
Abstract
Viral hepatitis is a disease of great concern to public health that is now met by a favorable momentum to combat the global epidemic. This article is intended to highlight the importance of viral hepatitis in the Vietnam population as well in the group of people living with HIV/AIDS (PLWHA). We reviewed available data on epidemiology and response on hepatitis B virus (HBV) and hepatitis C virus (HCV) and HIV coinfection in Vietnam. The hepatitis B surface antigen (HBsAg) prevalence in the general population ranged from 5.7% to 24.7%. The anti-HCV prevalence ranged from 0.38% to 4.3% in the general population, while among people who inject drugs (PWIDs) it ranged from 31% to 97.2%. The HBV prevalence among PLWHA is similar to the general population, while HCV/HIV coinfection is concentrated in some groups. Anti-HCV prevalence among HIV-infected PWIDs can be as high as 98.5%. Developing policies for diagnosis and treatment of chronic HBV and HCV infections are critical priorities in order to prevent clinical progression to cirrhosis and liver cancer.
Introduction
July 28, 2011, marked the first ever World Hepatitis Day. The Day was established following the World Health Assembly’s adoption of the resolution on viral hepatitis at its 63rd meeting 1 in 2010. In 2011, the US Department of Health and Human Services also released its first National Action Plan for the Prevention, Care, and Treatment of Viral Hepatitis, 2 in 2011. Globally, a momentum is building to combat the “silent” epidemic of viral hepatitis.
The epidemic has been called silent as the awareness on viral hepatitis has been disproportionately low among general public, policy makers, and health care workers, compared with its considerable disease burden. An estimated 57% of cases of liver cirrhosis and 78% of cases of primary liver cancer result from hepatitis B or C virus infection. 1 Approximately 2 billion people have been infected with hepatitis B virus worldwide, of whom more than 350 million are chronically infected, and between 500 000 and 700 000 people die annually as a result of hepatitis B virus infection. 1 –3 Some 130 to 170 million people are chronically infected with hepatitis C virus, and more than 350 000 people are estimated to die from hepatitis C-related liver diseases annually. 1 –3
In this article, we review the available data and information on the epidemiology and current response to hepatitis B and C, and HIV coinfection in Vietnam, and propose future intensified intervention to combat this “silent” epidemic.
Methods
We searched peer-reviewed articles on PubMed, using keywords “hepatitis B,” “hepatitis C,” and “HIV” in combination with “Viet Nam.” The authors met clinical and public health experts working on hepatitis and HIV at national and international organizations based in Vietnam and obtained information through interviews. Relevant references from the articles and information obtained in the interviews were also reviewed. Gray literature was also searched using Internet search engines in order to identify nonindexed materials. Existing international guidelines and scientific articles not directly related to Vietnam were reviewed to discuss the global situation and to propose strategic recommendations.
Results
The literature search on Pubmed provided 169 references using the keywords “hepatitis B” and “Viet Nam” and 80 references using the keywords “hepatitis C” and “Vietnam.” Selecting articles with reference to only epidemiology in Vietnam and written in English, the end result of the literature search was only 15 articles that underwent complete text review. This process adds 4 articles not indexed in Pubmed.
