
Abstract
Background
Hepatitis B virus (HBV) infection is highly endemic in Nigeria. The primary objective of this study is to describe the knowledge, self-reported vaccination status, and intention of healthcare workers to receive hepatitis B vaccine at a tertiary referral center in conflict-ravaged northeastern Nigeria.
Methods
This was cross-sectional analytical study among medical practitioners, nurses, laboratory workers, health attendants, pharmacists, and radiographers working at Federal Medical Center Nguru, Yobe State. Written informed consent was obtained from all study participants. Data were obtained using questionnaires and entered into a Microsoft Excel spreadsheet, cleaned and analyzed using JMP Pro software.
Results
Of the 182 participants, we found that 151 (82.97%), 81 (44.51%), 85 (46.70%), and 33 (18.13%) had good knowledge of HBV, good knowledge of hepatitis B vaccine, were vaccinated against HBV by the least dose, and had a complete hepatitis B vaccination status, respectively. The lack of availability of the vaccine was the main reason for not receiving the vaccine among the unvaccinated 36/91 (39.56%), followed by not knowing where to access the vaccine 19/91 (20.88%).
Conclusion
The study highlights the need for strategies to ensure the availability of hepatitis B vaccine in conflict settings and need for vaccinology training given the suboptimal level of awareness and uptake of the hepatitis B vaccine among the healthcare workers.
Keywords
Introduction
The World Health Organization African region and the western Pacific region are the regions of the world worst hit by the hepatitis B virus (HBV) epidemic. 1 A total of 150 million people were said to be living with chronic HBV infection worldwide in 2015. 1 The estimated population prevalence of chronic HBV infection in Nigeria is high and adds to the urgency of protecting healthcare workers who provide clinical care. 2 Moreover, 90% of the global occupational exposure to bloodborne pathogens occur in resource-limited countries with 66,000 HBV infections each year worldwide.3,4 Abubakar and colleagues reported that 8.7% of the source of occupational exposure to body fluids were positive to hepatitis B surface antigen at a tertiary referral center in Nigeria. 5 Therefore, improving hepatitis B vaccine coverage of healthcare workers in sub-Saharan Africa is an important public health issue; studies that document barriers and facilitators to full coverage in specific settings are a critical element of this effort.
Hepatitis B vaccine is highly immunogenic with 90–100% protection conferred following a completed hepatitis B vaccination schedule among infants, children, and adults. 6
The majority of operating room personnel are aware of the hepatitis B vaccine in Nigeria, 7 but only 26.8% of them were vaccinated against HBV in Nigeria. 7 The story is not different in the Republic of Georgia where only 12% of healthcare workers were vaccinated. 8 In the United States, the hepatitis B vaccination coverage among healthcare workers was 69.5%. 9 It is noticeable that these vaccination coverages are well below the Healthy People 2010 goal of 90%. 9
Previous studies have suggested policies and interventions to address the healthcare needs of people affected by conflict.10,11 In areas of conflict, the supply of drugs and vaccines is halted, health infrastructure is often destroyed, and health professionals may flee. 12 In addition, health facilities are flooded with multiply injured patients making the immune protection of the healthcare worker from occupational exposure to blood and blood-borne pathogens a cause for concern. Researchers are therefore encouraged to advocate for, and conduct relevant surveys within, settings afflicted by conflicts. 13
Few studies determine the knowledge, practice, and intention of healthcare workers to receive hepatitis B vaccine in Nigeria, making it challenging to mount prevention and control programs among this high-risk group working in conflict areas. The main objective of this study is to describe the knowledge, self-reported vaccination status and intention of healthcare workers to receive hepatitis B vaccine at a tertiary referral center in conflict-savaged northeastern Nigeria.
Methods
Ethics approval
Ethics approval to conduct the study was obtained from the ethical committee of the Federal Medical Center, Nguru (approval number 30/05/2017-05/06/2017). The ethical committee was certified by the Nigerian National Health Research Ethics Committee. Written informed consent was obtained from all study participants. The authors complied with all ethical regulations.
Study design
This cross-sectional analytical study took place between 21 June and 30 July 2017 among healthcare workers of the Federal Medical Center, Nguru.
