
Abstract
The provision of locally sustainable hearing aid device services is desirable in the Pacific Islands. The aim of the present study was (1) To assess the suitability of low-cost pre-programmable hearing aids in Samoa, a Polynesian nation of the Pacific Islands, and (2) To develop translations of established auditory rehabilitation questionnaires into the FaaSamoan language for clinical, public health, and research applications. A cross-over trial of 2 low-cost pre-programmable hearing aids among 20 adults in Samoa was conducted as part of a larger UN-funded global audiology study. The International Outcome Inventory for Hearing Aids, the International Outcome Inventory for Hearing Aids for Significant Others, and the Revised Hearing Handicap Inventory questionnaires were translated into the FaaSamoan language to assess the self-reported outcomes of study participants. Overall, high scores were measured for the self-reported outcome measures, suggesting good levels of use and satisfaction with the hearing aid devices. Overall, results found that once a hearing aid was fitted that 67.6% of participants reported no hearing handicap, 32.4% reported a mild to moderate hearing handicap, and no participant reported a significant hearing handicap.
Background
Age-related hearing loss is a significant disability among adults worldwide, with over 65% of adults over 60 years of age experiencing hearing difficulties.1-3 The provision of hearing aids is an effective method for reducing the adverse impact of hearing loss on communication skills, socio-emotional well-being, and quality of life. It is estimated that 80% of people with hearing loss are living in Low and Middle Income Countries (LMICs), where access to hearing aid services is limited or non-existent.4,5 Advances in hearing health technology, such as mobile applications for hearing assessments and low-cost pre-programmable hearing aids, offer the potential to increase access to auditory rehabilitation for people living in LMICs.6,7
The Pacific Island region is estimated to bear a significant burden of hearing loss among its adult population.1,8 As well as age-related hearing loss, additional hearing deterioration due to Type 2 Diabetes Mellitus is likely to be high among this population, where Non-Communicable Diseases (ie, Type 2 Diabetes Mellitus) are a public health crisis.9-12 Given the scarcity of hearing specialists in the Pacific Islands,8,13 hearing aids are generally available only through overseas donation programs. The closure of international travel during the COVID-19 pandemic highlighted the importance of locally sustainable models of hearing aid service provision.14,15
The Ear, Nose and Throat (ENT) Department of Samoa, a Polynesian nation of the Pacific Islands, was presented with an opportunity to participate in the United Nations’ global audiology study on Scalable Hearing Rehabilitation for Low- and Middle-Income Countries (SHRLMIC ). 16 The ENT Department and its evolving audiology service were thus able to investigate (1) the audiological profile of adults presenting to the ENT Clinic for ear and hearing complaints, and (2) the suitability of a hearing aid service delivery model that was low-cost, and did not depend on the skills of an audiologist. The primary recipients of this service would be adults at risk of age-related hearing loss (ie, adults aged 65 years and above), who currently represent 5.5% of the total population of Samoa. 17 The present report aims to highlight the Samoan experience within the context of the global study results. The findings should provide preliminary data to support health policy formulation for locally sustainable hearing aid services in Samoa.
Methods
The present report was prepared in accordance with SQUIRE reporting guidelines. 18
Ethical approval for the study was granted by (1) the Macquarie University Human Ethics Committee (Application number 7928), and (2) the Health Research Ethical Committee of the Government of Samoa.
