
Abstract
Gay, bisexual, and other men who have sex with men (GBMSM) are associated with the widespread human immunodeficiency virus (HIV) transmission in Taiwan. Additionally, little is known about disclosure patterns and rates, as well as factors influencing disclosure, among GBMSM living with HIV in the country. HIV prevention for GBMSM is effective when HIV status is disclosed. For instance, GBMSM disclosing their HIV status can result in early pre-exposure prophylaxis with a serodiscordant partner. In this cross-sectional study of 200 GBMSM living with HIV conducted from June to November 2020, we assessed internalized homophobia (IHP Scale) and social support (Multidimensional Scale of Perceived Social Support), as well as self-reported disclosure and non-disclosure. Among the participants, 75.5% revealed their HIV status within 3 months of diagnosis. Younger age, occupation type, and number of sexual partners were some factors associated with disclosure. Those receiving more social support and who experienced less IHP were more likely to reveal their HIV status. On the contrary, older GBMSM and GBMSM living with HIV who worked in educational enterprises still experienced severe IHP. Policymakers and healthcare practitioners should be aware of the problems faced by GBMSM living with HIV and offer practical assistance to improve their mental health.
Keywords
Background
By the end of 2021, it was estimated that, globally, there were 38.4 million people living with human immunodeficiency virus (HIV). 1 In Taiwan, the current population of people living with
HIV is 43 328, with a growth rate of 190 times from 1984 to 2021. Gay, bisexual, and other men who have sex with men (GBMSM) are associated with the widespread HIV transmission in Taiwan. As of December 2022, the majority of individuals (81.9%) who contracted HIV did so through sexual contact, with GBMSM accounting for 66.8% of this subset. 2
The act of revealing one’s HIV status to sexual partners has been deemed a crucial component of HIV prevention. 3 In the case of an individual living with HIV who is on virally suppressive antiretroviral therapy (ART), condom use is no longer the most effective measure for preventing the spread of the virus. Given the endorsement of Undetectable = Untransmittabile information by organizations like the World Health Organization (WHO)—that is, maintaining low enough viral loads to be unable to transmit the virus to others—it is more critical than ever for GBMSM living with HIV to inform their seronegative companions of their status to ensure timely pre-exposure prophylaxis.4,5 Despite this, HIV disclosure has been linked to discrimination, isolation, and intimidation. 6 To promote HIV disclosure and support those living with HIV in Taiwan, it is beneficial to explore the experiences of individuals who disclose their HIV status and the factors that either facilitate or impede such disclosure.
In 2013, the Taiwan Centers for Disease Control raised the CD4 count threshold for initiating ART from 350 to 500 cells/µL. Taiwan adopted the WHO-recommended treat-all policy in 2016, and the pre-exposure prophylaxis program was officially launched in September 2018. 7 However, an unexpected HIV diagnosis was revealed in 2017, 8 highlighting the importance of HIV-positive status disclosure to improve ART adherence and HIV prevention. 9 While GBMSM with suppressed viral loads are more likely to disclose their HIV-positive status,10,11 the proportion of men living with HIV who disclose their serostatus remains relatively low. In a Taiwanese study, only 36% of GBMSM disclosed their HIV serostatus to family members and/or friends. 12 The proportion of GBMSM who have disclosed their HIV status and the characteristics of those receiving ART in the treat-all era have not been adequately studied in Taiwan.
HIV disclosure is recognized as a complicated process, 13 one in which the social and cultural environment have a significant influence. 14 Recent research indicates that personal characteristics (age, disease severity), interpersonal factors (partner role type, relationship duration), and sociocultural factors (social support and cultural heritage) influence whether GBMSM living with HIV disclose their status.13,15,16 Studies describe various aspects of stigma related to HIV. Internalized stigma, which refers to a negative self-image, as well as disclosure worries, enacted stigma, anticipated stigma, and perceived stigma in the community, all influence stigmatization.17,18 Additionally, Asian GBMSM frequently face “dual pressure” when reporting their sexual orientation and HIV status owing to the strong societal emphasis on avoiding “shame.” 19 As a homosexual, being equated with feminine may result in internalized homophobia (IHP), also known as self-stigma, which is linked to psychological distress, sex trafficking, sexual coercion, and concealment of sexual identity.20,21 Compared with other MSM, men who reported higher levels of bisexual and internalized stigma found it more challenging to disclose having sex with men to their primary female partner. This difficulty in disclosure has a notable connection with reduced engagement in HIV prevention interventions, which is significantly correlated with reduced HIV prevention interventions. 22
Although it was the first Asian nation to legalize same-sex marriage in 2019, Taiwan still faces HIV-related stigma. Yu et al 23 observed stigmatization prior to and subsequent to HIV status disclosure in Taiwan. Before the disclosure, difficulties included fear of unemployment/isolation, while post-disclosure issues included the particular considerations and requirements of educational institutions or workplaces and difficulties in seeking medical care and stress relief. Consequently, HIV disclosure among GBMSM remains a public health concern.
