
Abstract
Previous studies on patient satisfaction in Ethiopia focused on satisfaction with nursing care and outpatient services. Therefore, this study aimed to assess factors affecting satisfaction with inpatient services among adult patients admitted to Arba Minch General Hospital, Southern Ethiopia. A mixed method cross-sectional study was conducted among randomly selected 462 admitted adult patients from March 7 to April 28, 2020. A standardized structured questionnaire and semi-structured interview guide were used to collect data. A total of 8 in-depth interviews were conducted to collect the qualitative data. SPSS version 20 was used to analyze the data, and a P-value <.05 in the multivariable logistic regression was used to declare the statistical significance of the predictor variables. The qualitative data was analyzed thematically. In this study, 43.7% of patients were satisfied with the inpatient services they received. Urban residences (AOR 95% CI 1.67 [1.00, 2.80]), educational status (AOR 95% CI 3.41 [1.21, 9.64]), treatment outcome (AOR 95% CI 2.28 [1.65, 4.32]), use of meal service (AOR 95% CI 0.51 [0.30, 0.85]), and duration of hospital stay (AOR 95% CI 1.98 [1.18, 2.06]) were the predictors of satisfaction with inpatient services. Compared to previous studies, the level of satisfaction with inpatient services was relatively low.
Background
Patient satisfaction is a patient’s subjective evaluation of the service expectations with service obtained in a particular health facility. 1 It is a vital indicator of quality healthcare service. 2 In addition, patient satisfaction is one of the key factors that determine the patient’s trust in the health care facility. 3 Moreover, it has a significant impact on reducing staff turnover, 4 patients’ complaints about the cost of the service, and improving the financial stability of healthcare organizations. 5 Besides, it also affects treatment outcomes, 6 medical malpractices, 7 and retention of the patient. 4
Evidence shows a varying level of patient satisfaction with the admission service offered in health institutions across different areas. For instance, 90.0% of patients in the United Kingdom 8 and 98.0% in Iran 9 reported being satisfied with the inpatient services. Furthermore, studies in Germany, 10 Pakistan, 11 Nigeria, 12 and Ethiopia 13 showed that about 83.0% to 62.0% of patients were satisfied with the inpatient services respectively.
Different factors were identified to have significant influence on patient satisfaction with inpatient services. Age, 12 sex, 14 rural residences,12,13,15 income and service fee,12,14 number of service providers, 14 food service, 16 and hospital and ward environments13,14,16-19 were identified as the determinants of patient satisfaction.
Ethiopia had seen progress in health sector programs such as expanding and upgrading health institutions, increasing the number of skilled healthcare providers, and launching health sector development programs in the last 2 decades.20,21 However, there is still a gap in providing quality and patient-centered services. Moreover, the utilization of patients’ feedback to improve service quality is low, where only 28.6% of hospitals use feedback for quality improvement. 22
Although evidence highlights the importance of using patients’ perspectives, particularly satisfaction in improving service quality, studies in Ethiopian health institutions focused on satisfaction with nursing care23-26 and outpatient services,27-29 excluding satisfaction with inpatient service. Furthermore, most of these studies used general rating tools23-29 which cannot reliably measure patient satisfaction. 30 Thus, this study aimed to assess satisfaction with inpatient services and its predictors among adult patients admitted to Arba Minch General Hospital (AMGH), Southern Ethiopia, by using a mixed method.
Methods
Study area and design
Arba Minch Hospital is situated in Arba Minch Town, Southern Ethiopia. It has surgical, medical, obstetrics and gynecology, ophthalmic, pediatric, and neonatal intensive care admission units. The hospital has 200 beds for adult admission and a total of 1273 and 1121 adults respectively were admitted and discharged during the study period.
A sequential explanatory mixed method study was conducted in AMGH from March 7 to April 28, 2020. This method was chosen because the qualitative part of this study was based on quantitative findings and thus elaborates it in detail. 31
Source population and eligibility criteria
For quantitative
The source population was all adult patients discharged from medical, surgical, gynecology and obstetrics, and ophthalmic units of the study hospital during the study period.