Phase 1: Hearing profile and characteristics
The aim of Phase 1 was to describe the audiological profiles of adults presenting for ear and hearing health care to the ENT Clinic of Samoa. The study protocol is described in full elsewhere. 16 In brief, the ENT Department of Samoa was one of 23 clinics and 16 countries to participate in the first phase of the SHRLMIC global study. Data collection was performed from June to December 2020, and each participating study site was required to conduct a retrospective review of a minimum of 200 consecutive cases presenting for audiology review. Inclusion criteria were: (i) ⩾18 years of age, (ii) primary concern of hearing difficulties, (iii) worse ear 4-frequency pure-tone average (0.5, 1, 2, 4 kHz)>20 dB HL, and (iv) case did not present as part of a screening program. The following data were extracted from the clinical records: age, gender, occupation (where possible), residence (urban/rural), referral source, history of noise exposure, hearing device status (not previously aided, aided unilaterally/aided bilaterally/bone anchored device/cochlear implant), whether a hearing aid was recommended at this visit (yes/no), whether the case was referred for ENT or surgical remediation, pure-tone audiogram thresholds (including bone-conduction thresholds where available), otoscopic findings (where available), tympanometric findings (where available), and speech recognition scores (where available).
Phase 2: Fitting pre-programmable hearing aids
The aim of Phase 2 was to compare the objective and self-reported outcomes of 2 pre-programmable hearing aids, with the 2 devices varying in both power and number of selectable hearing profiles/programs. The study protocol is described in full elsewhere. 16 In brief, the ENT Department of Samoa was one of 4 clinics in 4 countries (India, Philippines, Samoa, South Africa) to participate in the second phase of the SHRLMIC global study. Given that Samoa has no capacity for manufacturing hearing aid earmoulds, the ENT Clinic was provided with standard sized retention domes and coupling for the hearing aids to enable their participation in the global study. All resources for successful completion of the hearing aid trial were provided by the SHRLMIC project leader (JN), which included provision of hearing aid batteries.