People living with HIV frequently choose to disclose their HIV status to significant others (such as parents, close friends, partners, and siblings) who offer security and support. 24 Such disclosure has been shown to lead to improved self-esteem, higher levels of emotional support, and a reduction in depression and anxiety. 25 Social support for medication adherence is one tangible benefit of disclosure to significant others.26,27 Although same-sex marriage legalization has been beneficial in this regard, 28 identifying the factors that enable or hinder disclosure is vital in improving the mental health of GBMSM.
We aim to investigate the disclosure patterns and rates among GBMSM living with HIV and receiving ART in Taiwan. By examining factors such as sexual behaviors, IHP, and social support, as well as predictors of disclosing HIV status to particular individuals, we seek to fill the gap in the existing literature.
Methods
Design and setting
A cross-sectional design was implemented to examine disclosure concerns and associated factors among GBMSM living with HIV and receiving ART within the outpatient department of Mackay Memorial Hospital. The study was conducted from June to November 2020. We included GBMSM who were at least 20 years old, had been diagnosed with HIV, could communicate in Chinese or Taiwanese, and consented to participate. Excluded were individuals with acute infectious diseases, physical or mental disabilities, and a psychiatrist’s diagnosis of schizophrenia, bipolar affective disorder, or substance dependence.
Sample size calculation and sampling procedure
The sample size was calculated using binary logistic regression with a significance (α) of .05 and a test power of .8 using the statistical software G*Power 3.1.2. Based on previous findings, the likelihood odds ratio (OR) was set at 1.5. To reduce errors resulting from invalid questionnaires and missing data, we increased the sample size by 20% and the final sample size was approximately 200.
Data collection tools and procedure
A standardized data collection instrument was created after reviewing the relevant literature.13,15,16 We collected information on basic demographic characteristics, sexual behavior- and disease-related factors, IHP, and social support level.
First, in the outpatient clinic, participants who met the inclusion criteria were referred to the primary researcher. Prior to completing the study, participants were briefed on its purpose. The primary researcher also apprised them of their rights and the potential benefits and risks of participation. In addition, participants were informed that relevant data would be presented anonymously, the questionnaires would be coded, and the data would be stored securely and with utmost confidentiality. The researcher collected data using one-on-one and face-to-face methods. It took 10 to 15 minutes to complete the questionnaire.
Dependent variables
HIV disclosure status
HIV disclosure is defined as the disclosure of HIV status to someone other than a healthcare provider. HIV disclosure status is dichotomized as yes/no.
Patterns of disclosure
The study examined patterns of disclosure, categorizing them into 2 parts: before and after “early access to treatment for all.” Specifically, patterns of disclosure were categorized as the first person disclosed to (sexual partner, parents, close friends, and siblings) 24 and the timing and motivation of disclosure.
Independent variables
Patient-level factors
Sociodemographic variables
Sociodemographic variables include age (years), educational level, and occupation type.
Sexual behavior-related factors
Sexual behavior-related factors include current relationship status, time spent with the last partner, sexual orientation (same-sex or bisexual), number of sexual partners in the past 6 months, sexual behavior in the past 6 months, and serostatus of the sexual partner in the past 3 months.
Disease-related factors
Disease-related factors include the number of years since HIV diagnosis, 2 categories of “early access to ART for all” (2016 is a watershed moment), duration of receiving antiviral drugs, CD4 count in the past 6 months, and viral load in the past 6 months. The past 6 months’ laboratory values for plasma CD4 count and viral load were obtained from the patients’ charts.