Overview—Hepatitis B and C and HIV Coinfection in Vietnam
Hepatitis B
Tables 1 and 2 summarize the prevalence of hepatitis B surface antigen (HBsAg) and hepatitis B core antibody (anti-HBc) in the general population and key affected populations. Our review found that the reported HBsAg prevalence in general population ranged from 5.7% to 24.7% in Vietnam, with most reporting the prevalence from 10% to 20%. 7,9,10,11,13,17,22 The value was much higher for the indicators of past infection: the anti-HBs ranged from 16% to 40% and anti-HBc from 50% to 75%. 22,10,13 There are an estimated 8.4 million people living with chronic hepatitis B in Vietnam. 22
Prevalence of Viral Hepatitis B and C Infection among General Populations
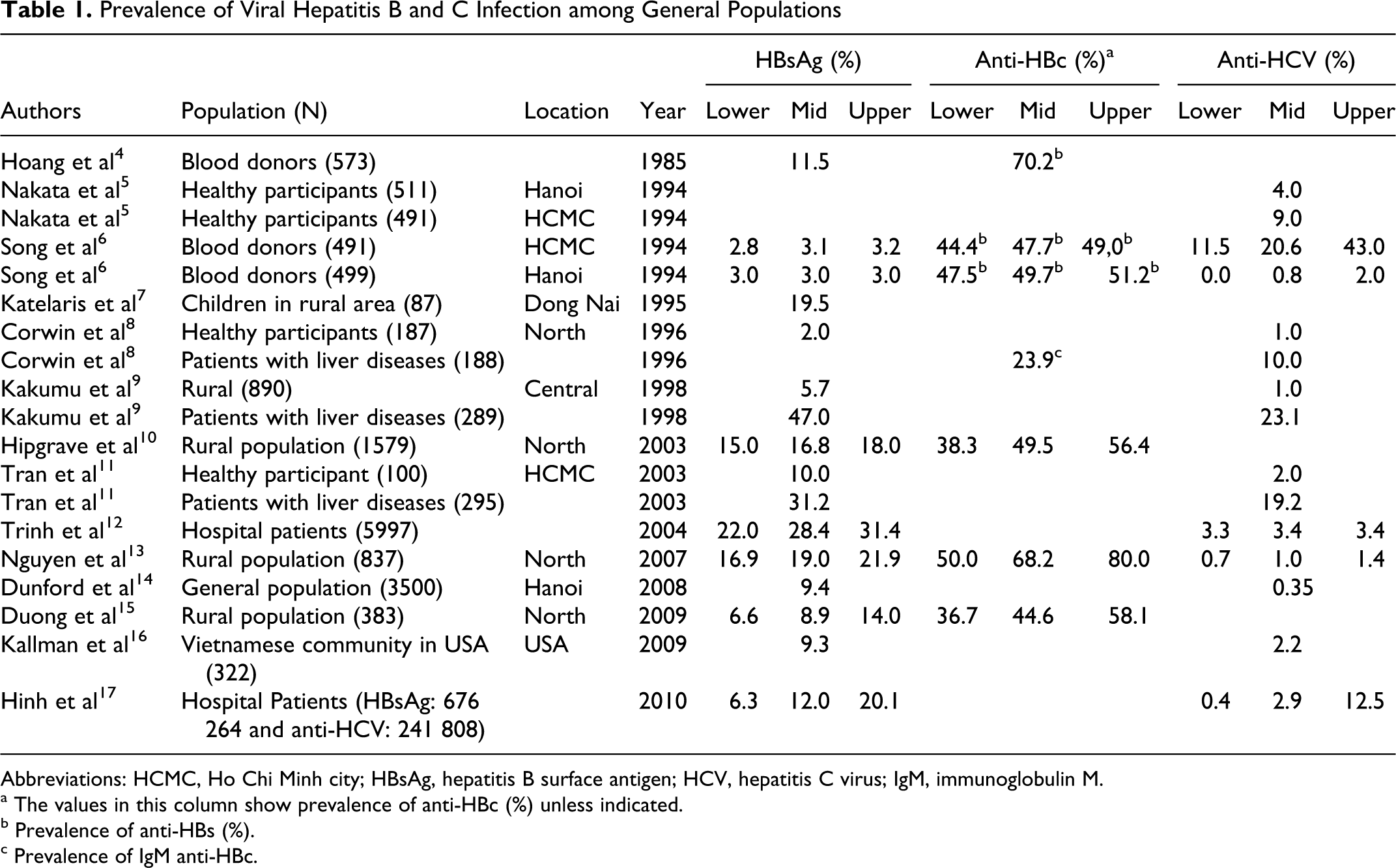
Abbreviations: HCMC, Ho Chi Minh city; HBsAg, hepatitis B surface antigen; HCV, hepatitis C virus; IgM, immunoglobulin M.
a The values in this column show prevalence of anti-HBc (%) unless indicated.
bPrevalence of anti-HBs (%).
cPrevalence of IgM anti-HBc.