Each study site was required to recruit 20 consenting adult participants with a hearing loss in at least one ear who were willing to trial a hearing aid. In Samoa, the 20 participants were recruited during routine ENT Clinic service delivery during February-April 2021; the hearing aid trials were conducted during May-June 2021 by a senior Australian audiologist currently based in Samoa. A cross-over trial study design (Figure 1) was used to compare the objective and self-reported outcomes of 2 pre-programmable hearing aids; the hearing aid brand was Auditus Melior (A&M) and the 2 device models were the STPFP1 and the XTM A4. The objective outcomes were measured using Real Ear Measurements (REMs) with Callisto calibrated equipment utilizing a 65 dB modulated speech-shaped broadband signal. The self-reported measures were the International Outcome Inventory for Hearing Aids (IOI-HA), the IOI-HA for Significant Others (IOI-HA-SO), the Hearing Handicap Inventory for Adults/Elderly (HHIA/E), and the Practical Hearing Aid Skills Test – Revised (PHAST-R) questionnaires.
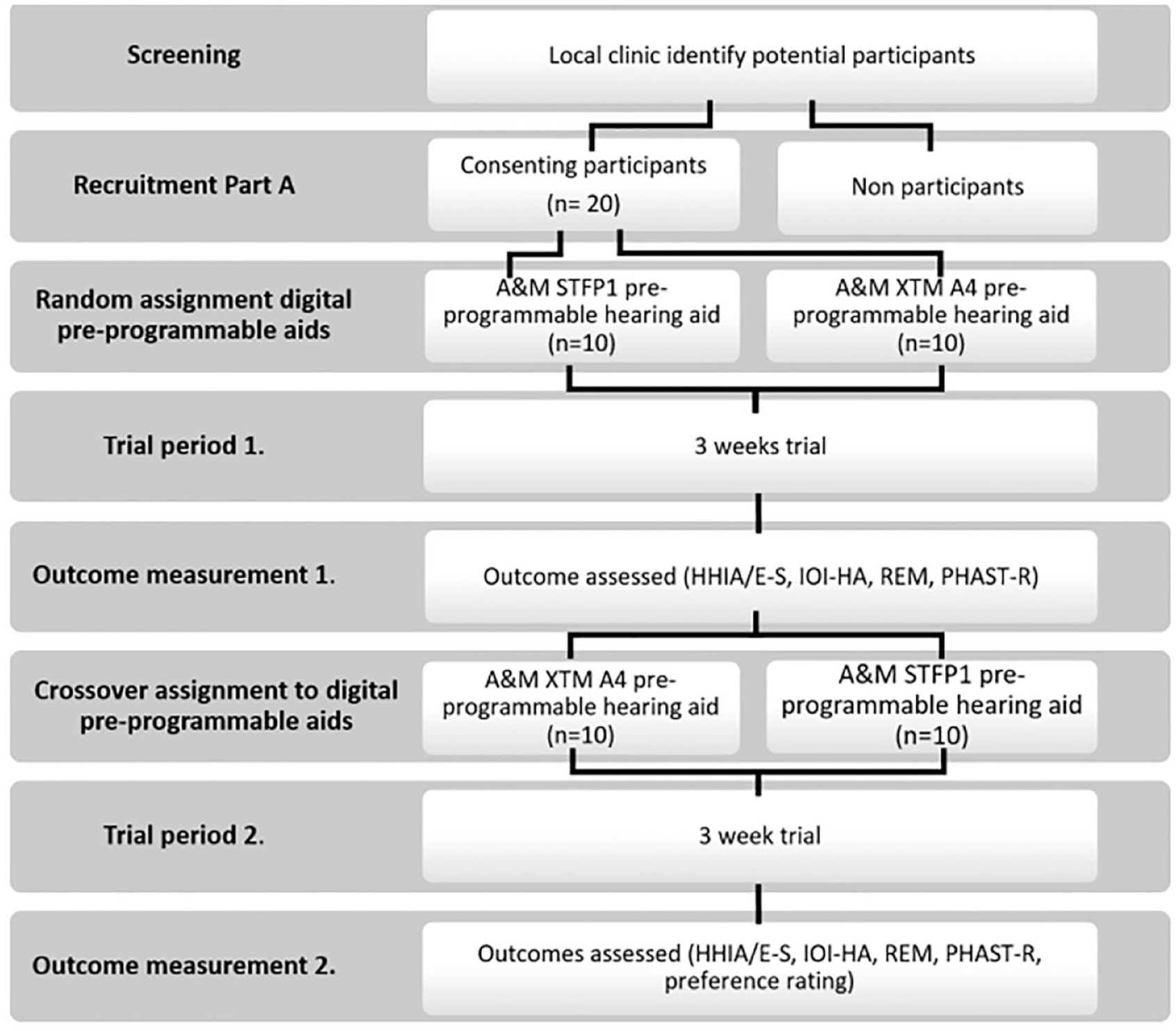
Overview of hearing aid trial cross-over methodology.
The ENT Department of Samoa engaged the services of a senior linguistics lecturer (GH) at the National University of Samoa for the translation of the IOI-HA and the IOI-HA-SO questionnaires from the original English.19,20 The translations were reviewed by a bilingual field expert (ENT Surgeon, PAF). The IOI-HA-SO questionnaire was added to the Samoan study procedure given that the majority of participants attended their audiology appointment with a support person. It was not possible to translate the HHIA/E questionnaire in time for the study, and this was administered with the assistance of bilingual accompanying caregivers or bilingual ENT nurses as appropriate.
Following their trial of both hearing aid devices, each participant was allowed to keep their preferred model. In this way, a preference was determined for the STPFP1 or XTM A4 model.
Three-month review (post-SHRLMIC global study)
Following completion of the SHLMIC study, the ENT Department of Samoa invited all Phase 2 participants for a 3-month review. By this time, the ENT Clinic of Samoa had selected the Revised Hearing Handicap Inventory (RHHI) for translation into the FaaSamoan language from the original English. 21 The RHHI combines the HHIA/E questionnaires into one questionnaire for adults of all ages. 21 The translation was again performed in collaboration with the senior linguistic lecturer (GH), and time permitted the participation of a university language student (MF) to enable improved cross-cultural translation practice. 22 The 3-month review appointments were an opportunity to formally field-test the Samoan translations of the IOI-HA, the IOI-HA-SO, and the RHHI.
