
Abstract
Residents in long-term care settings do not receive adequate support for hearing and vision devices. This study aimed to identify factors influencing support for residents’ daily use of hearing and vision devices. Semi-structured interviews with 23 staff were analyzed deductively to categorize data within the Capability, Opportunity, and Motivation model of Behavior (COM-B), and then inductively to identify themes and subthemes within each domain guided by the Theoretical Domains Framework. Capability factors included a lack of skills in managing and maintaining sensory devices, interpersonal communication skills, and forgetting about device use. Opportunity factors included device management not being included on care task lists and inaccessible sensory devices. Staff reported a strong sense of duty and positive feelings about providing device support, reflecting high motivation.
• This study identifies behavioral factors contributing to sensory device support in long-term care at the individual, interpersonal, and organizational levels. • It provides recommendations to improve hearing and vision care in long-term care settings.
• Interventions should include training to equip staff with the knowledge and skills for effective support for hearing aids and glasses. • Sensory device support tasks should be integrated into staff daily care routines. • There is a need to establish best practice guidelines for sensory device support and management in long-term care settings.What this paper adds
Applications of study findings
Introduction
Hearing and vision impairments are highly prevalent among older people living in long-term care settings, with approximately 90% experiencing hearing impairment and over 50% experiencing vision impairment (Bowen et al., 2016; Cohen-Mansfield & Taylor, 2004). Hearing and vision impairments negatively impact physical, psychosocial, mental, and cognitive well-being (Mick et al., 2014; Tseng et al., 2018). Vision impairment, for instance, limits independence, daily functioning, and mobility (Gallagher & Jackson, 2012), as well as increasing the incidence of disorientation, confusion, and falls (Rees et al., 2009; Stelmack, 2001). Hearing impairment similarly impacts quality of life, causing communication difficulties, loneliness, social isolation, and frustration (Bennett et al., 2022; Heffernan et al., 2022). When hearing and vision impairments coexist “dual sensory impairment,” difficulties are even more pronounced (Yamada et al., 2014). With the high prevalence of dementia in long-term care affecting up to 75% of residents (Gordon et al., 2014), hearing and vision impairments can further exacerbate responsive behaviors, leading to greater social isolation, increased medication use, use of physical restraints, and higher care costs (Heine & Browning, 2014; Leroi, 2020). Furthermore, hearing and vision impairments impact paid carers and family members resulting in depression, exhaustion, relationship stress, and increased care burden among care partners (Lawrence & Murray, 2009). Hearing and vision interventions (e.g., hearing aids and glasses) are effective in improving communication and reducing depressive symptoms and loneliness among older adults (Dawes et al., 2018; Punch & Horstmanshof, 2019) and improving outcomes for people living with dementia (Leroi et al., 2020). Addressing hearing and vision impairment is therefore important for optimizing quality of life for older people.
Despite the high prevalence of hearing and vision impairments among people in long-term care settings, these impairments are often undertreated (Andrusjak et al., 2020; Leroi et al., 2020). Many residents do not receive adequate support, including with hearing aids (e.g., insertion, battery changes) and glasses, environmental adjustments (e.g., noise reduction, improved lighting), and communication strategies (e.g., speaking face to face) (Andrusjak et al., 2020; Cross et al., 2022). As older people often experience reduced dexterity, many residents may struggle to manage their own hearing aids, with most residents relying on staff for hearing aid support (Punch & Horstmanshof, 2019). This dependence is even more pronounced for residents with dementia (Bott et al., 2022). A recent review highlighted several barriers to the identification and management of sensory loss in long-term care settings (Andrusjak et al., 2020). These included challenges with use and maintenance of assistive aids (e.g., hearing aids and glasses), limited access to specialists such as audiologists and optometrists, “unfriendly” sensory environments (e.g., high levels of background noise), reduced cognitive capabilities among residents, and a lack of staff knowledge about prevalence, impact, and support for hearing and vision impairment (Andrusjak et al., 2020). While training to improve staff knowledge about hearing aid maintenance may support hearing aid use, some studies reported that hearing aid use among people with hearing loss in long-term care remains low (Cohen-Mansfield & Taylor, 2004; Cross et al., 2024b). Although some interventions have focused on staff training, they show mixed results and have addressed only a narrow range of factors (Cohen-Mansfield & Taylor, 2004; Cross et al., 2024b). Broader, more comprehensive interventions are lacking, representing a significant missed opportunity to improve residents’ quality of life.