Prevalence of Viral Hepatitis B and C Infection among Key Affected Population

Abbreviations: HAARP, HIV/AIDS Asia Regional Program, HCMC, Ho Chi Minh city, PWIDs, people who inject drugs, SW, sex workers; HBsAg, hepatitis B surface antigen; HCV, hepatitis C virus.
The HBsAg prevalence among the subpopulations was also reported by various studies in Vietnam. The HBsAg prevalence ranged from 8.1% to 17.6% among health care workers and was also high among blood donors, people with liver diseases, people who inject drugs (PWIDs) and female sex workers ([FSWs]; Tables 1 and 2) 22,9,11,23,6,18,14
The available data suggest that hepatitis B virus (HBV) is a major cause of liver disease and liver cancer in Vietnam. Between 30.1% and 87.6% of liver cirrhosis cases and 34.8% and 80% of hepatocellular carcinoma can be attributed to HBV infection. 10,11,17,22
The vertical and perinatal transmissions are likely the major mode of transmission of hepatitis B in Vietnam. This is suggested by the high HBsAg prevalence in children 7,17,22 and similar prevalence among people of Vietnamese origin living in other countries (Table 1). 16,24 –26 However, an age-dependent increase in the HBsAg prevalence has also been reported, suggesting the additional role of the horizontal transmission. 17,22
Hepatitis C
Tables 1 and 2 summarize the prevalence of anti-hepatitis C virus (HCV) in the general population and in key affected populations. In Vietnam, the HCV is concentrated among certain population subgroups, mainly PWIDs and patients with liver disease. Some studies found that the anti-HCV prevalence in the general population ranges from 0.38% to 1.7% 5,6,8,27 in the Northern provinces of Vietnam and 1.0% to 4.3% in the Southern provinces. 5,6,9,10,27 The studies also suggested urban populations tend to have higher prevalence compared with the rural population (Table 1). 27 The most affected are men, between the ages of 15 and 59 years, living in urban areas. 17
Among the subpopulations, the highest prevalence was among PWIDs (Table 2). Among blood donors, patients with liver diseases, 5,6,8,9,11,27 and hospitalized nonliver disease patients, the prevalence was higher from the general population (Tables 1 and 2). 5,6,8,9,11,27
The most important risk factor was injecting drugs, as it relates to the transmission through sharing of needles and syringes. 17
In addition, repeated blood donation 6 and history of surgery, acupuncture, medical injections, and dental treatment were also reported risk factors for HCV infection in Vietnam. 18 People who had more than one hospital admission are estimated to be 7.2 times more likely to be infected with HCV than those who had never been hospitalized. 27 These data suggest that the unsafe health care practices, especially unsafe injections, have not been uncommon in the past in Vietnam. 6,18,28 –30 Blood transfusion was also an important risk factor for HCV infection in the past. Nevertheless, it is considered that transmission through blood transfusion was virtually eliminated when the country started the implementation of routine screening of donated blood. 31,32 In 2009, 100% of the blood units were screened for HIV, HBV, and HCV and more than 80% of them came from volunteer blood donors. 33,34
The hepatitis C virus is genetically divided into 6 major groups, many of which contain distinct subtypes. Each genotype has a particular geographical distribution, clinical evolution, and responses to treatment. The most common genotypes in Vietnam were genotypes 1 and 6, about 40% each, followed by genotypes 2 and 3, ranging from 5% to 17%. 11,35 –40
HIV and viral hepatitis coinfection
As a consequence of shared transmission route, coinfection of HIV and hepatitis B and C is common. One study reported HBV prevalence among people living with HIV/AIDS (PLWHA) as not much different from that in the general population (10.3% versus 12.5%). 23 On the other hand, similar studies showed the prevalence of PLWHA ranging from 24.7% to 39.7%. 10,22 Even though HBV and HIV share the many transmission modes, the principal mechanism of transmission seems different between HBV and HIV; that is, HBV infection occurs much earlier especially through vertical transmission, while HIV infection occurs through sharing of injecting equipment and unprotected sexual contact. 23
Both HIV and HCV infections and their coinfection are “concentrated” in the key affected populations, and PWIDs are the most affected. Anti-HCV prevalence among HIV-infected PWIDs can be as high as 98.5%. 18 HIV-HCV coinfection are known to be more likely due to the development of rapid fibrosis compared patients with HCV monoinfection, and with cirrhosis is associated with enhanced progression and mortality. A suppressed immune system lacks activity against HCV replication and leads to a higher viremia.