Independent variables
Psychosocial factors
Perspectives on sexual orientation identity
Using the IHP Scale, we determined that the Cronbach’s alpha rating of internal reliability for the pretest of the Chinese version was .84. The instrument contains 9 items scored on a 5-point Likert scale, all of which are positively worded. Example items are “I have tried to stop being attracted to men in general,” “If someone offered me the chance to be completely heterosexual, I would accept it,” “I wish I weren’t gay/bisexual,” “I feel that being gay/bisexual is a personal shortcoming for me,” and “I would like to get professional help to change my sexual orientation from gay/bisexual to straight.” The scores of the 9 items are summed, and the total score ranges from 9 to 45 points. A higher score indicates a higher tendency toward IHP. This measurement is based on participants’ self-reported perspectives on sexual orientation identity and homophobia.
Social support
The Multidimensional Scale of Perceived Social Support (MSPSS), which was translated to Chinese in 2008, 29 has a Cronbach’s alpha value of .88. This instrument is used to measure the level of social support among individuals with HIV across 3 dimensions: family (items 3, 4, 8, and 11), friends (items 6, 7, 9, and 12), and significant others (items 1, 2, 5, and 10). The 12 items are scored on a 7-point Likert scale, where 1 denotes “very strongly disagree,” and 7 denotes “very strongly agree.” All items are positively worded, and the total score ranges from 12 to 84 points. A higher score indicates a higher level of social support.
Data analysis
First, descriptive statistics were used to analyze participant characteristics. Nexty, the independent samples t-test and chi-square test were performed to examine sociodemographic characteristics, sexual behavior-related factors, and disease-related factors. Pearson’s product-difference correlation analysis was conducted to examine the association between IHP and social support. A binary logistic regression analysis was then performed to determine the relationships between the basic demographic characteristics, sexual behavior-related factors, disease-related factors, IHP, social support, and disclosure. The explanatory power of the disclosure of HIV status was measured. All statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA).
Ethical considerations
This study was evaluated and approved by the Institutional Review Board of Mackay Memorial Hospital (20MMHISO17e) in June 2020. All participants provided written informed consent.
Results
Participants’ characteristics
The data of all 200 GBMSM living with HIV were included in the analysis (recovery rate: 100%). The participants’ average age was 34.3 (standard deviation [SD] = 7.2) years (Table 1). The year of HIV diagnosis ranged from 2004 to 2020. The majority of the participants (60.5%) held a bachelor’s degree or higher. The majority (90%) were employed in the service (30.0%) or technology (28.0%) industries. The average relationship duration was 37.4 months, and 86.5% of the participants were homosexual. In the previous 6 months, 47% of the participants had had a regular sexual partner. Most participants (47%) had condom-protected anal contact within the last 3 months, and 58% were unaware of their sexual partners’ serostatus. The mean ART duration was 5.1 (SD = 3.9) years. The average number of years since diagnosis was 6.2 (SD = 4.6). The average CD4 count per 6 months was 591.1 (SD = 268.6), and 95.5% of the participants had viral loads of less than200 copies per mL.
Differences in the demographic and disease characteristics between the disclosure and non-disclosure groups (N = 200).

Patterns of HIV-positive status disclosure
Figure 1 shows that 75.5% of all participants disclosed their infection status to others.