Results
Phase 1: Hearing profile and characteristics
A total of 201 records were submitted to the SHRLMIC global study to represent the sample population of Samoa. The age range was 18 to 91 years, with a mean of 59.9 years (SD = 16.4 years). There were 106 female (52.7%) and 95 male (47.3%) cases. An overview of demographic information is provided in Table 1.
Demographic information overview of Samoan and SHRLMIC Global Study participants for Phase 1.

Scalable Hearing Rehabilitation for Low and Middle-Income Countries.
Audiometry results found that the 4-frequency average was 53.8 dB HL (SD = 22.8 dB HL; range 11.25-111.25 dB HL) for the right ears, and 54.5 dB HL (SD = 24.4 dB HL; range 7.5-110 dB HL) for the left ears. The 4-frequency average for the better ear was 50.3 dB HL (SD = 25.2 dB HL). Furthermore, the nature of hearing loss was conductive/mixed for 35 (17.4%) right ears and 27 (13.43%) left ears. An amplification device (ie, hearing aids) was recommended to 107 (53.2%) cases.
Phase 2: Fitting pre-programmable hearing aids
The Samoan sample population consisted of 11 female and 9 male participants (Table 2). The age range was 26 to 91 years, with an average of 69.9 years (SD = 13.2 years). One participant was fitted with hearing aids but returned them within a week, reporting that although he enjoyed improved hearing ability, he preferred to return to his quiet existence. A total of 19 participants therefore completed the study. Average hearing level for the right ear was 57.8 dB HL (Range 31.25-81.25 dB HL), and for the left ear 60.3 dB HL (Range 30.0-91.25 dB HL). Audiometry results indicated that bilateral fitting of hearing aids was appropriate for all participants.
Characteristics of Phase 2 study participants.
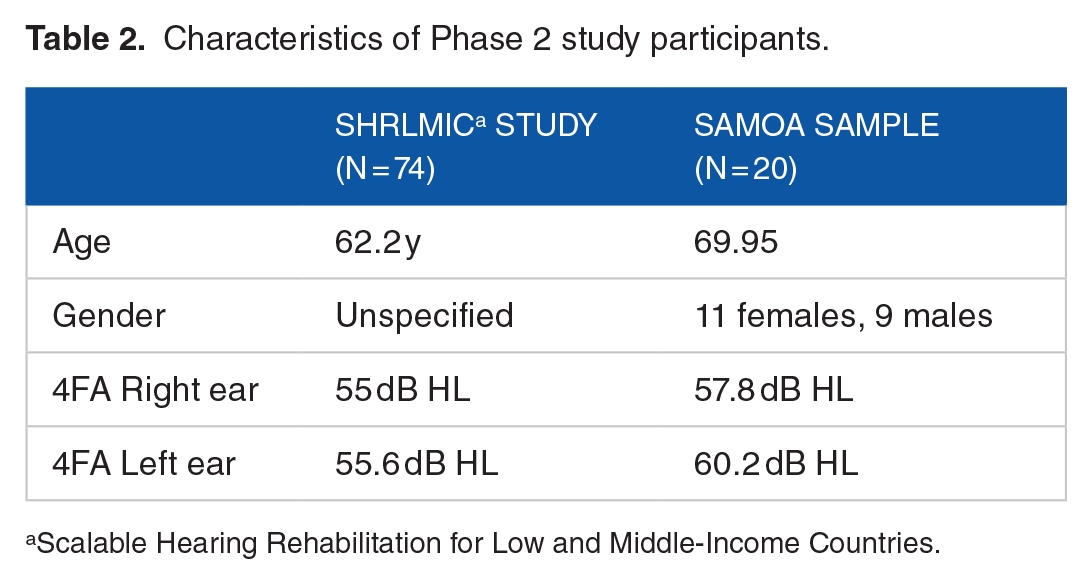
Scalable Hearing Rehabilitation for Low and Middle-Income Countries.