In addition, highly active antiretroviral therapy (HAART)-related hepatotoxicity, drug and heavy alcohol use, and other underlying patient conditions can aggravate liver disease. There is currently no evidence that HCV/HIV or HBV/HIV coinfections lead to faster progression of HIV infection.
Burden of Viral Hepatitis and Liver Diseases
Chronic HBV infection is the leading cause of liver disease and hepatocellular carcinoma in the general population in Vietnam. Chronic HCV infection also has a critical role in the pathogenesis of liver disease and hepatocellular carcinoma in the key affected populations.
As nonnotifiable diseases, data on the burden of HBV- and HCV-related liver diseases are very limited; however, some facility-based studies have found that 47.8% to 87.6% liver cirrhosis cases can be attributable to HBV infection, while 10% to 26.7% can be attributable to HCV infection. Moreover, 34.8% to 80% of patients with liver cancer can be attributable to HBV. 8,9,11,17,27,41 For the association between HCV and liver cancer, there are very limited data and only 1 study has reported that 14% of liver cancer was due to HCV infection. 17
Mathematical models estimate nationally that by 2013, the number of people with chronic HBV infection will reach its peak at 8.6 million cases and then decrease to 8 million by 2025, as a direct impact of the universal infant vaccination. 42 However, the prevention of new infections does not affect the progression of the already infected individuals, and thus the estimates suggest liver cancer and liver cirrhosis cases will continue to increase: liver cirrhosis will increase from 36 500 cases in 2005 to 58 600 in 2025 and liver cancer will increase from 15 600 in 2005 to 25 000 in 2025. 42 As a result, the estimated annual HBV-related deaths will increase from 23 300 in 2005 to 40 000 in 2025. 42
Ngo et al have found that liver cancer and liver diseases were the fourth and sixth causes of deaths among males, respectively, and that liver cancer was the third cause of death among females, between 15 and 59 years of age. 43 Nevertheless, among cancer-related deaths, liver cancer was ranked as the leading cause, with 31.0% among males and 19.9% among females, followed by lung and stomach cancers. 44
The Burden of Disease study in Vietnam in 2008 estimated that liver cancer was the second leading cause of death in men, while it was the sixth cause in women. Liver cancer was also the third and fourth cause of years of life lost in men and women, respectively, in 2008 in Vietnam. Among the cancer types, liver cancer was estimated as the largest cause of disability adjusted life year in both sexes. 45
With an estimation of more than 8 million individuals infected with HBV or HCV in Vietnam, viral hepatitis represents an important burden on the health and economic sectors. 42 In addition, since progression to liver diseases and liver cancer takes many years, an even greater burden is to be expected in coming decades.
Situation in the Key Affected Populations
People who inject drugs
Officially registered there were 180 000 PWIDs in Vietnam. The most commonly used drug is heroin (81.9%), and the main use pattern is injecting (62.2%) followed by inhaling (27.3%). 46 In Ho Chi Minh city (HCMC), 37% of the PWIDs reported sharing needles and syringes. 47
The prevalence of blood-borne viruses was higher in PWIDs than in the general population, with prevalence of HIV among PWIDs at 18.4% to 29.5%, according to the national sentinel surveillance, 33,47 while other studies found the prevalence to be ranging from 17.5% to 72%. 18,47 –50
Despite the shared modes of transmission of HIV, HBV, and HCV, the data show HBV prevalence among PWIDs similar to that in the general population. 18,21,22,23 This finding suggests that HBV infection most likely occurs in the early infant period. In contrast, the HCV infection was highly associated with the drug injecting behavior. 5,17,18,21,27 The higher prevalence of HCV than HIV in PWIDs suggests that HCV is more efficient than HIV in blood-borne transmission.