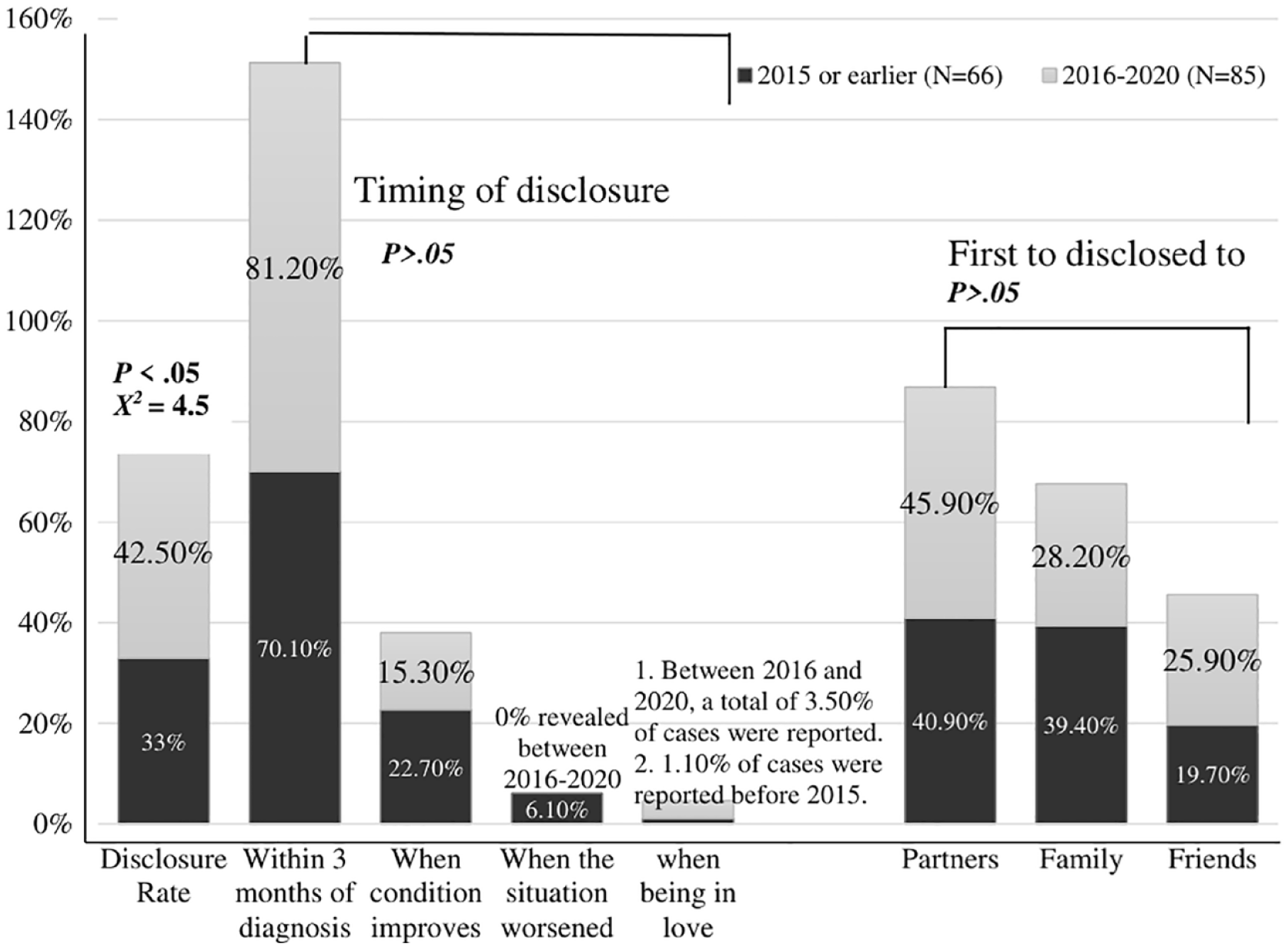
Comparison of HIV-positive status disclosure rate and patterns before and after “early access to ART for all.” Patterns of disclosure are categorized as disclosure rate, timing of disclosure, and the first person disclosed to (eg, sexual parents, close friends, and siblings).
Overall, diagnoses in or before 2015 were associated with a lower disclosure rate (33%) compared with the period from 2016 to 2020 (42.5%), which was statistically significant (X2 = 4.55, P < .001). Following the implementation of “early access to treatment for all” between 2016 and 2020, participants most frequently disclosed their status to their partners, accounting for 45.9%. In contrast, before 2015, the participants were most likely to have disclosed their status to family members (39.4%). The majority of the participants disclosed their status within 3 months of diagnosis both before and after “early access to treat for all” (70.1% and 81.2%, respectively). On the other hand, before “early access to treat for all,” only 6.10% of the participants disclosed their status when their condition had worsened. As shown in Figure 2, the most prevalent reasons for disclosure were feelings of responsibility and obligation, the reduction of psychological stress, and, before 2015, the explanation that they could not transmit the infection to anyone. The variations in CD4 counts before and after disclosure of HIV-positive status, which were statistically significant (t = 3.8, P < .001), are displayed in Figure 3.