Real Ear Measurements (REMs) for the Samoan sample population were submitted to the SHRLMIC leadership team for inclusion in the overall project data analysis. 16 Overall SHRLMIC study results found that there was a relatively good mean fit to prescriptive target for both models of hearing aids. 16 Generally, neither hearing aid met the very strict criteria for a good fit (within 3 dB of target averaged across the 4 frequency range). 16 However the STFP1 device was an average of 6 dB from target, and the XTMA4 device was an average of 8 dB from target. 16
The SHRLMIC global study results reported that the PHAST-R questionnaires showed good handling skills of hearing aids by the participants. The majority of participants were able to successfully change the hearing aid batteries, remove and insert the device into their ears.
The self-reported outcomes for the Samoan population are summarized in Tables 3 and 4. The IOI-HA questionnaire was completed twice by all study participants (n = 19) for a total of 38 completed IOI-HA questionnaires. There were 14 participants who attended their appointments with a caregiver, and a total of 28 IOI-HA-SO questionnaires were completed. Following the methodology of the SHRLMIC global study, the questionnaire results were combined rather than reporting separate IOI-HA or IOI-HA-SO results for the first and second hearing aid devices: the rationale for this choice was that the questionnaires were completed following 2 weeks’ experience with each hearing aid device (ie, the 38 IOI-HA questionnaires and 28 IOI-HA-SO questionnaires all reflect a new hearing aid fitting experience).
Summary of self-reported questionnaire scores regarding outcomes of hearing aids.
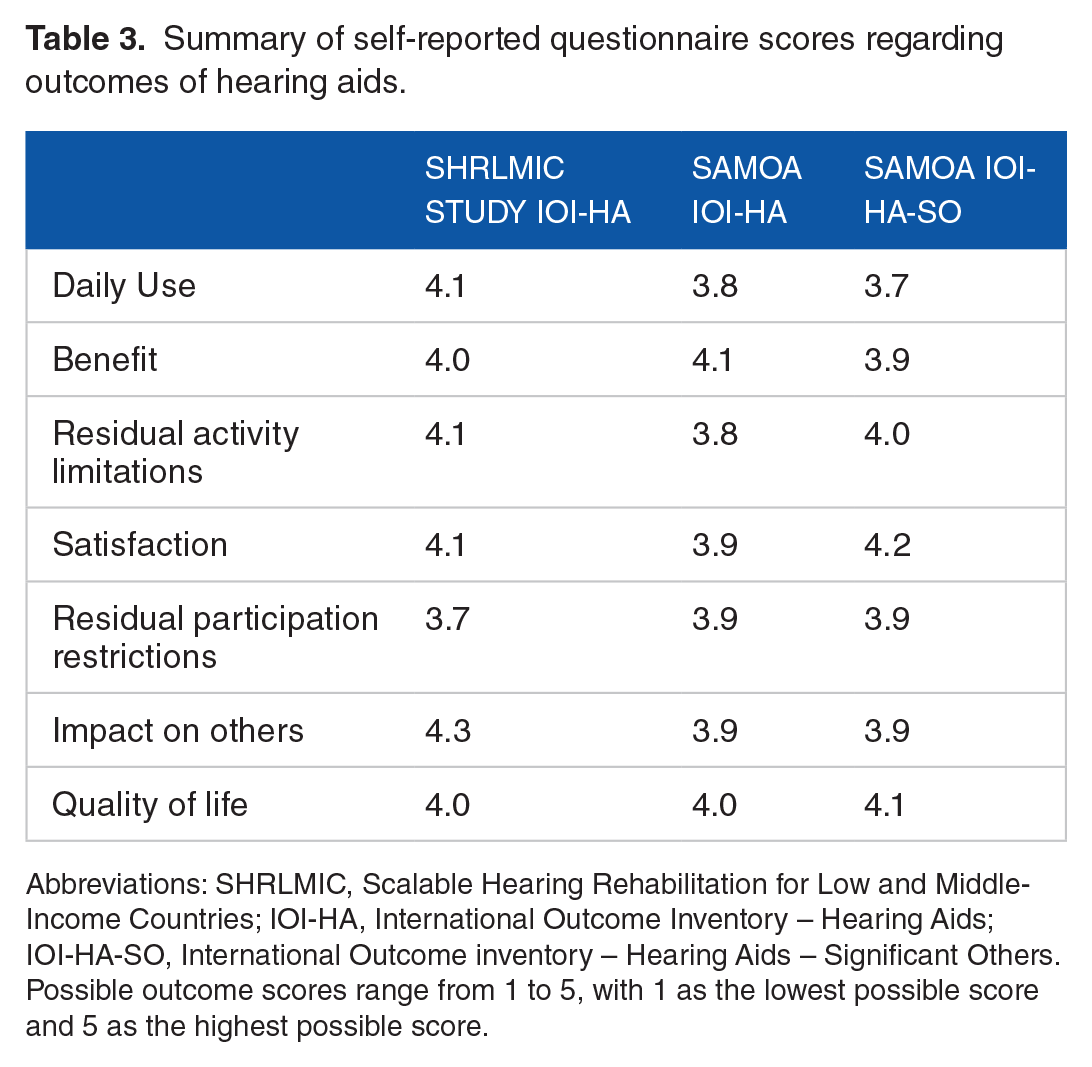