To support the hearing and vision needs of long-term care residents, it is therefore essential to understand the factors that influence staff in providing day-to-day support for sensory device use. These factors include those related to staff, residents, the local environment, and the broader care ecosystem. We used a health behavioral model to describe these factors: the
The aim of this study was to identify and describe the factors influencing long-term care staff support for residents’ daily use of hearing and vision devices for residents according to the COM-B model. By systematically mapping these factors using a behavior change framework, this research will provide the foundational evidence needed to develop targeted interventions that enhance staff support for sensory device use in long-term care settings.
Methods
Study Design and Setting
This qualitative study utilized semi-structured interviews with staff working in one long-term care facilities in Perth, Australia. The aim was to identify factors that influence how staff support day-to-day device use which involved the following aspects:
• Each morning, check glasses are on and clean.
• Each morning, check that hearing aids are on, inserted correctly, on correct ears, and working.
• Each evening, check hearing aids and personal listening devices are removed, wiped clean, and stored safely and batteries are conserved.
• Each week, check frames are well aligned and in good order.
The interview topic guide is provided in supplementary material. This study and related findings are reported in line with the consolidated criteria for reporting qualitative research (COREQ) (Tong et al., 2007). Ethical clearance for this research was granted by the Human Research Ethics Office of The University of Queensland (Ethics ID number: 2022/HE001477).
Sample
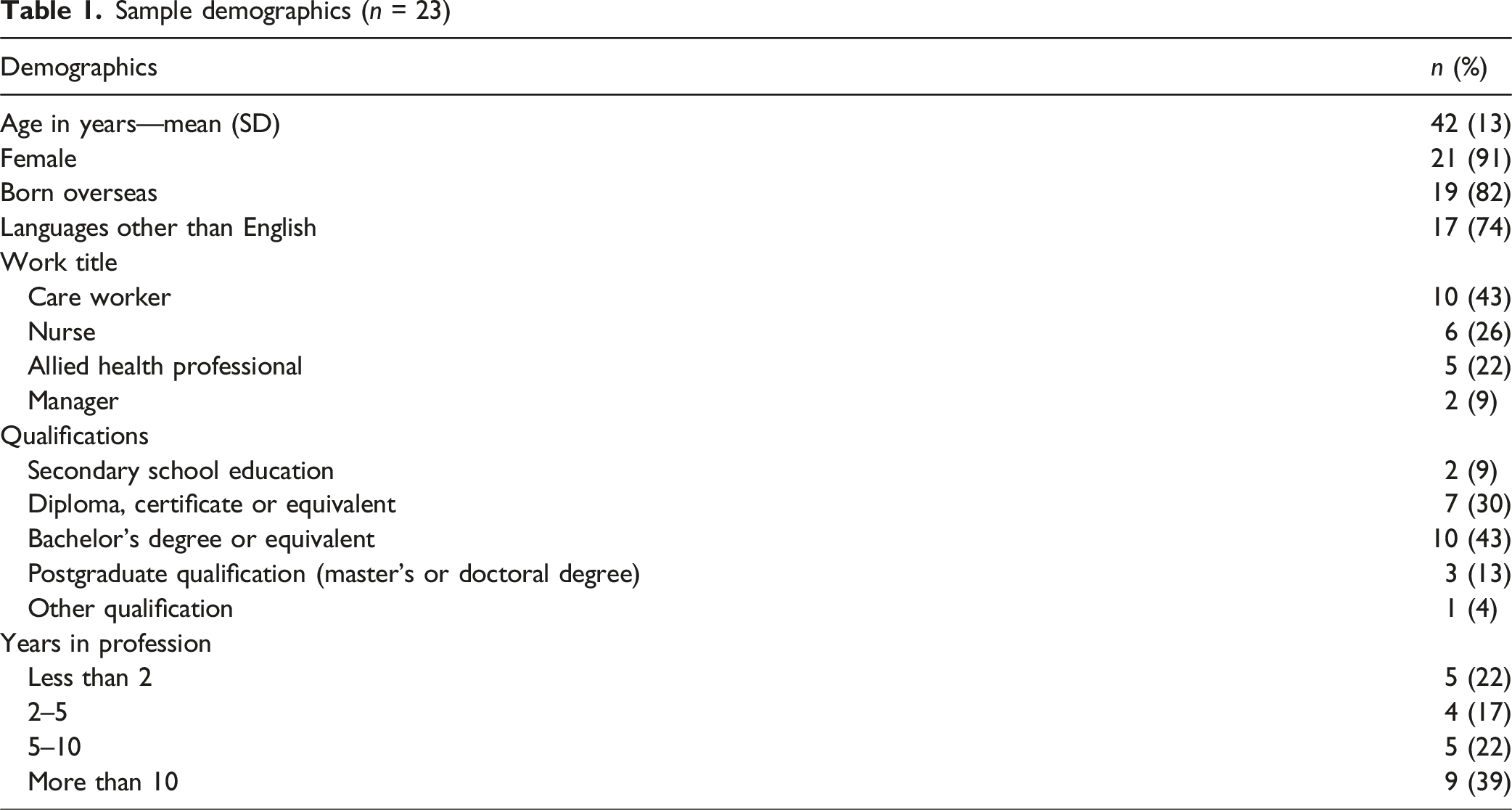
Long-term care staff were approached directly by senior managers at two sites of the facility. Staff were eligible to participate if they were currently working in long-term care in Australia and provided daily care support to residents, were able to provide informed consent, and self-reported adequate conversational English. Maximum variation purposive sampling was applied to ensure diversity across roles (e.g., nurses, healthcare assistants, and managers), seniority levels, and ethnicity.
Data Collection and Analysis
Interviews were conducted face to face by a trained research assistant (N.R.) at the long-term care setting where participants worked between May 2023 and August 2023 and lasted between 30 and 60 min. Participants completed a demographic questionnaire at the beginning of the interview, and with their permission, the interviews were audio-recorded.