Study setting and site
The study was undertaken among healthcare workers at the Federal Medical Center, Nguru, Yobe State, a tertiary referral hospital in northeastern Nigeria. The hospital is situated in a semiurban metropolis located in northeastern Nigeria, ravaged by conflict since August 2011. 14 The Boko Haram insurgency is characterized by the use of crude weapons to terrorize and kill security agents and members of the public, as well as kidnappings and use of women and children as suicide bombers in markets, motor parks, places of worship, schools, hospitals, and security posts. 15 Healthcare workers have been killed, abducted, or displaced due to the Boko Haram insurgency.15,16 Yobe State was declared a state of emergency during peak periods of the attacks. 16 A reduction in access to healthcare and immunization has been reported in areas afflicted by the Boko Haram insurgency. 17 Additional challenges to the access and functionality of healthcare were posed by counter-insurgency operations, such as banning of motorcycles and temporary interruption of cellphone services during major anti-insurgency operations. 16
The hospital has a bed capacity of about 150 and serves as a tertiary referral center in northeastern Nigeria. There is no staff dedicated to infection control and prevention in the hospital. Healthcare workers can access hepatitis B immunization services free of charge at the routine immunization clinic, where hepatitis B vaccine is provided to children under 5 years of age. It is not mandatory for healthcare workers to receive hepatitis B vaccine as part of workplace safety in Nigeria.
Study participants
Study participants comprised hospital workers having direct contact with patients, that is, medical practitioners, nurses, laboratory workers, health attendants, pharmacists, and radiographers working at the hospital. Single-population proportion formula was used to determine the sample size for this study. We considered a 95% level of confidence, a 5% error margin, and proportion of healthcare workers who were aware of hepatitis B vaccine 86.6%, 7 to arrive at the required sample size for the study. Eligible study participants were selected using a simple random sampling technique. The sampling frame comprised a list of healthcare workers obtained from the human resource development office of the hospital.
Data collection
Data were collected from respondents using a standardized self-administered questionnaire developed from questionnaire used in a previous study. 18 Hard copies of the questionnaires, provided in English language, were distributed to study participants by research assistants. The purpose of the study was explained, and written consent obtained from the study participants. The participants had an opportunity to contact the research team for clarity on the questions in the questionnaire if the need arose. The questionnaires were completed and returned within an hour or by the end of the working day. Questionnaires were coded with numbers and did not have any personal identification to maintain privacy and confidentiality. The questionnaire was pretested on 10 healthcare workers selected randomly, and after that, validated and modified, as appropriate.
There were multiple sections in the questionnaire that covered: demographic characteristics of study participants; knowledge of HBV and hepatitis B vaccine; the practice of hepatitis B vaccination and stated intention to receive the vaccine among the unvaccinated. Only closed-ended questions were included in the questionnaire.
Scoring
Scores of 1 or 2 and 0 were applied to correct and wrong responses, respectively, for graded questions. The section on sociodemographic information was not graded/scored. Knowledge on HBV, knowledge on hepatitis B vaccine and self-reported hepatitis B vaccination status scores for each study participant were obtained out of a possible maximum of 8, 24 and 3, respectively. Scores of ⩾7 and ⩾17 were considered good for knowledge on HBV and knowledge on hepatitis B vaccine, respectively, based on the distribution of respondent scores that was higher than the mean score. Respondents that received at least three shots of hepatitis B vaccine were considered to have complete hepatitis B vaccination status.
Statistical analysis
The data from the questionnaires were entered into a Microsoft Excel (Version 2013; Microsoft Corporation, Redmond, WA, USA) spreadsheet and cleaned. Data from the Excel spreadsheet were then exported to, and analyzed using, JMP Pro software (JMP Version 12.0.1, SAS Institute Inc., Cary, NC, USA). Using descriptive statistics, results were presented as frequencies and percentages. Odds ratios and 95% confidence intervals (CIs) were computed to describe predictors of good knowledge and good practice. Relative risks (RRs) and 95% CIs were computed to describe factors associated with the intention to receive the hepatitis B vaccine among the unvaccinated.