Abbreviations: SHRLMIC, Scalable Hearing Rehabilitation for Low and Middle-Income Countries; IOI-HA, International Outcome Inventory – Hearing Aids; IOI-HA-SO, International Outcome inventory – Hearing Aids – Significant Others.
Possible outcome scores range from 1 to 5, with 1 as the lowest possible score and 5 as the highest possible score.
Overview of Hearing Handicap Inventory for Adults and Elderly (HHIA/E) questionnaire results.

A total of 18 Samoan participants completed the HHIA/E self-report questionnaire at both hearing aid review appointments as required (N = 36), and one participant only completed the HHIA/E questionnaire once. The rationale for combining the results is the same as described above for the IOI-HA and IOI-HA-SO questionnaires. Overall results for the 37 completed HHIA/E questionnaires found that, once fitted with hearing aid devices, 67.6% of participants reported no hearing handicap, 32.4% experienced a mild to moderate hearing handicap, and no participant displayed a significant hearing handicap (Table 4).
At the completion of the SHRLMIC global study, a total of 8 (42.1%) Samoan participants preferred the XTMA4 hearing device, while 11 (57.9%) preferred the STFP1 hearing device.
Three-month review (post-SHRLMIC global study)
All 19 participants were invited for a three-month review, and 10 participants were willing to attend with their caregivers. Field-testing of the Samoan language versions of the IOI-HA, IOI-HA-SO, and RHHI questionnaires was performed, and participant feedback was encouraged regarding the translations. Suggestions for amendments were noted by the chief investigator (AK), who forwarded them to the translator (GH) for finalization of the FaaSamoan versions of these 3 questionnaires (Appendices).