Recordings were transcribed verbatim, de-identified, and verified for accuracy against the original digital recordings. Data were analyzed using a hybrid analytic approach, combining deductive (COM-B-guided coding) with inductive (data-driven thematic) analysis. Three members of the research team (N.E.S., C.M., and N.R.) independently conducted a deductive analysis to map potential factors influencing day-to-day device use support to the COM-B model: Capability (physical and psychological), Opportunity (physical and social), and Motivation (automatic and reflective). Subsequently, two researchers (N.E.S. and C.M.) conducted an inductive thematic analysis, following Braun and Clarke’s method (Braun & Clarke, 2006). This included familiarization with the data, generation of initial codes, development of themes and subthemes, and iterative refinement. These themes were then aligned, where possible, to the 14 domains of the Theoretical Domains Framework (TDF) (e.g., knowledge, social influences, environmental context, and resources) (Atkins & Michie, 2015) to more easily inform implementation strategies. Where TDF domains were too broad to fully capture specific findings (e.g., “Social influences” did not sufficiently capture nuances such as “residents’ reactions to staff support”), new themes were generated to preserve the richness of the data. Microsoft Excel was used to organize and interpret the data within the COM-B and emergent themes. Independent coding was cross-checked, and any discrepancies were discussed until resolution was reached between the two researchers (N.E.S. and C.M.). The characteristics of the participants were summarized using descriptive statistics.
Findings
Sample demographics (n = 23)
Summary of themes and subthemes

Psychological Capability
Knowledge and Skills
Staff knowledge of residents’ hearing and vision needs varied. Some were unaware of whether residents owned hearing aids or glasses. Conversely, other staff were well-informed about which residents use glasses or hearing aids, and the health conditions (e.g., dementia) that affect their use. These knowledgeable staff were also aware of factors related to hearing aid use for individual residents, including those that refused to wear them, those that frequently misplaced their hearing aids, or those in need for assistance, particularly among those with dementia. They highlighted how dementia impacts residents’ ability to manage their hearing and vision devices, leading to challenges such as forgetting to wear them, residents not being able to check if devices were working properly or being able to use them. P23: “I don't think it's coming from a lack of care. I think it's more, oh, I didn't know he wore hearing aids, or I didn't know they wore hearing aids.” P20: “Well the dementia client will not be able to tell you if their hearing aid is dirty, need cleaning or it's not working. All you can see most of the time is behavior.”