Those scenarios suggest that both HCV/HIV and HBV/HIV coinfections will be common among PWIDs. This is supported by study findings, among the participants in administrative detention centers for PWIDs, 20 as well as by a community-based survey in Bac Ninh province in the northern Vietnam, 18 which showed very high prevalence of viral hepatitis among PWIDs (Table 2).
Efforts of the government of Vietnam to contain the spread of HIV among PWIDs include needle and syringe programs, condom distribution, opioid substitution therapy with methadone, and expansion of antiretroviral (ARV) treatment. However, these programs do not mention viral hepatitis prevention and control, and moreover, the impact of these programs on HCV prevention is inconclusive. 18 The lack of educational activities targeting PWIDs concerning viral hepatitis and the lack of routine testing for HCV and HBV in PWIDs are challenges to control HCV and HBV epidemics in this group.
Female sex workers
Along with PWIDs, FSWs are a major risk population in the HIV epidemic in Vietnam. 33 Surveillance has found a national HIV prevalence ranging from 3.2% to 10% among FSW, with street-based FSW showing higher prevalence than karaoke-based FSW in the past years. 47,51,52 In Hanoi, the prevalence ranged from 6% to 23%, while in HCMC it ranged from 8% to 10%. 47,48,51,52
Concerning the HBV and HCV prevalence, studies have shown similar rates of HBsAg to the general population (Table 2). 14,23 There were no studies on the HCV prevalence among FSW in the bibliographic review.
In addition, 17% to 32% 47,53 of FSW in Hanoi reported injecting drug use, 64% of them shared needles and syringes. 53 Since condom use in the most recent sexual intercourse was reported to be more than 90% (59.3%-97.8%), needle sharing remains a major mode of transmission of HIV among FSW and very likely that of HCV.
Men having sex with men
In Vietnam, the HIV prevention program targeting men having sex with men (MSM) is still of limited scale, although the government is intensifying its intervention efforts to this group due to the recent rapid rise in the HIV prevalence among MSM in urban centers and identification of MSM networks with HIV beyond the major urban centers.
The HIV prevalence in MSM was 5.3% to 8% in HCMC and 9% in Hanoi according to the studies conducted before 2008. 47,54,55 However, more recent surveillance shows that HIV prevalence is rapidly rising in this population. According to the integrated biological and behavioral surveillance, HIV prevalence in MSM increased from 5.3% in 2006 to 16.7% in 2009 in HCMC and from 9.4% in 2006 to 17.4% in 2009 in Hanoi. 56
The MSM also seem to have overlapping risk factors. The Integrated Biological and Behavioral Surveillance in 2006 reported that 22% of MSM in Hanoi and 4% in HCMC reporting selling sex in the past year. 47 Use of injecting drugs was reported by 9% of MSM in Hanoi versus 4% to 6% in HCMC, and among them 26% were HIV infected. 47,55 Among MSM in HCMC, the most associated risk factor was use of injecting drugs (odds ratio [OR] = 30.3) followed by selling sex (OR = 6.12). 55
No study on HBV or HCV infection among MSM was found in our bibliographic review. However, because of overlapping risk factors and reported low level of consistent condom use in this group, it is possible that HCV and HBV prevalence among MSM is likely to be high.
It is common among MSM to have sex with both men and women, which is reported by 30% of MSM in HCMC. Therefore, the female sexual partners of MSM are also with increased risk of transmission. 55
Discussion
Current Response and the Suggested Way Forward
Surveillance of Hepatitis B and C
In Vietnam, there is neither case reporting nor a surveillance system for hepatitis B and C. It is recommended that the health information management system should include hepatitis cases and the number of those who received treatment. Inclusion of HBV and HCV testing in the HIV sentinel surveillance system should also be considered.
Prevention of Hepatitis B and C
Routine immunization of hepatitis B for all infants has been promoted. Further scale-up of HBV immunization should be considered to achieve the universal coverage. Harm reduction and HIV prevention interventions targeting key affected populations, including the needle–syringe programs, opioid substitution therapy, and condom promotion, have been rapidly scaled up in Vietnam over the past decade as part of the national HIV response. These interventions are also anticipated to be effective for the prevention of transmission of other blood-borne viruses including HBV and HCV. However, to date, there have been few educational and prevention activities to raise awareness and promote knowledge on viral hepatitis in Vietnam targeting key affected populations. One of the few initiatives belongs to Vietnam Network of People Living with HIV/AIDS, a nongovernmental organization (NGO) comprising PLWHA. It is recommended that interventions should be widely expanded to educate the affected populations on prevention, diagnosis, and treatment of hepatitis B and C along with those having HIV.