Discussion
Similar to the results of the overall global SHRLMIC study, the findings for the Samoan cohort population revealed that adults generally present for help regarding their hearing difficulties once hearing levels have reached a moderate grade of hearing impairment. 16 Although listening difficulties may have been evident sooner, attendance for hearing healthcare was generally prompted by the well-known factors of hearing impairment causing significant distress or negative impacts on the quality of life of the person and their family.23-25 This situation usually indicates a readiness to accept an amplification device to address the hearing loss and associated communication difficulties. As stated above, there are 11 373 adults aged 65 years and older in Samoa, representing 5.5% of the total Samoan population (205 557). 17 While epidemiology studies will inform policy-makers of the number of adults who may benefit from hearing aid provision, the clinical data is more indicative/representative of adults with hearing loss in Samoa who are also ready to trial a hearing aid device, and able to access the hospital. This information may be more helpful as Samoa begins to explore the option of a government-subsidized hearing aid service from the ENT Department. As demonstrated in our study sample, it is important to note that even when hearing aid devices provide improved listening benefits, they may still be rejected for a number of reasons, including personal preferences for the comfort of a quiet environment. 26
Another finding that supports the provision of amplification services from the ENT Department is the fact that there was a high level of people presenting with a conductive or mixed hearing loss. Basing the audiology service at the ENT Department facilitates medical or surgical intervention for ear and hearing healthcare, a vital consideration in a region with one of the highest rates of ear disease in the world.27,28 Given the increased risk of impacted cerumen 29 and otitis externa 30 among hearing aid users, a future hearing aid service that includes ENT review at every appointment is recommended.
Overall, the Samoan participants of the hearing aid trial were satisfied with the amplification devices in meeting their hearing needs. This aligned with the results of the overall SHRLMIC global study, 16 as well as similar studies from both high-income nations and LMICs.19,31,32 From the audiologist perspective, the mobile application based software and standardized probe tips and coupling would eliminate the need for specialist qualifications and manufacturing services in basic hearing aid device provision. Participation in the SHRLMIC study promoted the recommendation that a basic and locally sustainable hearing aid service could be possible in Samoa under the supervision of an audiologist, with minimal training provided to the ENT nurses or other suitable health worker candidates.
Participation in the global study also built capacity for the audiology service in Samoa through the development of FaaSamoan language translations of the IOI-HA, IOI-HA-SO, and RHHI questionnaires. These will not only form part of the audiology clinical service, but will also prove useful for our public health and research activities. 33 The audiology clinic is working with the PEN FaaSamoa initiative to develop a hearing screening protocol for primary care providers for people living with non-communicable diseases, and a screening version of the RHHI questionnaire would be a suitable option for identifying people who may benefit from the specialist services of the ENT/Audiology Department.9,10 The RHHI will also be used during our outreach community visits to older adults, and should provide preliminary information on the socio-emotional impacts of hearing loss: in the absence of epidemiology studies, this will be useful for service provision planning until formal hearing survey data are available.
While the ENT Clinic of Samoa was well-resourced to successfully complete participation in the SHRLMIC global study, the ethical dilemma of on-going care and support for people fitted with hearing aids was raised.14,15 At this time, there is an non-government organization in Samoa that provides a basic hearing aid service dependent on overseas donations and international partnerships. Study participants were referred to this organization as required. The issue of on-going care, maintenance and support of people fitted with hearing aids must be satisfactorily addressed if the ENT Clinic of Samoa is to implement and offer a hearing aid delivery service to the people of Samoa.
There were only 10 participants who accepted the invitation to return for a 3-month follow-up appointment following their hearing aid fitting and completion of the SHRLMIC global study. Given the importance of follow-up care and post-fitting counseling to optimize benefits of hearing aid devices, an assessment of follow-up rates and factors influencing attendance for follow-up should be included in the monitoring and evaluation of hearing aid delivery service implementation.23,34
Limitations
As stated above, a limitation of the present study was that the IOI-HA, IOI-HA-SO, and HHIA/E questionnaires were not translated as per optimal practice prior to the study due to time limitations. Attempts were made to adhere to best practice for the translation of the RRHI within the context of Samoan resources.
The present report was written to highlight the option of pre-programmable hearing aids for our Samoan population. A limitation of the study was that barriers such as cost, transport, and access to the ENT Clinic were not investigated. This should be included in future studies that further assess the feasibility of implementing a locally sustainable hearing aid service in Samoa.