Comparison of HIV-positive disclosure patterns before and after “early access to ART for all.” Patterns of disclosure are categorized as motivations for disclosure.

Variations in the CD4 counts before and after disclosure of HIV-positive status.
Distinctions in the demographic and disease characteristics between the disclosure and non-disclosure categories
Table 1 compares the demographic and disease characteristics of the disclosure and non-disclosure groups. Age and employment were significantly associated with HIV disclosure. The average age of participants living with HIV was 33.5 (SD = 6.74) years, whereas the average age of HIV-negative participants was 36.6 (SD = 8.23) years. Younger participants were more likely to disclose their HIV status than older individuals (t = 2.65, P < .05). The Chi-square test revealed that HIV status disclosure was not associated with employment status (χ2 = 0.24, P = .62) but with occupation (χ2 = 27.03, P < .001). Disclosure was more prevalent among participants in the occupation categories of engineer in technology industry (31.1%), service industry (32.5%), and technician (17.2%) than in education industry (5.3%). The number of sexual partners in the previous 6 months differed significantly between the disclosure and non-disclosure categories (χ2 = 13.45, P < .005); participants with a single regular sexual partner disclosed more than any other group. Sexual conduct in the past 6 months and knowing the serostatus of their sexual partners in the past 3 months was also associated with HIV status disclosure (χ2 = 11.10, P < .005 and 38.47, P < .001, respectively). Among the 84 participants who knew the HIV status of their companion, 97.6% disclosed their own status. Of the 116 participants who were unaware of their partner’s serostatus over the past 3 months, 59.5% disclosed their own HIV status. HIV status declaration was strongly correlated with years since diagnosis and ART. Those who disclosed their HIV status had an average of 5.8 (SD = 4.2) years since diagnosis, compared with 7.6 (SD = 5.2) years for those who did not. Those with a shorter average time since diagnosis disclosed their HIV status more easily (t = 2.2, P < .05). The duration of ART was also linked with HIV status declaration (t = 2.2, P < .05). The average period of receiving antiviral medicines was shorter for those who disclosed their HIV status (4.7 years; SD = 3.6 years) than for those who did not (6.2 years; SD = 4.3 years). The association of CD4 count in the previous 6 months and viral load in the last 6 months with HIV status declaration was similar. A marginally significant positive correlation between age and IHP was observed (r = .2, P = .2).
Correlations between IHP, social support, and disclosure of HIV status
IHP and disclosure of HIV status
Table 1 shows the participants’ IHP Scale scores. The average score was 18.81 (SD = 7.41), indicating a low level of IHP. The t-test was inconclusive (t = 0.48, P > .05).
Social support and disclosure of HIV status
The participants’ average MSPSS score was 59.14 ± 15.03 (Table 1), indicating a considerable level of social support. The participants had the highest score of 20.89 (SD = 5.84) in the significant others (such as parents, close friends, partners, and siblings) dimension and the lowest score of 17.75 (SD = 6.47) in the family dimension. The score for the friend dimension was 20.50 (SD = 5.61). A significant correlation was noted between social support and the disclosure of HIV status (t = −5.03, P < .001). The 3 dimensions of significant others (t = −4.55, P < .001), family (t = −3.47, P < .05), and friends (t = −3.80, P < .001) were significantly correlated with social support.
IHP and social support
The correlations between IHP and social support and its dimensions were examined using Pearson’s product-difference analysis. IHP was negatively correlated with overall social support (r = −.23, P < .01), indicating that participants with a strong tendency toward IHP had a lower social support score. The correlation between IHP and various dimensions of social support, from high to low, was friends (r = −.23), significant others (r = −.22), and family (r = −.13). All dimensions were negatively correlated with IHP.