Adult patients discharged from the selected admission units of the hospital during the data collection period were included in the study. Moreover, Patients referred to other hospitals, unable to provide information, and those admitted for the second time during the data collection period were excluded. Moreover, due to the possibility that patients who stayed less than 24 hours in the hospital may not have had enough information about admission services, they were also excluded from the study. 17
For qualitative
The source population was all adult patients discharged from selected units of the study hospital during the study period. Moreover, to get enough information about the services provided and the way they were delivered to inpatients, we selected those inpatients who had a history of previous admission and/or had an admission duration of at least 1 week for in-depth interviews.
Sample size and sampling procedures
For quantitative
For the first objective (magnitude of satisfaction with inpatient services), a single population proportion formula was used to estimate the sample size. Considering the proportion of patient satisfaction to be 62.0% (P) obtained from a previous study, 13 5% level of significance (α), 95% confidence level (Zα/2), and a margin of error of 5% (d), the sample size was 362. For the second objective (factors affecting satisfaction), the sample size was computed for each of the statistically significant factors reported in previous studies, and the factor which gave the largest sample size was taken. Using Epi-Info version 7.1.4.0 and assuming a confidence level of 95%, power of 80% and satisfaction among patients from rural areas to be 88%, satisfaction among patients from urban areas to be 76%, and the ratio of patients in urban (unexposed) to rural area (exposed) to be 2.3, 15 the sample size was 431. Therefore, taking the largest sample size (431) with a 10% non-response rate, the sample size for this study was 474.
To select study participants, first, we estimated the average monthly discharge of each ward (medical—274, surgical—244, Obstetrics and Gynecology—239, and ophthalmic—51) using a previous 1-year adult patients discharge report of the selected units of the hospital (9696) since the data collection was planned to be completed within 1 month. Then, the sample size was proportionally allocated for each unit based on the estimated number of discharges per month. By dividing the estimated number of monthly discharged patients in each unit by the proportionally allocated sample size for each unit, the “K” value (2) was determined. The first patient to be involved in the study was drawn using the lottery method from the first 2 (2) intervals. Finally, in cooperation with the head of each admission unit and based on eligibility criteria, participants being discharged from each unit were systematically selected daily from the discharge registration book, based on the “K” value until the desired sample size is reached from each unit.
For qualitative
A total of 8 patients were interviewed and participants of the interview were selected from all adult admission units on exit. Using a purposive sampling method, patients with a history of a previous admission to the study hospital and/or those with the longest (at least 1 week or above) duration of hospitalization were selected for an in-depth interview. The selection of participants from units was stopped after data were saturated or after adding more participants from the units does not generate any new information.
Operational definitions
Patient satisfaction was measured using the standardized tool with reported Cronbach alpha’s score of .89. 15 The tool consists of 28 items with the response on a 5-point Likert scale; 1 = very dissatisfied, 2 = dissatisfied, 3 = neutral, 4 = satisfied, and 5 = very satisfied. Then, the mean score of 28 individual satisfaction items was calculated by combining their responses. Finally, patients with a score greater than or equal to the mean satisfaction score (101.6) were classified as “satisfied” and those with a score below the mean score were considered “dissatisfied.” Predictor variables were socio-demographic and the patient’s clinical and non-clinical characteristics. Moreover, some of the terms used in this study were operationalized as follows:
Study variables
Patient satisfaction was a dependent variable of the study. Whereas, Socio-demographic characteristics of respondents (age, marital status, sex, residence, education status, income, ethnicity, religion, occupation), Clinical characteristics (duration of hospitalization, waiting time, number of nurses and physicians, treatment outcome, number of visits by providers, history of admission), and Non-clinical characteristics (food service, number of beds per ward, ward type, cleanness and comfortability of ward and hospital environment) were independent variables of the study.
Data collection tools and procedures
For quantitative
Primary data were the main source of data for this study, which were collected directly from patients that were discharged from the hospital in the quiet room. Data were collected using an interviewer-administered structured satisfaction tool adapted from the literature.13,15 The questionnaire has 3 components: participant’s sociodemographic characteristics (9), patient’s clinical and non-clinical characteristics (12), and satisfaction tool that was further divided into health professionals’ relationships, attitudes, and communication (10), health problem diagnosis and management (9), physical environment (7), and food service (2) dimensions.