Results
Study population and demographic characteristics
Out of 232 questionnaires distributed, 50 were excluded due to missing data (32) or nonresponses (18). As shown in Table 1, out of the 182 participants, 135 (74%) were males, 148 (81%) were married, 42 (23%) were medical practitioners and 115 (63%) had 0–9 years of service. The median age of the respondents was 34 years. There were 39 (21%), 102 (56%), 28 (15%) and 13 (7%) respondents in the ⩽29 years, 30–39 years, 40–49 years and 50 years or older age groups, respectively.
Demographic and occupational characteristics of healthcare workers who responded to the survey regarding their knowledge of hepatitis B virus, hepatitis B vaccine, and their self-reported vaccination status.

CI, confidence interval; OR, odds ratio.
Knowledge of HBV infection
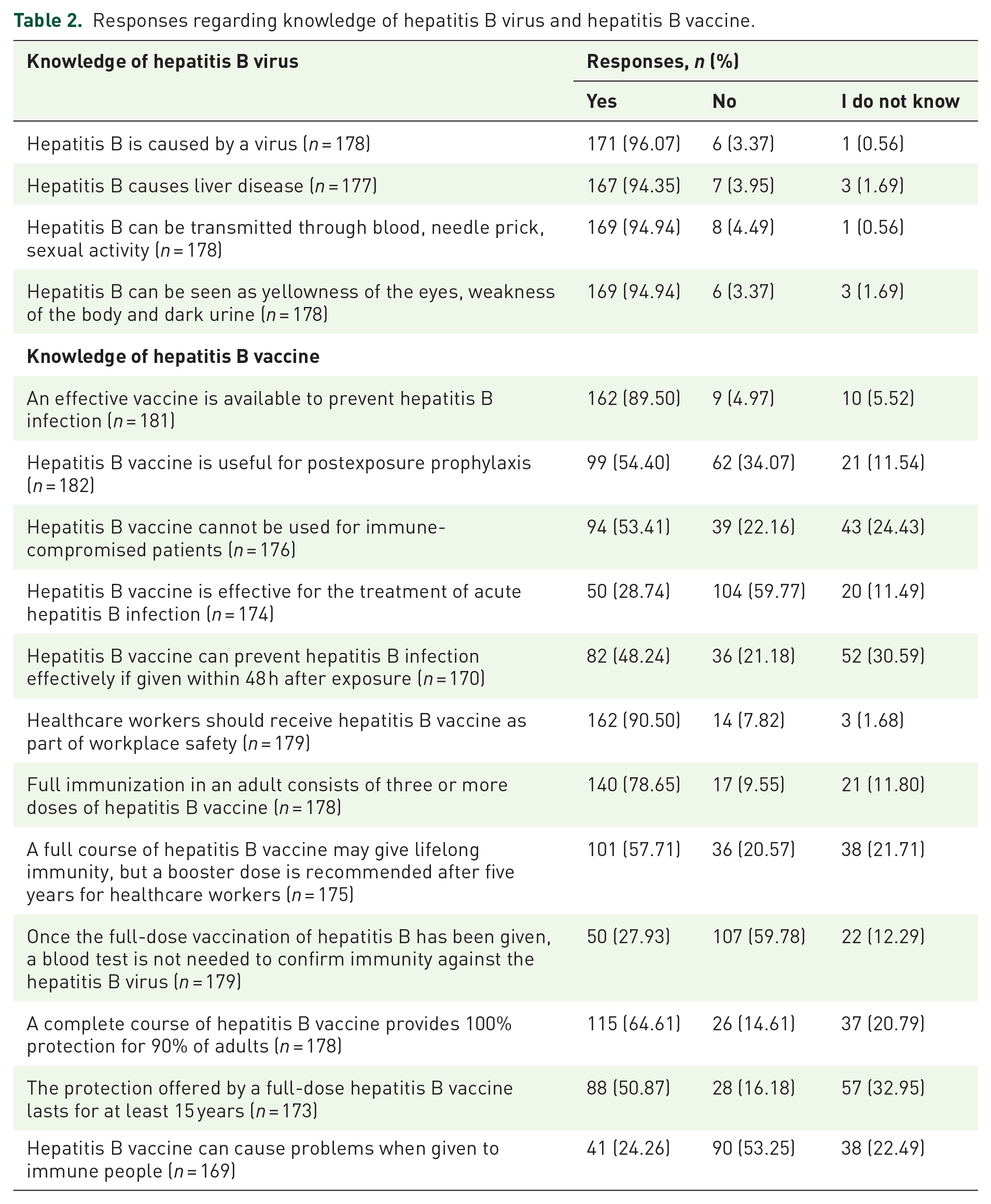
As shown in Table 1, out of 182 respondents, 151 (82.97%) had good knowledge of HBV. This finding does not differ across age groups, sex, healthcare category, and years of practice. As shown in Table 2, the majority of respondents correctly identified that hepatitis B disease is caused by a virus (96.07%), causes liver disease (94.35%), is transmitted through blood, needle prick, sexual activity (94.94%) and presents clinically with yellowness of the eyes, weakness of the body, and dark urine (94.94%).