Predictors of disclosure or non-disclosure of HIV status
To determine the predictors of HIV status disclosure among MSM, we conducted a logistic regression analysis of variables substantially correlated with HIV status disclosure. Table 2 summarizes the findings. The occupation, sexual behavior in the previous 6 months, knowledge of their sexual partners’ serostatus in the last 3 months, and social support significantly explained whether participants would disclose their HIV status. Participants from the education industry had a lower disclosure rate (B = −3.47, OR = 0.03, P < .001) than those from other industries. On the contrary, engaging in anal intercourse without a condom within the past 6 months (B = 1.39, OR = 4.02, P = .04), knowing the serostatus of sexual partners within the past 3 months (B = −3.83 OR = 0.02, P < .001), and having social support (B = 0.75, OR = 2.10, P < .001) increased the likelihood of disclosure. The overall regression (x 2 ) value reached significance at 103.56 (P < .001), whereas the Hosmer–Lemeshow test value of 2.3 (P > .05) did not, indicating that the overall regression model was well-fitting. Furthermore, the Cox and Snell’s R 2 correlation strength of .41 and the Nagelkerke R 2 correlation strength of .61 indicated that this model possessed considerable explanatory power.
Logistic regression analysis of the participants’ disclosure of HIV status.
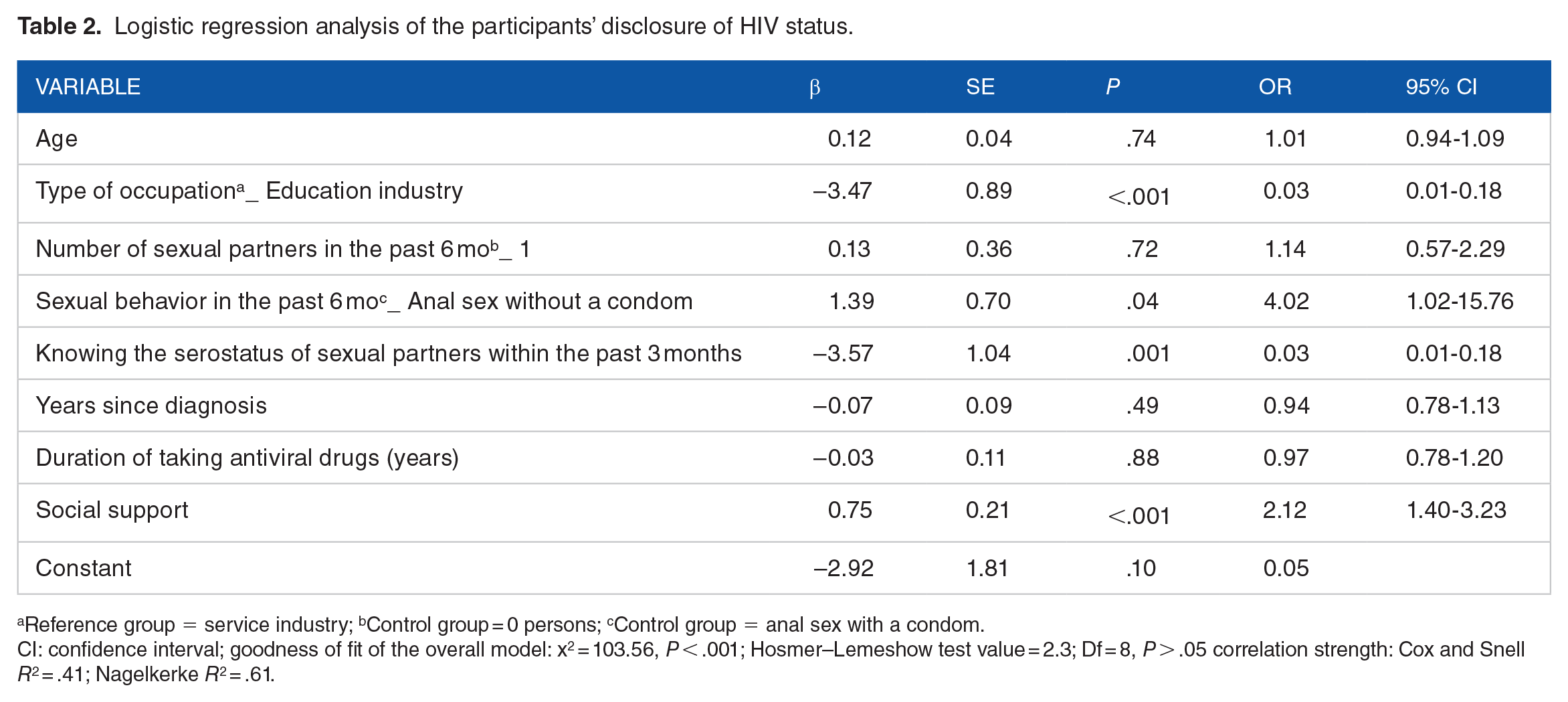
Reference group = service industry; bControl group = 0 persons; cControl group = anal sex with a condom.