The tool was primarily prepared in the English language and translated into Amharic. The training was provided for data collectors and supervisors for 2 days and the instrument was pre-tested on 5% (24) of the sample size in Ottona Hospital, Southern Ethiopia. Moreover, a daily check of the filled questionnaire was performed to ensure that it was complete. Missing variables, outliers, or other errors during data entry were checked using computer frequencies and sorting.
For qualitative
About 8 in-depth interviews were carried out with 5 semi-structured guiding questions by experienced 2 interviewers after quantitative data were analyzed and predictor variables were identified to explore why certain variables were significantly or not significantly associated with the outcome variable.
The questions were first prepared in English and then translated into the Amharic language. Furthermore, participants of the study were selected purposively from all adult admission wards on exit based on the eligibility criteria. The interview was done and audio-recorded in a quiet room to minimize disturbances. Field notes were taken during the interview process. The duration of the interviews was between 40 and 60 minutes.
Data management and analysis
For quantitative
First, the data were screened for completeness, and incomplete data were excluded. Epi-info version 7.0 was used for data entry and cleaning and Statistical Package for Social Science (SPSS) version 20 was used for analyses. Logistic regression analyses were conducted to identify the predictors of patient satisfaction and since using a P-value <.05 can fail to identify variables known to be relevant, variables with a P-value <.25 in the crude analysis 32 were included in the multivariable logistic regression analysis to retain significant variables and control the effect of confounders. The variables that were included in the multivariable logistic regression were sex, age, residence, marital status, religion, ethnicity, educational status, household income, occupation, frequency of hospitalization, meal service, duration of hospitalization, time of hospitalization, treatment outcome, admission mode, treatment fee, number of nurses visit, and number of physicians visit Then, an adjusted odds ratio (AOR) with a 95% confidence interval was estimated to assess the predictors of the outcome variable. Finally, a P-value <.05 was used to declare the statistical significance of the explanatory variables. Furthermore, model fitness was confirmed with the Hosmer et al 33 model fitness test with a P-value of .48 indicating that the model fits the data effectively. 33 Moreover, a multicollinearity diagnostic test was also performed, and the values of the variance inflation factor (VIF) for variables included in the model were <10 (1.03-1.94), indicating no multicollinearity. 34
For qualitative
Field notes data were organized and audio recorded data were transcribed verbatim and translated by the first and second authors and compared for consistency throughout the final write-up. Finally, data coding, sorting, and themes were developed based on the deductive approach of the thematic analysis procedure provided by Braun and Clarke. 35 The method was chosen because it was usually independent of a particular epistemological or theoretical perspective. Moreover, the method involves the use of preconceived notions and is flexible, making it easier to manage any changes made.35,36 Finally, to provide a clear picture of the research problem, we integrated the findings of both qualitative and quantitative phases during the discussion of the results of the whole study in the interpretation stage of the study.
Results
Quantitative phase
Socio-demographic characteristics
A total of 462 patients participated in the study, giving a response rate of 97.50%. The mean age of the respondents was 33.85 ± 11.04 years and 99 (21.40%) patients fall within the age range of 25 to 29 years. Nearly half 236 (51.10%) of the participants were from rural areas and the majority 359 (77.70%) were married. Furthermore, 145 (31.40%) and 140 (30.30%) participants attended primary education and had no formal education respectively (Table 1).
Socio-demographic characteristics of adult patients admitted to AMGH, Southern Ethiopia, 2020.
