus infection
Twenty-nine students [7.6% (95% CI: 5.5, 10.5%)] were diagnosed with hepatitis B infection. Of these, 89.7% were female, 65.5% were rural residents, and 58.6% had experience of sharing sharp instruments.
Factors associated with hepatitis B virus infection
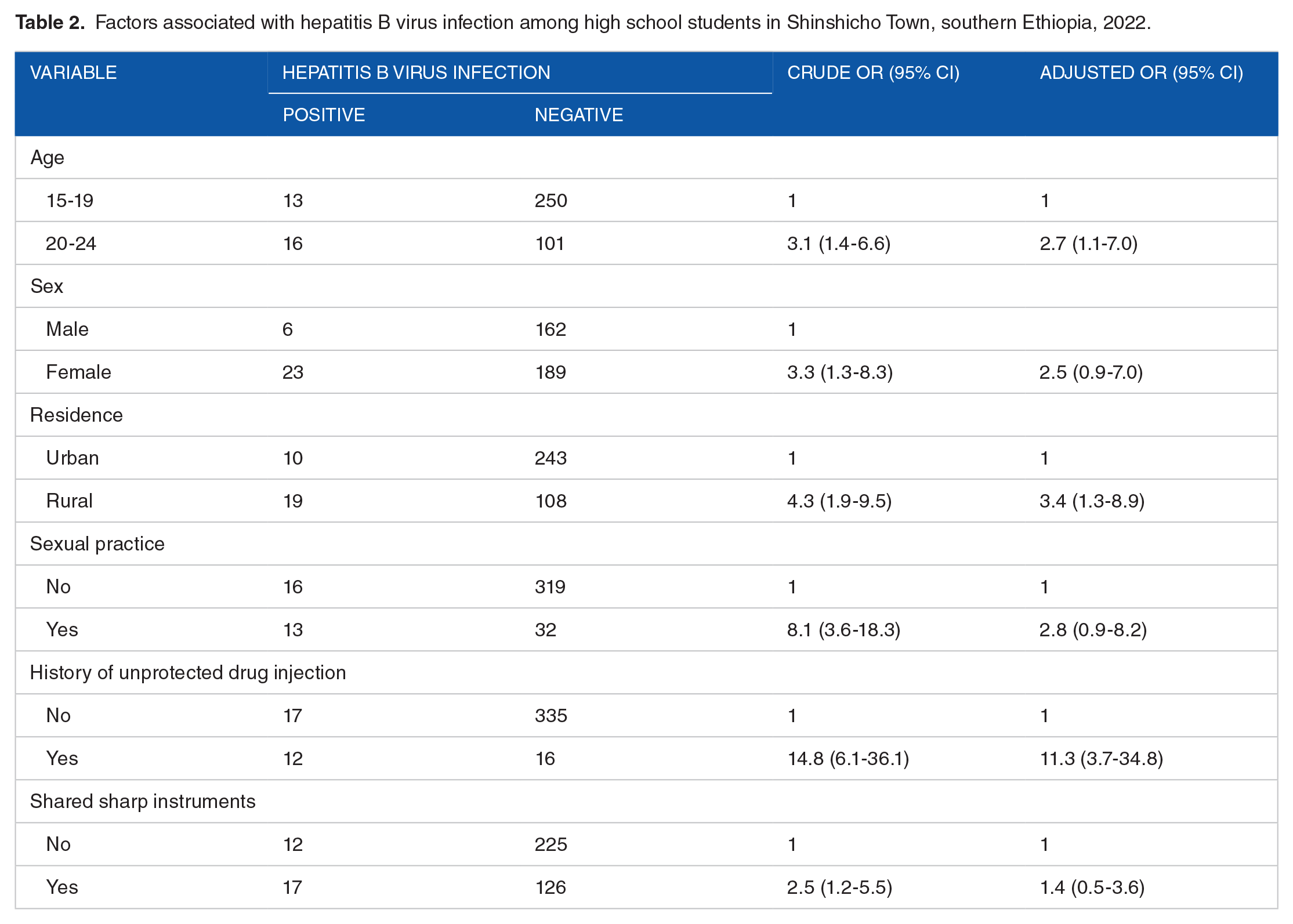
Age, sex, residence, sexual practice, history of unprotected drug injection, and sharing sharp instruments had an association with hepatitis B infection at a P-value ⩽ .25 in bivariate logistic regression analyses. However, only age 20 to 24 years [AOR: 2.7; 95% CI: (1.1-7.0)], rural residence [AOR: 3.4; 95% CI: (1.3-8.9)], and history of unprotected drug injection [AOR: 11.3; 95% CI: (3.7-34.8)] remained statistically significant at a P-value ⩽ .05 (Table 2).
Factors associated with hepatitis B virus infection among high school students in Shinshicho Town, southern Ethiopia, 2022.
Discussion
This study aimed to assess the prevalence of hepatitis B virus infection and its associated factors among high school students in Shinshicho Town, southern Ethiopia, in 2022. The study revealed that the prevalence of hepatitis B virus infection was 7.6% (95% CI: 5.5, 10.5%). Additionally, age 20 to 24 years, rural residence, and history of unprotected drug injection were independently associated with hepatitis B virus infection.