CI: confidence interval; goodness of fit of the overall model: x2 = 103.56, P < .001; Hosmer–Lemeshow test value = 2.3; Df = 8, P > .05 correlation strength: Cox and Snell R2 = .41; Nagelkerke R2 = .61.
Discussion
Based on our analysis, disclosure of HIV-positive status among Taiwanese GBMSM is associated with IHP and social support levels. The GBMSM living with HIV who were receiving ART included in this study were mostly young and middle-aged with a undergraduate degree. The overall HIV status disclosure rate was 75.5%. Compared with a study conducted in the United States, more of our participants disclosed their HIV infection status (75.5%vs 58%). 30 GBMSM with HIV who were older and had higher IHP levels were less likely to tell others they had HIV. However, those who had the support of significant others, such as parents, close friends, partners, and siblings were more likely to disclose their HIV status. The most common reasons for disclosure were feelings of responsibility and obligation, followed by the desire to alleviate psychological tension. In addition, the disclosure rate was statistically significant, and there was no discernible difference in the pattern of disclosure before or after the “early access to ART for all” era. However, there were significant variations in the CD4 counts before and after the disclosure of HIV-positive status. Research in Western countries has shown specific reasons behind people living with HIV informing certain people of their HIV status. 31 When individuals with HIV needed help, before the “early access to ART for all” era, they were likelier to tell family and friends about their status. They may have had to tell their friends if they desired a closer relationship. As a result, GBMSM living with HIV are typically driven to adapt by seeking support and changing their attitudes. 30
This study found that 3 months after receiving illness awareness and information and counseling from their case managers, the majority of individuals disclosed their HIV status, regardless of whether they were diagnosed before or after the “early access to ART for all” period. Similar to our results, in a study conducted in Malawi, 32 the researchers reported that after disclosure counseling and training, about half of the participants declared their HIV status within a week or 2 of diagnosis. Regarding healthcare interactions, we observed that communication between patients and healthcare providers improved at the beginning of ART. HIV disclosure varied by sociodemographic factors. Older participants were less likely to expose themselves owing to their sociohistorical background, fear of upsetting sexual partners, loneliness and rejection, and their need for social support. 33 Regarding employment, those in the education sector were less likely to disclose their HIV status than service workers, and community and occupational stigma were negatively associated with disclosure. 34 We found that workers in technology may have a higher socioeconomic status and face less stigma, making them disclose their HIV status easily. On the contrary, cultural factors may make HIV disclosure difficult for educators despite being valued in both Eastern and Western cultures. According to a poll, most South African instructors did not disclose for fear of embarrassment, job loss, and biased rumors. 35 Educators living with HIV endure added stigma and discrimination in Eastern Confucian societies and often struggle to disclose their condition. In Taiwan, government, non-government, and advocacy organizations are raising HIV awareness, education, and acceptance. However, changes to firmly-held cultural values take time.
Sharing one’s HIV status can encourage safe sexual behavior, make it easier to find a regular sexual partner, and help better understanding one’s serostatus. 36 We revealed a correlation between HIV disclosure and stable partners, knowledge of partners’ serostatus within the previous 3 months, and protected anal contact. Individuals living with HIV disclosed their status to their partners and engaged in protected sexual activity based on their comprehension of early ART treatment. According to Daskalopoulou et al, 5 GBMSM with HIV are more likely to disclose their status to sexual partners with the same serostatus. Furthermore, the length of a person’s relationship has a significant impact on how aware they are of their serostatus.
In our study, no statistically significant difference was observed in the progression or regression of the disease. Ninety-five point five percent of the participants—precisely 191 individuals—were found to have an undetectable viral load. Interestingly, the likelihood of disclosure decreased as the number of years since diagnosis and the duration of antiviral drug treatment increased. This outcome aligns with the findings of earlier studies,5,30 which have also reported no correlation between reducing viral load and the act of disclosing one’s HIV status to a sexual partner. It was thought that the “early access to ART for all” perception had changed how infected people told their sexual partners about their serostatus. This result is similar to the findings of Fiorentino et al 37 in which he stated that people who took ART soon after being diagnosed were more likely to tell their sexual partners that they were HIV-positive. In our study, 116 people who were first diagnosed with HIV started taking ART right away, and 62.3% of them chose to tell others about their HIV status. The number of years since a patient has been diagnosed with HIV and the length of time of taking ART both reduce the likelihood of disclosing one’s HIV status.