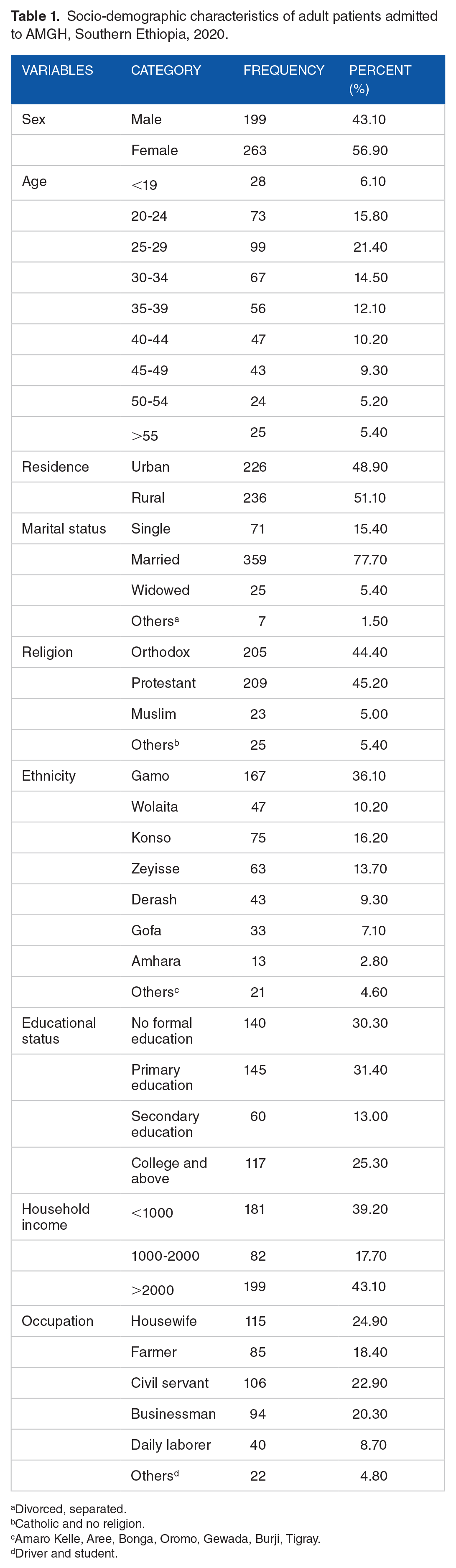
Divorced, separated.
Catholic and no religion.
Amaro Kelle, Aree, Bonga, Oromo, Gewada, Burji, Tigray.
Driver and student.
Participant’s clinical and non-clinical characteristics
About 271 (58.70%) participants were admitted to the hospital for the first time and 134 (29.00%) were admitted due to obstetrics and gynecological cases, followed by injury and poisoning cases 60 (13.00%). About 387 (83.80%) patients reported that their illness was improved since admission and nearly three-quarters (72.50%) of them used the hospital meal service. About 47% (217) of participants waited for <30 minutes for admission. In addition, 250 (54.10%) and 364 (78.80%) patients reported that they were visited 4 to 6 and 1 to 2 times per day by nurses and physicians respectively (Table 2).
Clinical and non-clinical characteristics of adult patients admitted to AMGH, Southern Ethiopia, 2020.

Endocrine, neurological, and oncologic cases.
Patient satisfaction with inpatient service
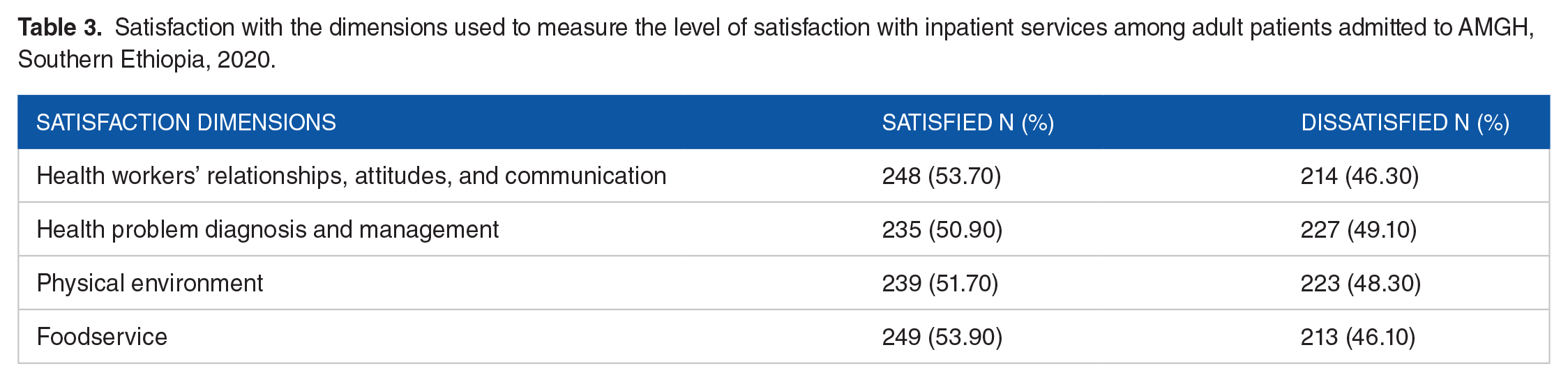
The overall satisfaction with inpatient service among the study participants was 43.70% (95% CI [39.00, 48.00]). Analysis of 4 dimensions used to measure satisfaction showed that 248 (53.70%), and 235 (50.90%), were satisfied with health workers’ relationships, attitude and communication, and health problem diagnosis and management respectively (Table 3).