Staff attributed this inconsistency in knowledge to staffing arrangements. They explained that agency staff, who may only work once or twice a week, have limited familiarity with residents, while those who work more consistently know the residents better. Participants also added that new staff have less knowledge than those who have been working for longer periods and have developed a deeper understanding of the residents’ needs over time. P15: “Most of the carers, it's a lot of changing of different carers. So, it's not like a routine that carer knows the client.”
Staff expressed a lack of knowledge and skills pertaining to device management. Knowledge of hearing aids was challenging, due to the variety of types and the insufficient guidance provided, as many devices lacked clear user manuals or instructions. While some staff reported that they were comfortable with basic tasks such as checking if hearing aids were in the correct ears and whether they were functioning, they lacked knowledge of more advanced tasks like changing batteries, properly using the devices, and inserting them correctly. Cleaning of glasses and hearing aids was also problematic, with staff unsure of appropriate cleaning methods, often resorting to using tissues or personal clothing. Staff were unsure how to check the frames and screws of glasses. Consequently, problems with devices were only addressed once they were broken or not working. P22: “I think there's a lack of knowledge around how to change batteries, how to use the devices, how to insert them correctly. It's quite often, not until something like a pair of glasses actually break or something happens to them, that it's escalated and, as a result, actioned.”
Staff also noted limited understanding of the importance and value of hearing aids, further hindering effective device management.
Despite these challenges, some staff reported developing their skills through experience. P10: “They never teach us. So, we learn on job.”
Many participants highlighted their interpersonal skills and how these were important in supporting device use. Staff reported that they showed empathy and adapted communication strategies based on individual resident needs, particularly for those with dementia. They employed strategies including demonstrating actions to explain how devices worked and showing the devices to residents beforehand to ensure understanding. For residents who did not want to put on their glasses or hearing aids, staff reported trying gentle persuasion. Staff reported that a personalized approach—such as suggesting that a person would need their glasses to complete a crossword puzzle—was effective in encouraging residents to use their sensory devices.
Some staff highlighted using gestures, visual cues, and mimicking actions or pointing to help residents with comprehension difficulties. They demonstrated how to use hearing aids or glasses, and when hearing aids were broken, they relied on written communication or speaking loudly. P9: “Because sometimes we just have to make visual cues for them to understand what we're trying to do for them.”
Some staff reported a lack of communication skills, often failing to relay or document residents’ sensory care needs, such as lost glasses during handovers. P7: “I think it need a little bit more communication because one person got glasses, meet that person, need his glasses. And then if they don't have it, where is the glasses? Where it go?.. They need assist. That's why when the glasses have to be in the iCare (the electronic care record system), whatever, in the handover.”
Memory, Attention, and Decision Processes
Staff reported observing residents’ hearing and vision difficulties through facial expressions or by noticing dirty, crooked, or broken glasses.
Most staff reported frequently forgetting daily tasks related to sensory support, including changing hearing aid batteries, putting on hearing aids, and conducting checks for functioning. Forgetting to carry out sensory support tasks was attributed by staff to feeling rushed or under time pressure. P2: “Yes. Sometimes when it's rushed, we forgot to put the hearing aid as well. And then we realize, oh, we forgot to give him or her hearing aid, and we just go.”
Behavioral Regulation
Staff reported needing to manage other responsibilities while adjusting their work to accommodate extra time needed to support residents with dementia, ensuring flexible hearing and vision support. P16: “Also, we re-approach them after a while, 10, 15 min, 20 min because they change quickly. And they might be next minute they say, ‘Oh, thank you so much for giving my glasses,’ and they're happy.”
Physical Opportunity
Time
Staff believed that there is not enough time in their busy work schedules to support hearing and vision device management, or to check each resident’s care plan in relation to sensory needs. Lack of time is exacerbated by understaffing, changes in staff, and at the start of shifts. P22: “Yes [to times when staff might forget to include device support in their routine] if they're under pressure, if they're feeling rushed, if they're running on lower than normal staffing levels, if there's been an event in the area that morning.”