Society often equates GBMSM with HIV because of IHP in the culture at large, which makes it harder to stop HIV from spreading. 38 We determined that while IHP was not the primary factor associated with disclosure, IHP of greater intensity would undermine social support. Additionally, the prevalence of elevated IHP was higher among older GBMSM living with HIV than in a previous study. 38
However, our findings were comparable to those from a study in South Korea, 39 which reported that individuals with high IHP levels—notably older lesbian, gay, and bisexual individuals—require mental health therapies. Although same-sex marriage was legalized in May 2019, and lesbian, gay, bisexual, and transgender people are more visible in Taiwanese society, the bill on ethnic minority conflict still exists. 40 We found that the participants received better support from their acquaintances and significant others than their family members. This observation corroborates the finding that most support comes from significant others and friends. 41
Owing to traditional Oriental values and the desire to avoid bringing disgrace upon the family, the amount of recognition and support is a significant factor in determining whether or not an individual discloses their HIV status. A Hong Kong study on factors affecting the well-being of GBMSM living with HIV reported that Chinese culture influences the self-disclosure of disease status and sexual orientation of GBMSM. 42 A longitudinal study investigating social support for individuals newly diagnosed with HIV revealed that friends, healthcare providers, and stable partners provided the most support, while family members offered the least. 43 Social support for GBMSM living with HIV plays a crucial role in facilitating access to necessary medical care. After disclosing their status, they experience increased social support, leading to a noticeable rise in their CD4 count. According to our analysis, working in the education field, being aware of partners’ serostatus, engaging in anal intercourse without using a condom, and receiving social support were predictors of HIV status disclosure.
Limitations
First, owing to the cross-sectional design, we were unable to make causal inferences. Second, as the data were self-reported, the accuracy of HIV status disclosure could not be determined. Third, the survey did not evaluate whether seronegative sexual partners utilized pre-exposure preventative measures. Finally, individuals who did not disclose their HIV status were excluded from this study.
Conclusions
Our results indicated that older GBMSM who had been diagnosed and began receiving treatment a long time ago were less likely to report their HIV status. Social support and awareness of the partner’s serostatus increased the likelihood of HIV disclosure. Further, GBMSM living with HIV who had little family support and significant IHP had low social support. In 2019, Taiwan became the first Asian country to legalize same-sex marriage. However, older GBMSM living with HIV continue to exhibit significant internalized stigma and require more mental health interventions. These findings suggest that the government, organizations working for the well-being of GBMSM living with HIV, and healthcare providers should educate GBMSM living with HIV and their partners earlier. Family care, family health education, family ties, social worker assistance, and nurse-led family groups help GBMSM living with HIV be accepted by their families.
Furthermore, we identified the primary determinants of HIV status disclosure. Our findings can be used to design interventions to increase the proportion of GBMSM with HIV who disclose their status, thereby safeguarding their seronegative partners. In addition, HIV-specific health education should be provided to family members to help them recognize and accept individuals living with HIV.
Footnotes
Acknowledgements
We express our appreciation to all participants and the healthcare providers for their support.
Funding:
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. We express our appreciation to all the 200 participants involved in the study and to other health providers for their support.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
T.-Y. Y., B.-H. L., W.-C. C. and F.-L. W. conceived, conceptualized and designed the study; T.-Y. Y., W.-C. C. and F.-L.W. performed the data collection and reviewed the article drafts. T.-Y. Y., B.-H. L., and F.-L.W. participated in collection, curation, and organization of all clinical data. All authors prepared the original draft and supervised the study. All authors have read and agreed to the published version of the manuscript.
Ethics Approval
This study was reviewed and approved by the institutional review board of the Mackay Memorial hospital (20MMHISO17e).
Consent to Participate
Informed consent was obtained from all individual participants in the study.