Satisfaction with the dimensions used to measure the level of satisfaction with inpatient services among adult patients admitted to AMGH, Southern Ethiopia, 2020.
The result of Chi-square test showed that sex, educational status, meal service, and treatment fee were associated with patient satisfaction (Table 4).
Cross-tabulation and Chi-square (χ2) test results for the association between independent variables and satisfaction with inpatient care services among adult patients admitted to AMGH, Southern Ethiopia, 2020.

Factors affecting patient satisfaction with inpatient services
The multivariable logistic regression analysis was done for variables such as sex, age, residence, marital status, religion, ethnicity, educational status, household income, occupation, frequency of hospitalization, meal service, duration of hospitalization, time of hospitalization, treatment outcome, admission mode, treatment fee, number of nurses visit and number of physicians visit that have a P-value <.25 in bivariable logistic regression analysis.
The multivariable logistic regression analysis showed that the odds of satisfaction were 0.67 higher among patients from urban residences (AOR 1.67; 95% CI [1.00, 2.80]) compared to those from rural areas. Similarly, patients with no formal education (AOR 3.41; 95% CI [1.21, 9.64]) had an increased likelihood of being satisfied than those who had formal education. Patients with improved treatment outcomes (AOR 2.28; 95% CI [1.65, 4.32]) were more likely to be satisfied compared to their reference group. Moreover, an adjusted analysis identified the use of hospital meal service (AOR 0.51; 95% CI [0.30, 0.85]) and duration of hospitalization (AOR 1.98; 95% CI [1.18, 2.06]) as the factors affecting patient satisfaction (Table 5).
Bivariable and multivariable regression of satisfaction with inpatient services among adult patients admitted to AMGH, Southern Ethiopia, 2020.

Significant at P-value <.05 in multivariable logistic regression analysis. Hosmer and Lemeshow model fitness test (P = .48).
Qualitative phase
Participants’ description
Eight participants were interviewed in depth. Among them, 4 were males and 4 were females. Participants were selected from all adult admission units of the hospital. The minimum and maximum age of the participants was 28 and 58 respectively. Furthermore, the study participant’s lowest duration of hospital stay was 1 week, while 2 months was the longest duration of hospital stay.
The findings of the in-depth interviews were discussed in 5 themes—Residence, Educational status, the status of health, Hospital food service, and duration of the hospital stay.
Residence
Participants from rural and urban areas raised their concerns regarding their satisfaction with the services they received at the hospital. Thus, for instance, a 36-year-old male patient from the urban area expressed his satisfaction with hospital inpatient service as follows:
“. . .As far as I am concerned, I have no words to describe how happy I am with the service I have received at this hospital. Having grown up in this town, I am familiar with most health professionals, so if I need them, I call them and they respond promptly to me. Moreover, my family members and neighbors have been visiting and comforting me every morning and evening since the accident. Even the way the hospital staff provides service is improving from time to time as I compare it with what I have experienced before. . .” [From the medical ward]
Conversely, participants from rural areas expressed their dissatisfaction with the service given to them in the admission units of the hospital. Participants complained highly about the absence of a support system for patients from the rural communities served by the hospital.
“Generally, I am less satisfied with the inpatient services provided in this hospital. This is because the hospital has no means of supporting patients who come from rural areas. Patients and their attendants spent a lot of money. And you know that rural communities in our country are poor as a whole. So having this in mind how can I say I am satisfied with the services I was provided with? [A 58-year-old female from the obstetrics and gynecology ward]
Education status
This is a theme under which patients with different educational statuses expressed their satisfaction with the service delivered to them at inpatient units. Accordingly, a 39 years old female civil servant from the obstetrics and gynecology ward outlined her suggestion as follows:
“. . .To speak frankly, I am not satisfied with the service I received during my stay in this hospital. That is because, even if the hospital posted patients' rights and responsibilities in the compound, its workers could not provide services that way. For example, once upon a time, I feel severe pain in my stomach and called one health professional to see and gave me medication, but she said “my working hour was over, the other nurse who will care for you is coming, wait for some minutes”. That is disappointing. . .”