Responses regarding knowledge of hepatitis B virus and hepatitis B vaccine.
Knowledge of hepatitis B vaccine and self-reported vaccination status
Of the 182 respondents studied, 81 (44.51%) had good knowledge of hepatitis B vaccine (Table 1). This finding is not statistically different across sociodemographic and occupational characteristics of the participants. As shown in Table 2, fewer respondents correctly identified that there is an effective vaccine for the virus (89.50%), that the vaccine is used for postexposure prophylaxis (54.40%), and that the vaccine is highly effective in preventing HBV infection if given within 48 h after exposure (48.24%).
Only 85/182 (46.70%) and 33/182 (18.13%) of the respondents were vaccinated against hepatitis B with the at-least a dose and at-least three doses, respectively (Table 3).
Practice of hepatitis B vaccination, occupational exposure, and self-reported hepatitis B infection.

Of the participants that had not received the vaccine before, 4/97 did not respond to this question.
HBsAg, hepatitis B surface antigen.
Reasons for receiving the vaccine among the vaccinated
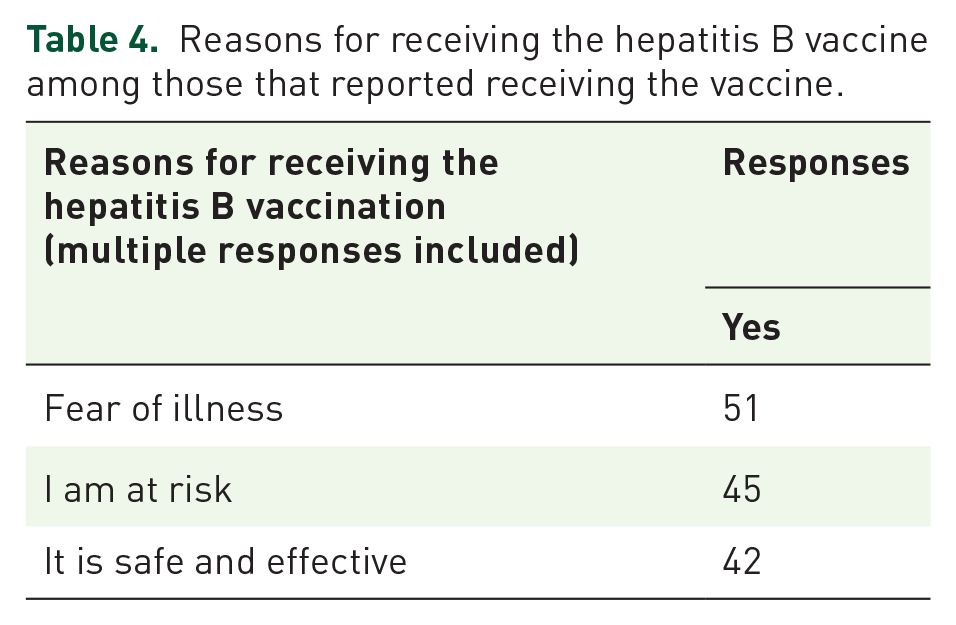
The most commonly reported reasons for receiving the hepatitis B vaccine was fear of illness caused by the virus followed by being at risk of infection and the safety and effectiveness of the vaccine (Table 4).