Barriers
Participants discussed several barriers to supporting device use related to residents’ health conditions, including hair and skin conditions that made it difficult to wear hearing aids and glasses. Other barriers included poor fit of glasses and hearing aids, breakages, malfunctioning hearing aids due to wax buildup, hearing aid batteries being flat, and challenges with keeping hearing aids dry (e.g., during showering). P17: “Because one of our clients, she had a excoriation skin problem on the ear...also, she had hearing aid and glasses at the same time.”
Prompts and Cues
Staff highlighted the absence of a clear task list to guide the daily management of hearing and vision devices, making it challenging to consistently meet residents’ needs. Some participants mentioned that including hearing support tasks (e.g., put on hearing aids) into the electronic task list system Clinical Manager was helpful and enabled more consistent support for hearing aids. Although staff colloquially referred to the system as “iCare,” Clinical Manager is the current electronic health record platform used by all clinical staff to record and access task lists, care plans, handover notes, and progress documentation.
Additionally, staff reported that some residents will remind staff about their hearing aids or request assistance with them. Staff also mentioned visual prompts within residents’ rooms, such as posters or small signs with notes about hearing aids: P2: “Right now, they're putting in every room who have the hearing aids, the small notes, like please help me with my hearing aid, so that we know who have a hearing aid, who doesn't have.”
Material Resources
Staff reported that resident care plans are essential references for sensory needs, such as whether a person wears glasses or hearing aids, though some noted that hearing or vision information on care plans may not always be current. New staff reported that they learn from both the care plans and experienced colleagues, with registered nurses providing instructions about hearing aids and giving hands-on training. P22: “And then hopefully they read their care plan, which would have the information in it for them to be informed around the individual.”
Although staff reported that they knew where to find information in the care plans and commented about the importance of regularly checking care plans, staff reported that they do not consistently take the time to read and use this information. Additionally, staff reported limited awareness of clinical protocols and procedures for managing hearing and vision impairment, as well as for assisting residents. P5: “I'm not sure about that [policies and procedures] with the [Name aged care setting].”
Several participants reported a lack of formal training about supporting residents with hearing aids, stressing the need for such training. Some mentioned the availability of hearing aid manuals; while some aids come with clear, user-friendly instructions, others do not. P10: “No, actually about the hearing aids and the glasses, we don't have a video. We don't have it. They never teach us. We learn on job.”
Accessibility
Staff reported challenges in discovering where each resident’s glasses and hearing aids were stored because storage locations differed. For residents with cognitive impairment or dementia, devices were typically stored in medication cupboards. Other residents usually keep their glasses or hearing aids in their rooms, often on bedside tables or in drawers. Some residents misplaced their devices. Staff changes meant that new staff did not know where a resident’s glasses or hearing aids were kept. Staff emphasized the need for a consistent storage place, particularly for residents with visual impairments, because people with visual impairments found it more difficult to find their devices. P6: “Some people I think either misplace them or stash them somewhere and don't quite remember where they've stashed them for safekeeping.”
Another issue that affected accessibility of glasses and hearing aids was the lack of labeling. Most devices were not labeled with the residents’ names, so that staff did not know who they belonged to. P7: “I wish the name is there. Because sometimes they mix up this one, taking this one. Even the staff think. Oh, that's her glasses. No, that's not the one. They're just guessing.”
Additionally, participants identified accessibility of care plans as a barrier to readily accessing information about residents’ sensory needs. Managers also discussed the challenges associated with changing from paper-based care plans to electronic systems. A shortage of iPads and laptops and technical problems limited access to electronic care plans. Agency staff do not have access to electronic care plans, hindering continuity of care. Staff reported that electronic care plans are not easy or quick to use, cannot be printed for reference, and do not provide concise summaries of care needs. These challenges mean that staff do not feel they have an easy way to be informed about residents’ needs. P22: “They all have access to be able to do it, but it's not user-friendly. They have to go out of their way to access it and the system is not quick to give them the information.”
Social Opportunity
Cultural Norms
Managers reported that effective care depends not only on the confidence and knowledge of staff but also on their cultural and language ability. P22: “I think differences in levels of understanding of English, being culturally and linguistically diverse, can put people off reading if there's too much information there. So, we try to keep it simple.”
Some staff expressed a sense of religious duty, which guides them to perform their tasks. P19: “God is watching us. So, I'm fear of God, I do not fear of human being.”