Another 48-year-old female high school teacher from the Eye ward stated:
“. . .I am afraid to say I am satisfied with the service I receive during admission to this hospital. To begin with, in the card room, the staff does not speak loud enough and gets angry when talking to us. In addition, we buy most of the drugs at a high price from private pharmacies. Furthermore, the bed sheets are not changed regularly, and the health professionals do not come to us as quickly as we need them. Thus, having experienced such problems, I find it difficult to say I am satisfied with the service I got in this hospital.”
However, participants with no formal education were satisfied with the service they received from their admission units. The participants expressed their satisfaction, particularly with how the hospital’s health professionals communicated with them and diagnosed and handled their health problems as fantastic.
For example, A 42-year-old male participant from the surgical ward stated:-
“I want to thank the staff of the hospital. While there was a language barrier between us when I came here with electric burns, I was treated with compassion from the entrance to the emergency room. The staff provided food, changed my bed sheets daily, and gave me medication on time. Overall, even if some people were worried about the service delivered to patients admitted to this hospital, I am personally very pleased with the service I got here as I compare it to service I got from a health center found near our community.”
Status of health
In the interview, participants also shared their opinions on the quality of service they received from hospital in-patient services. Participants that feel their health status was improved have expressed their praise to health professionals at the hospital.
“. . .I am very satisfied because as I mentioned in the beginning, I was not aware of myself when I came here, but now my health condition has improved dramatically. So I would like to praise the Lord who gave this knowledge and skill to those health professionals. Moreover, I would like to express my sincere gratitude to the staff of this hospital.” [A 50-year-old male patient from the medical ward]
On the contrary, participants who reported their health status was not improved much following discharge expressed concern about the care they received in the hospital’s inpatient units. In addition, participants who did not get proper care, diagnosis, or treatment for their health problems were disappointed with the in-patient services provided in the hospital.
“. . .They order you to buy medication and then disappear. As well, unless you call them, the ward nurses do not come to us and ask us about our health problems. Although I did not recover from my illness, the doctors told me to go home, so I accepted their decision and was discharged. This is because I think it is better to be at home and recover from the illness there than simply staying in the ward without proper treatment and follow-up.” [A 39-year-old female from the obstetrics and gynecology ward]
Hospital food service
This is a theme under which participants shared their concerns regarding the meal served to patients admitted to the hospital. Participants expressed their dissatisfaction with the hospital’s meal service as expensive, poor in quality, and not considering patients’ health status.
“. . .Their food was poor in quality and expensive when I compare it with that bought for me outside of the hospital. So as the hospital is a place where patients with different kinds of health problems are treated, it should serve food that improves the patients’ recovery from illness. However, the food served by the hospital is not prepared in this manner. For that reason, I stopped using hospital-provided food and bought it from outside the hospital. Moreover, I would like to recommend that hospital administrators should work on improving the food quality and costs.” [A 38-year-old male from the surgical ward]
On the other hand, some participants highlighted the pleasing service provided in the inpatient units, even though they did not use the meals provided by the hospital. Accordingly, a 28 years old female patient from the obstetrics and gynecology ward stated:
“. . .As I am from this town, I am eating the food brought for me from home, but I thought the meal served by the hospital was also tasty. The reason is that many patients in my room had been using the food, and I did not hear any complaints or concerns regarding its quality or adequacy. Apart from toilet and ward hygiene concerns, almost every aspect of the services I received in this hospital inpatient unit was excellent.”
Duration of hospital stay
Participants who were hospitalized for more than 72 hours and whose treatment was postponed expressed dissatisfaction with the service provided in the hospital’s inpatient unit.