Identification of people with HBV and HCV infection is also an important prevention measure, as it enables them to adopt behaviors that reduce the risk of transmission to others.
Diagnosis of Hepatitis B and C
The diagnoses for both HCV and HBV infections are based on serological and molecular assays. However, at present, there is no national standard algorithm to diagnose HBV and particularly HCV infection in Vietnam, and thus different assays and techniques are used for the diagnosis. It is recommended that a national testing algorithm be developed urgently to support scale-up of screening and confirmation of HBV and HCV infection and related diseases. The National Institute of Hygiene and Epidemiology in Hanoi has recently conducted evaluation of HIV assays to develop the National algorithm for HIV testing. Viral load testing using polymerase chain reaction (PCR) techniques is becoming progressively accessible and affordable in Vietnam to diagnose treatment failure of antiretroviral therapy for PLWHA. The Ministry of Health may consider the use of such experiences and available infrastructure within HIV programs and other health sector resources to accelerate the diagnostic algorithm development and scale-up of the HBV/HCV screening and diagnostic services. 57
The following recommendations are based on the international guidelines and take into account the resource availability and current situation of the viral hepatitis epidemic in Vietnam.
Hepatitis B
The most commonly used assay for HBV screening is HBsAg. 58,59 However, for diagnosis and clinical management of HBV diseases, other markers, such as hepatitis B e antigen (HBeAg), anti-HBc immunoglobulin M (IgM), total anti-HBc, hepatitis B e antibody (anti-HBe), and anti-HBs, are needed. Those markers help identify 3 phases of HBV infection: the immune tolerant phase, the immune active phase, and the inactive phase. 57,60 –63 The HBV treatment is indicated only for patients in the immune active phase 57,64,65 and a molecular assay is used to assess the presence and concentration of circulating HBV DNA in this phase. 60
The mass screening for HBsAg requires massive resources, and on public health grounds, certain groups of persons should be prioritized. 60,64 –67 National policy should preferentially offer HBV screening to those recommended in Box 1.
Proposed persons who should be prioritized for HBV screening in Vietnam

Hepatitis C
Serological tests for detecting antibodies to HCV only identify previous exposure and are commonly used as screening tests. Serological tests are performed using enzyme immunoassay test or rapid test. However, to confirm current active disease, HCV RNA PCR assay is used for direct evidence of the presence of virus in the blood. The HCV RNA PCR is also performed to measure the viral load needed to monitor treatment response.
Mass screening for hepatitis C has not yet been recommended in Vietnam as the HCV epidemic is concentrated to certain subpopulations. However, national policy should be developed to preferentially offer HCV screening to those who are at elevated risk of HCV infection as recommended in Box 2. 64,65,68 –71
Proposed persons who should be prioritized for HCV screening in Vietnam

Assessment of liver fibrosis
The gold standard method to assess the liver necroinflammatory activity is histological examination through liver biopsy. The most commonly used score for biopsy is the METAVIR fibrosis score, and treatment is indicated with a grade of at least F2. 64,67,68,72 –74 However, liver biopsy is not commonly performed in Vietnam. Instead noninvasive methods, that is, serological markers and ultrasound-based methods are used to assess liver fibrosis.
Globally, various scores that combine serological markers and attempt to predict the level of liver fibrosis have been developed and tested. 74 –83 One of the most investigated scales is the Hepascore using a combination of commonly available laboratory markers. It reportedly has a general specificity of approximately 80% for identifying both significant and advanced fibrosis. 76,79,80
The elastography, an ultrasound-based method is already being used in some hospitals in Vietnam. The transient elastography, also known as FibroScan, uses the speed of propagation of waves created by the transducer to estimate the stiffness of the liver tissue. Despite being operator dependant and the need for special training and ultrasound equipment, elastography is a rapid and noninvasive method of estimation of severity of cirrhosis. Confirmed by several studies, FibroScan is an efficient and simple method for evaluating liver fibrosis in patients with chronic infection of both HBV and HCV. 77,78,84 Based on global evidence, it is recommended that Vietnam Ministry of Health develop and field test a standard diagnostic algorithm for advanced viral liver disease, combining a set of serological markers (eg, with a Hepascore type assay) and molecular assays (PCR viral load tests) to identify those who require HBV and HCV treatment and to monitor treatment effectiveness. Availability of the quality-assured elastography should also be expanded at referral hospitals.