Organizational Culture
Staff described the work culture as positive, reporting that managers are supportive of the provision of sensory care, and informally educate staff about support for hearing and vision needs. Staff reported that managers were approachable and encouraged staff to seek support and assistance whenever they needed. P3: “Say someone needed assistance in how to put hearing aids in or the type of stuff that they should be looking for to know if the hearing aid/glasses are working, the managers are always great at taking that opportunity to educate you.”
Interpersonal Influences
Participants recognized a need to assist residents with dementia in using their hearing aids and vision devices. Residents with dementia often forgot about their devices, lacked insight into their hearing or vision difficulties, and struggled with checking and using devices properly. P16: “And then we always tell them, ‘You need your glasses if you want to read that book’. Some of them they understand, some of them they don't know what's going on.”
Some residents with cognitive impairment frequently misplaced glasses or hearing aids, took others’ glasses or hearing aids, or hid them. Consequently, families may refuse to provide hearing aids due to the cost of having to replace lost devices. P15: “The family didn't buy. I'm pretty sure they stopped buying the hearing aids because she will take them out.”
Although nurses reported encouraging the use of hearing and vision devices, there was uncertainty about whether hearing and vision care policies were effectively monitored or enforced. P22: “Are they [hearing and vision care policies and procedures] enforced? They should be.”
Residents’ Reactions
Residents with dementia require more time and patience to provide support. Their reactions to assistance with hearing aids or glasses were reported to vary depending on cognitive level, dementia stage, and mood. P16: “It's very hard with the dementia people because dementia people sometimes they don't like to wear the glasses. … They get annoyed with the sound that comes from hearing aids.”
To address these challenges, participants emphasized the need for adaptability, for example, returning later that day and trying a different strategy. Staff noted that insisting too strongly on using glasses or hearing aids could lead to verbal or physical aggression. P3: “Unfortunately, sometimes it's physical aggression. Sometimes it's verbal. So, you just have to be aware that if someone's going to get aggressive because of it.”
Social Support
Most staff highlighted a strong sense of team spirit and support, with carers working collaboratively with nurses and therapist assistants to ensure that hearing aids and glasses are functional and clean. Morning handovers facilitated communication. Staff reported seeking specialist support from colleagues when dealing with issues such as broken glasses or malfunctioning hearing aids and consulting occupational therapy teams for repairs. Some staff reported that evening shift staff may not consistently perform device support tasks, such as turning off hearing aids overnight so that the batteries are not flat by the morning. Inconsistent overnight device support created additional challenges for day staff. P23: “The evenings, to be honest, I think it gets missed. I think they're not taking them out. They're certainly not wiping them clean, and they're definitely not opening up that battery door.”
Participants added that families play a crucial role, advising staff on how to carry out daily checks or make repairs. Although repairs are usually quick, delays can occur if families are unavailable, or if the next of kin are slow to provide consent for repairs or replacement. Some families provide additional resources such as batteries or cleaning kits. Staff reported that families would raise concerns about sensory care, including lost glasses, or the cost of maintaining sensory aids. P23: “The complaints that I'm getting from family again, is we're going through too many batteries, etcetera.”
Automatic Motivation
Emotions
Staff expressed positive emotions such as happiness, satisfaction, and a sense of accomplishment in relation to supporting the hearing or vision needs of residents. However, they also expressed feelings of frustration, sadness, stress, and guilt when they felt that a resident’s sensory needs were not being met. P17: “The residents are happy and you get the needs that they have met, then you be able to go home happy.”
Impulses: Habit and Routine
Most staff indicated that supporting device use is part of their daily routine. In the morning, staff routinely check hearing aids and glasses. Some staff clean the devices before helping residents put them on, while others clean them only if they notice they are dirty. At night, some staff would remove hearing aids, take out batteries, and turn off the devices or place them on chargers. Staff reported that there is no formal routine for checking glasses, but they would report loose or broken frames to the registered nurse in charge. P16: “Just like we put in a routine. That person need a glasses, that person need a hearing aids. We have routine, we know how we work.”
Reflective Motivation
Goals and Intentions
Some participants emphasized that assisting with day-to-day device use is part of their duty and that sensory care is an essential part of carer responsibilities. P11: “This is also a responsibility, so we have to do it.”