Recommendations
The formulation of a policy brief proposal is recommended to initiate hospital-based hearing aid device provision at ENT Clinic. The hearing aid device service should be implemented gradually, with monitoring and evaluation activities to further guide the expansion/development of the service as national health budget allocations allow. According to the 2021 Census, the number of adults in Samoa over 65 years of age is 11 373 or 5.5% of the total Samoan population. This figure may serve as a starting point for budgeting for hearing aid provision among this age group. The low-cost pre-programmable hearing aids used in the present study were approximately $100USD (Western Samoan Tala $265).
The formulation of policy brief proposals should also be considered to facilitate improved outcomes for Samoan adults who are the recipients of hearing aid devices through overseas donation programs. These policies should highlight the capacity-development of audiology services at the ENT Department, in order to enable locally sustainable and high-quality on-going care for hearing aid recipients through such programs.
Conclusions
The participation of the ENT Department of Samoa in the global SHRLMIC study offered an opportunity to trial a model of hearing aid provision that may be locally sustainable. The hearing aids are low-cost, pre-programmable, and may be fitted by non-specialists. Participation in the study also enabled the translation of audiology questionnaires into the FaaSamoan language, which will benefit clinical, public health, and research audiology initiatives in Samoa. Our findings may be translational, and prove useful to our Pacific Island neighbors.
Clinical Messages
High satisfaction with pre-programmable hearing aids among hearing-impaired adults in Samoa
Pre-programmable hearing aids are a suitable and potentially locally sustainable option for low-resourced settings
Successful development of auditory rehabilitation questionnaires in the FaaSamoan language for use in clinical settings and research purposes
Supplemental Material
sj-docx-1-his-10.1177_11786329231212122 – Supplemental material for High Levels of Satisfaction Among Hearing Aid Users in a Pilot Study for Sustainable Low-Cost Auditory Rehabilitation Services in Samoa
Supplemental material, sj-docx-1-his-10.1177_11786329231212122 for High Levels of Satisfaction Among Hearing Aid Users in a Pilot Study for Sustainable Low-Cost Auditory Rehabilitation Services in Samoa by Annette Kaspar, John Newall, Sione Pifeleti and Galumalemana Hunkin in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329231212122 – Supplemental material for High Levels of Satisfaction Among Hearing Aid Users in a Pilot Study for Sustainable Low-Cost Auditory Rehabilitation Services in Samoa
Supplemental material, sj-docx-2-his-10.1177_11786329231212122 for High Levels of Satisfaction Among Hearing Aid Users in a Pilot Study for Sustainable Low-Cost Auditory Rehabilitation Services in Samoa by Annette Kaspar, John Newall, Sione Pifeleti and Galumalemana Hunkin in Health Services Insights
Supplemental Material
sj-docx-3-his-10.1177_11786329231212122 – Supplemental material for High Levels of Satisfaction Among Hearing Aid Users in a Pilot Study for Sustainable Low-Cost Auditory Rehabilitation Services in Samoa
Supplemental material, sj-docx-3-his-10.1177_11786329231212122 for High Levels of Satisfaction Among Hearing Aid Users in a Pilot Study for Sustainable Low-Cost Auditory Rehabilitation Services in Samoa by Annette Kaspar, John Newall, Sione Pifeleti and Galumalemana Hunkin in Health Services Insights
Footnotes
Acknowledgements
The authors wish to acknowledge Dr Penaia A. Faumuina who provided bilingual field expertise for the review of the translations of the clinical questionnaires. The authors would also like to acknowledge Miracle Faautu who participated in the translation of the clinical questionnaires during her final student year at the Centre of Samoan Studies (National University of Samoa). We would also like to thank the 20 participants who took part in the present study.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Samoan project site received funding under the following global project: Project reference: UNOPS/CFP-2020/001/ATSCALE. This activity was funded by USAID in support of ATscale and managed by the UNOPS.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AK: data collection, data analysis, preparation of manuscript. JN: study design, manuscript review. SP: manuscript review. GH: data collection, manuscript review.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.