Treatment of Hepatitis B and C
At present, neither HBV nor HCV treatment is subsidized by the government or supported by the national health insurance scheme. Thus, the treatment has been accessible only to those who can afford to pay the full cost. There is no available data on how many people have received treatment of HBV or HCV disease in recent years in Vietnam. However, considering the high cost of HBV and HCV treatment, it is likely only a few patients have received definitive treatment.
HAART for PLWHA has been rapidly scaled up since 2005 with 49 492 people receiving ARV medications at the end of 2010, in Vietnam, mostly with international donor support. Lamivudine (3TC) has always been used for first-line HAART in Vietnam, and tenofovir (TDF) is becoming more and more available.
There is currently no national guideline on HBV and HCV treatment in Vietnam. Without access to such treatment, Vietnam will bear an increasing burden of liver disease, liver cancer, and associated death. It is therefore recommended that national guidelines for treating HBV and HCV diseases be developed. To support the national efforts, the international evidence and standards related to HBV and HCV treatment is summarized below.
This article is also a call for political commitment, national leadership, international resource mobilization, and further regulatory and research efforts to make the treatment of HCV disease available and affordable in Vietnam and other resource-limited settings. The current treatment options are not affordable for most Vietnamese patients without financial support. In HIV treatment, all the research, development, advocacy, and negotiation efforts have dramatically lowered the price for HAART. We do hope that similar solidarity will find the solution for HCV treatment.
Hepatitis B
Serological, biochemical, and molecular markers are used to identify the HBV-infected persons who have active liver inflammation. Treating these immune active patients will prevent them from developing liver cirrhosis and liver cancer, thus reducing future mortality and morbidity. 57 For clinical follow-up, short-term goals are HBeAg seroconversion to Anti-HBe, HBV DNA suppression, Alanine transaminase (ALT) normalization, and HBsAg seroconversion to Anti-HBs. 64,65,67,73
Treatment is indicated if serum ALT is persistently elevated higher than 2 times of the upper limit of the normal range and if HBV DNA is higher than 20 000 UI/mL for HBeAg-positive patients or higher than 2000 UI/mL for HBeAg-negative patients.
The most commonly used drugs for HBV treatment include conventional interferon, pegylated interferon, adefovir, TDF, 3TC, emitricitabine, and entecavir. The therapy duration is 6 months for conventional interferon and 6 to 12 months for pegylated interferon. For oral antiviral drugs, the treatment can be stopped when HBeAg seroconversion and HBV-DNA suppression are sustained for at least 6 months. For HBeAg-negative patients, the HBV-DNA should be suppressed for 12 months. 73
The effectiveness of interferon-based treatment is modest with a HBeAg loss rate at 33%; however, when it is achieved, it is sustained in more than 80% during the long-term follow-up. 73 In addition, interferon-based treatment is associated with adverse effects, due to which some patients cannot tolerate standard treatment and require dose modification or a complete cessation of treatment prematurely. 73
The oral antiviral drugs are better tolerated and have a better response rate but require a longer treatment course. The HBeAg seroconversion rate using 3TC ranges from 35% to 65% after 5 years of therapy. 65,73 The emergence of drug resistance during long-term therapy is also not uncommon. In 5 years of treatment, it was reported that up to 70% of patients acquired a 3TC -resistance strain of HBV. 74
Hepatitis B/HIV coinfection
Indication for treatment for HBV disease is the same for HIV/HBV coinfected patients as the HBV monoinfected patients. The World Health Organization (WHO) now recommends initiating HAART regardless of CD4 count if PLWHA require treatment for HBV disease. For those patients, ARV drugs that are active against HBV, that is, tenoforvir and 3TC or emitricitabine, should be included as the standard of care. 64,65,67,73,85 –88 It is also important to avoid ARV drugs that are potentially hepatotoxic, such as nevirapine (NVP).