Reasons for receiving the hepatitis B vaccine among those that reported receiving the vaccine.
Reasons for not receiving the vaccine among the unvaccinated
As depicted in Table 5, the lack of availability of the vaccine was the main reason for not receiving the vaccine among the unvaccinated 36/91 (39.56%), followed by not knowing from where to get the vaccine 19/91 (20.88%). The majority of the unvaccinated intend to receive the vaccine in the future 76/91 (83.52%). Among the unvaccinated, those that do not intend to receive the vaccine in the future are more likely to report that they are not at risk of getting the infection (RR = 6.43, 95% CI: 3.97–10.40) and that god will protect them from getting the infection (RR = 2.95, 95% CI: 1.15–7.52) compared with those that intend to receive the vaccine in the future (Table 5).
Reasons for not getting the vaccine among the unvaccinated and their intention to receive the vaccine in the future.

These reasons were listed in the questionnaire as options.
CI, confidence interval.
Occupational exposure and self-reported history of having HBV infection
As shown in Table 3, 103/175 (58.86%), 129/177 (72.88%) and 38/177 (21.47%) of the respondents reported having had an accidental exposure to blood or body fluids of patients, were ever screened for hepatitis B surface antigen (HBsAg), had a history of having hepatitis B disease/positive HBsAg screen, respectively.
Discussion
Our study has shown that majority of respondents have poor knowledge of hepatitis B vaccine and poor hepatitis B vaccination status, despite the majority having good knowledge of the HBV. We have also shown that the most frequent reason for receiving the vaccine was fear of illness caused by the virus and the commonest reasons for not receiving the vaccine was the lack of availability of the vaccine and not knowing from where to access it. Furthermore, the majority of the unvaccinated intend to receive the vaccine in the future.
Knowledge of HBV infection
Similar to our findings, the majority of respondents had good knowledge of HBV infection in studies conducted in northwestern Nigeria, 19 southern Nigeria,7,20 and other parts of the world.21–23
Knowledge of hepatitis B vaccine and self-reported vaccination status
Our findings are similar to those in Pakistan 24 but differ from those in Cameroon, where the majority of respondents had good knowledge of the hepatitis B vaccine. 25 In our study, the majority of respondents were aware of the existence of an effective vaccine to prevent HBV infection and that the vaccine should be given to healthcare workers as part of workplace safety, but few received at-least dose of the hepatitis B vaccine. Although hepatitis B vaccine is part of the expanded program of immunization and national immunization program in Nigeria, it is not mandatory for healthcare workers to receive the vaccine as part of workplace safety. This may partly be responsible for the poor vaccination status of the majority of respondents in our study and many other previous studies within and outside Nigeria.7,9,21,22,25–29
The poor knowledge of the utility of the vaccine for postexposure prophylaxis, coupled with poor hepatitis B vaccination status among the healthcare workers is a serious concern, and calls for urgent need for infection prevention and control education to guard the safety of the healthcare workers.
Reasons for receiving the vaccine among the vaccinated
We found that the most commonly reported reasons for receiving the hepatitis B vaccine were fear of illness caused by the virus followed by being at risk of infection and the safety and effectiveness of the vaccine. This is similar to findings in the United States, where the decision to accept or reject hepatitis B vaccine was determined by the beliefs of the healthcare providers regarding the safety and efficacy of the hepatitis B vaccine. 30 Various studies have used the health-belief model to examine the uptake of vaccination.31,32 The internal locus of control refers to the belief in the power of self in the control of disease; the powerful-others locus of control is the belief in the power of others in the control of disease; while the chance locus of control is the belief in the power of chance in the control of disease.30,33–35 These beliefs may play a role in acceptance or declining vaccination.