The prevalence of hepatitis B virus infection among high school students in Shinshicho Town was observed to be 7.6%, which was categorized as a high-burden setting according to the WHO classification. 2 This was higher than the 2.6% prevalence of hepatitis B virus infection detected among medical waste handlers and healthcare workers in primary hospitals in northwest Ethiopia. 13 The discrepancy could be explained by the fact that hospital workers might follow and apply infection prevention procedures more strictly compared to high school students. This was because hospital workers had better awareness about the mechanism of hepatitis B virus transmission due to their professional background, frequent infection prevention and control training, and regular safety supervision. Nevertheless, previous studies have revealed that a nearly consistent prevalence of hepatitis B virus infection was observed among pregnant women, commercial sex workers, people living with human immunodeficiency virus (HIV), and blood donors, implying that high school students are at increased risk for hepatitis B virus infection.14,15 Therefore, strengthening hepatitis B virus infection prevention activities in high schools is required to reduce virus transmission among the students.
This study indicated that there was a statistically significant association between the age of high school students and hepatitis B virus infection. Compared to late adolescents (aged 15-19 years), the odds of being infected with the hepatitis B virus were about 3 times more likely among young adults (aged 20-24 years). This could be justified by the fact that young adults were more likely to engage in risk-taking behaviors as well as unprotected sexual practices, which might increase their risk of exposure to hepatitis B virus infection. 16 Hence, school-based hepatitis B virus prevention activities should be age-sensitive.
The odds of being infected with the hepatitis B virus among high school students who lived in rural areas were more than 3 times higher compared to those who lived in urban areas. The possible reason could be that students living in rural areas might experience risky traditional practices like tonsillectomy, tattooing, ear piercing, ritual scars, circumcision, traditional surgery, unsterilized hearing shaving, home delivery, dental extraction at home, and unsafe abortion.15,17,18 Thus, strengthening school-based hepatitis prevention and control programs, such as vaccination, routine screening and treatment of carriers, and the provision of health education, could reduce the risk of virus transmission.
A history of unprotected drug injections was independently associated with hepatitis B virus infection among high school students. A study conducted in Hawassa, southern Ethiopia, also indicated that people who had a history of unprotected drug injection were more likely to be infected with the hepatitis B virus compared to those who did not have a history of unprotected drug injection. 19 The possible explanation could be that drug injectors might use unsterile needles or share needles with other drug injectors. This behavior increases the risk of transmitting the hepatitis B virus, as contaminated needles can easily spread the infection from 1 person to another. Hence, school-based hepatitis prevention and control activities should include educating students about the risks of practicing drug injections.
Ethiopia has recognized the public health and clinical burdens of viral hepatitis and is working to eliminate it by 2030. In 2016, the government developed its first national strategic plan document, providing a comprehensive strategy, key interventions, program coordination and partnership, and monitoring and evaluation of the viral hepatitis program in the country. Many remarkable achievements have been recorded following the implementation of this strategic plan. For example, the hepatitis B vaccine has been integrated within the childhood immunization program, universal precaution and infection prevention activities have been implemented at all levels of the health system, screening blood for hepatitis B virus has been implemented by the national blood bank service, the hepatitis B virus prevention and control program has been integrated with national HIV services, and a national viral hepatitis technical working group has been established. 20 Hence, the findings of this study will serve as additional input to improve hepatitis B virus prevention and control services at high schools in the study area and similar settings.
The findings of this study should be interpreted in light of its limitations. Due to the cross-sectional nature of the study, causality between the independent variables and hepatitis B virus infection could not be established. Students might also provide only socially desirable responses, such as a history of abortion, unprotected drug injection practices, shared sharp instruments, and tooth extraction, which would introduce bias.
Conclusion
A high prevalence of hepatitis B virus infection was observed among high school students in this study. Therefore, strengthening the school-based screen-and-treat program, especially targeting students from rural areas and young adults, and conducting awareness campaigns about the importance of practicing safe behaviors, such as avoiding unprotected drug injections, could contribute to the prevention and control of hepatitis B virus infection among high school students.
Footnotes
Acknowledgements
The authors wish to thank the Shinshicho Town educational offices for their logistical and administrative support. They also extend their deepest gratitude to the data collectors, supervisors, and study participants for making this study possible.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ Contributions
DT, ST, TE, and TT conceived, designed, and conducted the study. ST, TE, and TT supervised and provided mentorship. DT, ST, TE, and TT were involved in the analysis and interpretation of the findings. ST wrote the manuscript. All authors have approved the final version of the manuscript.
Ethics and Consent
Ethical approval was received from the Institutional Review Board of Wachemo University via the School of Graduate Studies (Ref No: 880/14). Written informed consent was obtained from students aged 18 and older. Written informed consent was obtained from parents or guardians for students below the age of 18. Written assent was also obtained from children 15 to 17 years of age.