Hepatitis C
The standard treatment course currently recommended for chronic hepatitis C is the combination of pegylated interferon and ribavirin, for which a study reported an efficacy of 56% in achieving the sustained viral suppression. 72 Two options of pegylated interferon are available: pegylated interferon α-2a and pegylated interferon α-2b, which have similar rates of success.
Patients diagnosed with chronic hepatitis C infection and who have detectable HCV RNA, elevated ALT, and evidence of significant liver necroinflammatory activity are indicated for treatment. 53,68,71 The treatment is based on the HCV genotype. Patients with HCV genotypes 1, 4, and 6 should receive 48 weeks of treatment, while genotypes 2 and 3 should receive 24 weeks of treatment. 72,89
The goal of HCV treatment is to achieve a sustained virological response (SVR) which is confirmed with HCV RNA PCR being undetectable at 6 months after treatment completion. During the treatment, the effectiveness is assessed using the following categories to predict a successful SVR. 72,89
rapid virological response, undetectable HCV RNA after 4 weeks of treatment;
complete early virological response, undetectable HCV RNA after 12 weeks of therapy;
partial early virological response, HCV RNA decreases at least 2 logs from the baseline after 12 weeks of therapy.
Hepatitis C/HIV coinfection
If HCV treatment is indicated but the CD4 count is above the general threshold to initiate HAART, it is preferable to initiate the HCV treatment before HAART initiation. In contrast, if the patient is eligible for HAART using the general criteria, HAART should be initiated first and then HCV treatment should be initiated after the stabilization of the immune system to ensure treatment efficacy and to minimize the adverse events. 60,89,90
Conclusion
We compiled the available study findings and information related to viral hepatitis epidemic and response in Vietnam. Our review indicates that Vietnam bears substantial burden associated with chronic hepatitis B and C infection. The burden of the viral hepatitis may be impacting PLWHA.
The authors advocate that more attention should be paid and investment made to strengthen prevention, diagnosis, care, and treatment of viral hepatitis. Further expansion of immunization against HBV including the birth dose, assurance of safe health care practices, and harm reduction services for PWIDs are priority prevention interventions for Vietnam.
Developing policies for diagnosis and treatment of chronic HBV and HCV infections are also critical priorities in order to prevent progression to cirrhosis and liver cancer and to minimize related morbidity and mortality. To optimize the response in Vietnam and other resource-limited settings, further operational research is needed to strengthen the evidence base. Mobilization of resources from domestic and international funding sources is needed, and mechanisms to promote price reduction of treatment (such as UNITAID which played a critical role in reducing the price of ARV drugs) are essential. Further programs on viral hepatitis should be synergized to the already ongoing efforts on HIV for better results.
The viral hepatitis resolution of the 63rd World Health Assembly requested the Director General of WHO to collaborate with all the stakeholders in supporting national responses to viral hepatitis, especially in low- and middle-income countries. 1 This article is a call for concerted efforts of national health authorities, international donors, technical agencies, and community partners to jointly intensify our combat against the silent epidemic of viral hepatitis and to dramatically reduce the associated liver disease burden in Vietnam and in the world.
Footnotes
Acknowledgments
We would like to express our sincere appreciation for all the persons who shared their literature, data, and other information on HBV and HCV in Vietnam and to those who took their time to speak with us through the interviews. We received generous support from both public and private sectors, including the Vietnam Authority for HIV/AIDS Prevention and Control, the national institutes and national hospitals affiliated with Vietnam Ministry of Health, the Vietnam Network of people living with HIV, the US Center for Diseases Control in Vietnam, and some of the Vietnamese’s pharmaceutical companies. We are also very grateful to Dr Keith Sabin for his expert inputs on HIV and hepatitis epidemiology in Vietnam and to Ms Pamela Kechter who provided us with assistance in the literature management and proofreading the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by regular WHO budget.