Reasons for not receiving the vaccine among the unvaccinated
We found that lack of availability of the vaccine was the main reported reason for not receiving the vaccination among the unvaccinated, followed by not having the knowledge of where to get the vaccine. These challenges should be urgently addressed, especially given that the majority of the unvaccinated in our study intend to receive the vaccine in the future. The State Ministry of Health changed drug, vaccine, and consumable deliveries to 3 months from the usual 1 month to minimize stockout. However, out-of-stock drugs, vaccines, and consumables occurred in health facilities in Yobe State during peak periods of the insurgency. 16 The demand in health services fluctuates across facilities during peak periods of the insurgency. For instance, it is reported that during the third quarter of 2012, facility-attended deliveries in Nguru rose sharply to 835 deliveries compared with 111 deliveries in the previous quarter. 16 In Damaturu, the numbers declined to 21 deliveries compared with 797 deliveries over the same period. 16 By the second quarter of 2013, Nguru experienced reduced numbers of deliveries to previous levels, while Damaturu experienced a sharp rise. 16 The pattern reversed again by the third quarter of 2013. 16 These fluctuations are largely due to immigration of people to areas perceived as safe, depending on where the insurgents intensify their activities at a time. 16 Hepatitis B vaccine stockouts are likely to occur when large, unanticipated deliveries occur that increase demand for vaccines. Other conflict areas are affected differently. In war-torn countries, there is limited space for health interventions, as evidenced by the continued prevalence of polio in countries afflicted by civil unrest. 36 In war-torn Syria, up to 90% of pharmaceutical products that the country produced before the conflict has been reduced, leading to a substantial shortage of essential medicines. 37
On the other hand, having no knowledge of where to obtain the vaccine, reported by the healthcare workers as a reason for not receiving the vaccine, is a cause for concern. The fact that some of the healthcare workers were not aware that the vaccine could be obtained at the under 5s immunization clinics, when available, signifies a gap in the hospital infection prevention and control program.
We found a statistically significant difference in reporting not been at risk of getting HBV infection among the unvaccinated not intending to receive the vaccine in the future compared with those intending to receive it. However, this finding should be interpreted with caution, given the small absolute difference in counts. The finding that some unvaccinated healthcare workers not intending to receive the vaccine in the future reported reliance on powerful-others locus of control to provide protection against hepatitis B highlights the importance of motivational factors as predictors of health behavior in healthcare planning. This concept was demonstrated among young women whose decision to receive human papilloma vaccine was fourfold greater when they received a strong recommendation for the vaccine versus those who did not. 32
Healthcare professionals have a responsibility to understand the challenges of the complex environments in which they work and adapt workable interventions accordingly. 10
Occupational exposure and self-reported HBV infection
Our finding that the majority of respondents reported having had an accidental exposure to blood or body fluids of patients, and that some of the healthcare workers reported having hepatitis B disease/positive HBsAg screen, further buttresses the need for infection-control-program improvement in the health facility, and the need to ensure availability of the hepatitis B vaccine, even in this setting afflicted with conflict. In the interest of prevention and control of nosocomial infections, the 21.5% of healthcare workers who self-reported having a history of HBV infection or an HBsAg-positive test should go for management of HBV infection if they had not been on any treatment regimen following their diagnosis.
The major limitation of this study is the use of the self-report method to assess the uptake of hepatitis B vaccination which is subject to recall bias. Therefore, the assessment of hepatitis B vaccination status should have been confirmed by examining employee health records where they exist and perhaps by measuring the serum anti-HBS antibody titer of the respondents. Hence an elaborate infection prevention and control program that keeps up-to-date confidential employee health records is recommended in Nigeria. Another limitation of the results is the overall small sample size.
Despite these limitations, to the best of our knowledge, our study was the first to describe vaccination-related knowledge and status among healthcare workers specifically in settings most affected by civil conflict in Nigeria. Gaps have been identified in availability and access to hepatitis B vaccine in conflict settings, with resulting poor vaccination status of healthcare workers. This highlights the need for deliberate efforts to counteract the challenges affecting healthcare delivery in conflict settings and the need for vaccinology training given the suboptimal level of awareness and uptake of the hepatitis B vaccine among the healthcare workers.
Footnotes
Acknowledgements
We acknowledge the research assistants that assisted with data collection.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.