Optimism
Staff were keen to support the use of hearing and vision devices, but they reported that this was often challenging. There were varying levels of optimism regarding the likelihood of residents using these devices regularly. P3: “... we would love for people to wear their glasses, and we'd love for them to wear their hearing aids, but it's just sometimes not possible.”
Beliefs About Consequences
Participants believed that supporting hearing aid and glasses use was beneficial to residents, helping improve communication, enabling residents to participate in conversations and group activities, and fostering social engagement and happiness. For residents with dementia, staff reported that supporting device use helped relieve agitation among residents, improved communication with residents, and strengthened relationships between residents and staff. P15: “Some of the clients that they get very agitated, they can't see, they can't actually read. So, it causes them to be upset.”
Staff also talked about how supporting device use improves residents’ safety, preventing falls and fractures, avoiding accidents, and maintaining independence. P1: “They can hear us properly, they can see things properly, which can avoid a lot of falls. So, it benefits them a lot. And it saves us, from shouting in their ear.”
Beliefs About Capabilities
Staff confidence varied significantly in supporting hearing aid and glasses use, with many lacking confidence due to insufficient knowledge and training. Less confident carers would offer sensory support but readily accept resident refusal, lacking the confidence to appropriately influence resident choice. P23: “You've got a dozen or so... that are quite confident... But I would say the biggest majority would say, oh, okay then. And just leave it.”
This contributed to inconsistent device use and family concerns about unmet sensory needs.
Professional Role and Identity
Participants emphasized that supporting device use and knowing which residents need assistance is a key part of their professional role. P10: “And I'm not here to do because of someone. I'm doing it because it's part of my job and I love... You know how they could say it, they say duty of care.”
Discussion
Our findings suggest that long-term care staff perceive a need to support hearing aid and glasses use and are motivated to provide that support but experience numerous challenges. Staff reported a lack of confidence and need for formal training in how to support hearing aid and glasses use. The workplace was reported to be positive and supportive of provision of sensory care: however, there were challenges with a lack of awareness of institutional hearing and vision care policy and practice, difficulties accessing information about sensory needs in residents’ care plans, and time pressures in delivering care. Staff turnover and time constraints were identified as factors contributing to a lack of familiarity with residents’ individual needs, which negatively impacted the consistency of sensory support. Sensory needs were sometimes neglected because they were not well integrated into care routines or communicated between staff. Cognitive impairments, such as dementia, create challenges due to residents’ fluctuating abilities, emphasizing the need for tailored support.
Our findings are consistent with previous studies identifying barriers such as lack of knowledge and low confidence among long-term care staff in supporting use of assistive hearing/vision devices, along with lack of formal training in hearing or vision care (Andrusjak et al., 2020; Cross et al., 2024a; Dawes et al., 2021; Punch & Horstmanshof, 2019). Additional barriers include suboptimal management of sensory aids, unsuitable environment, lack of communication among the team, and challenges associated with addressing sensory needs of residents with cognitive impairment. Importantly, it has been acknowledged that the barriers to providing sensory support to residents are complex and that collaborative multifaceted approaches are required. A supportive work environment and team collaboration are essential for effective device use. Furthermore, partnerships with families by involving them in care planning and educating them about the benefits of consistent device support and the impact of unmet sensory needs encourage their active role.
These findings align with the limited intervention literature identified in our introduction, highlighting the need for multifaceted interventions. While prior intervention studies have primarily focused on staff training for hearing aid maintenance with mixed outcomes (Cohen-Mansfield & Taylor, 2004; Cross et al., 2024b), our systematic exploration using the COM-B framework offers insights into why such narrowly targeted interventions may have had limited success. Specifically, our findings highlight that training alone (targeting capability) is insufficient when barriers related to opportunity (e.g., inaccessible devices and time constraints) and motivation (e.g., lack of confidence) remain unaddressed. This helps explain the variable results of prior interventions and reinforces the need for a comprehensive, multifaceted approach (Meyer et al., 2025).
Based on our findings, we propose the following seven recommendations to improve support for hearing and vision device use in long-term care settings: First, provide staff training and skill development focused on practical aspects of device use, such as insertion, cleaning, and troubleshooting. This addresses psychological capability gaps in knowledge, limited training access, and enhances confidence. Second, embed hearing and vision care tasks into daily routines and electronic documentation systems (e.g., checklists, care plans) to ensure consistency across shifts. This supports behavioral regulation, routine building, and reduces omissions due to time pressure or forgetfulness. Third, introduce visual prompts and reminders in resident environments and care plans to support memory, habit formation, and continuity of care during busy periods.
Fourth, ensure consistent storage and labeling of devices, and improve access to maintenance materials. This enhances physical opportunity by reducing device loss, confusion, and inconsistent placement of aids. Fifth, strengthen team communication and handovers and foster collaboration with families. This supports social opportunity by improving interpersonal coordination and reinforcing staff motivation through positive feedback and shared responsibility. Sixth, clarify and monitor institutional policies and ensure timely access to up-to-date care plan information to support consistent practice. Seventh, establish stronger partnerships and more consistent collaboration with the internal occupational therapy department to ensure specialized assessments and ongoing support, particularly for complex cases. This builds on existing team-based practices and addresses the need for accessible clinical expertise. Collectively, these recommendations address the multi-level factors identified in this study and provide a foundation for improving sensory support as part of routine aged care.
Limitations and Strengths
A key strength of this study is the use of the COM-B model and TDF, which provided a systematic, theory-informed approach to identifying factors that influence how staff support device use in long-term care. This enabled an in-depth exploration of the behavioral drivers underlying hearing aid and glasses use, thereby informing the design of targeted interventions.
As this study was conducted in a single long-term care facility, these findings may not be representative of all long-term care settings. However, a strength of the study was the in-depth insights obtained directly from aged care staff. The diversity across participants’ roles and employment levels offered a range of perspectives on daily challenges, skills, and knowledge gaps. This has contributed to a more comprehensive and inclusive understanding of the barriers and enablers to supporting hearing and vision devices in aged care. Although deductive analysis may limit findings to COM-B components and TDF domains, combining deductive analysis with inductive thematic analysis allowed us to uncover broader themes. This combined approach enhanced analytic rigor while capturing nuanced insights beyond the theoretical framework.
Conclusion
Staff in long-term care settings face multiple challenges with supporting daily use of hearing aids and glasses among residents despite being motivated to do so. These challenges span individual knowledge and skills, environmental and institutional constraints, and communication processes. Addressing these factors requires a multi-level approach that includes staff training, integration of sensory care into routine workflows, improved documentation systems, and clarification of responsibilities across clinical roles.
Multi-level interventions are therefore necessary to target factors at the individual, interpersonal, and organizational levels to improve quality of care for residents. Findings highlight the need for policy frameworks and best-practice guidelines that include sensory support as a core component of high-quality aged care. Future research should evaluate the implementation of targeted, behaviorally informed strategies and explore their impact on staff practice and resident outcomes across diverse care contexts.
Supplemental Material
Supplemental material -
Factors Influencing Staff Support for Sensory Device Use for People in Long-Term Care Settings
Supplemental material for Factors Influencing Staff Support for Sensory Device Use for People in Long-Term Care Settings by Najwan El-Saifi, Carly Meyer, Naomi Rose, Kasia Bail, Colette Browning, Dayna R. Cenin, Melanie Ferguson, Chyrisse Heine, Lisa Keay, Sheela Kumaran, John Newall, Emma Scanlan, Hamid R. Sohrabi, Melinda Toomey, Johanna Westbrook, and Piers Dawes in Journal of Applied Gerontology
Supplemental Material
Supplemental material - Factors Influencing Staff Support for Sensory Device Use for People in Long-Term Care Settings
Supplemental material for Factors Influencing Staff Support for Sensory Device Use for People in Long-Term Care Settings by Najwan El-Saifi, Carly Meyer, Naomi Rose, Kasia Bail, Colette Browning, Dayna R. Cenin, Melanie Ferguson, Chyrisse Heine, Lisa Keay, Sheela Kumaran, John Newall, Emma Scanlan, Hamid R. Sohrabi, Melinda Toomey, Johanna Westbrook, and Piers Dawes in Journal of Applied Gerontology
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the NHMRC Medical Research Future Fund, Grant No. MRF2007432.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.