For instance, a 42-year-old male patient who stayed for 2 months in the surgical ward highlighted that:
“. . .Eh, in the beginning, especially during the admission process, I was pleased with the service I received, but later, the doctor informed me that my burn wound would require skin to be removed from other parts of my body, and he ordered medications to be bought. After that, my brother bought the medications and told the nurses. However, after repeatedly saying that “there is a shortage of some medicines in the operating room,” they took the skin from my right thigh and sutured it to the burn wound after I began experiencing financial hardship approximately two weeks after the doctor told me about it. And that is the most disappointing situation I ever encountered. . .”
The study found that participants who stayed in the inpatient unit of the hospital for a short time appreciated the service it provided. They appreciated that the hospital staff took the time to understand their health problem and handled it well. Furthermore, participants valued the health professionals’ cooperation and follow-up that they made for them in their ward.
“. . .I just have no words to describe the kindness and compassion of the doctors as they try to understand the patient’s problems. Before I transferred to my admission unit, much blood was lost from my body. When I reached the emergency room, all the health staff immediately worked together and began to resuscitate me urgently. Following my transfer to the admission unit, health professionals working in that room were also regularly monitoring my health condition and following me. So overall I am very happy and pleased with the service provided to me in this hospital” [A 36-years-old male from the medical ward]
Discussion
This study examined factors affecting satisfaction with inpatient care service among adult patients admitted to AMGH and followed up with a qualitative study using in-depth interviews to elaborate and explore why certain variables were statistically related to the outcome variable or not.
The current study showed that the overall satisfaction among study participants was 43.70% (95% CI [39.00, 48.00]). The finding is almost similar to a study conducted in Southeast Nigeria, which reported that the level of satisfaction among admitted patients was 47.30%. 37 However, our finding was lower compared to the studies in Jimma 62.0% 13 and Mekelle 80.00%, 15 Ethiopia. This finding was also lower than the satisfaction level found in Germany 80.0%, 10 India 79.0%, 38 Iran 98.0%, 9 Pakistan 82.5%, 11 and North-Central Nigeria 67.5%. 12 In addition, the finding of this study was lower than the result of 3 studies in China, which reported a satisfaction level of 76.00, 19 90.00, 14 and 58.00%. 39 This difference might be due to differences in the socio-demographic characteristics of the participants and the methods employed. In contrast, this study found higher patient satisfaction than a pooled report from Iran, which showed 14.10% 40 and a cross-sectional study conducted in China, which revealed 18.50%. 41 This disparity could be due to differences in the organization of the hospitals and the tool used to measure satisfaction.
This study also found that socio-demographic and patient clinical and non-clinical characteristics were significantly associated with patient satisfaction. Quantitatively, participants from urban areas were 1.67 times more likely to be satisfied compared to those from rural residences. Likewise, the rural participants of the qualitative phase also expressed their dissatisfaction with the inpatient services of the hospital. They linked this to financial challenges and a lack of support systems in the hospital. The findings were consistent with the result of a study in Zambia, which reported a 53.00% increased likelihood of satisfaction among patients from urban residences. 42
However, this finding was not in agreement with the studies in North-central Nigeria, 12 Mekelle, 15 and Jimma, Ethiopia 13 which reported higher odds of satisfaction among patients from rural areas. The variation could be due to differences in the population included in the studies. For instance, the study in Mekelle was limited to the obstetrics and gynecological ward. In addition, the disparity could be explained by the fact that most of the patients in our study were from rural catchment areas. Moreover, participants from rural areas are far from their homes and spent money on transport, medications, and attendant food. So they will have financial problems and become less satisfied. In contrast, patients from an urban area may have high access to and use health information and are familiar with urban life compared to patients from rural areas.
Statistically, the present study found that patients with no formal education were 3.41 times more likely to be satisfied compared to those who attended college and above. Qualitatively, the analysis revealed that participants with no formal education were satisfied with the inpatient service they received at the study hospital. However, participants with formal education (college and above) expressed their disappointment with the service provided to them by relating it to the prompt response of health professionals, the availability of drugs, and information posted in the hospital compound. The findings were consistent with the studies done in Haryana, India, 40 Jimma, Ethiopia, 13 Surakarta, Indonesia, 18 North-Central Nigeria, 12 and Pakistan. 43
On the other hand, this finding is not in line with the study at Gandhi Memorial Hospital, Ethiopia, which reported higher odds of satisfaction among participants with secondary-level education. 44 This variation could be due to differences in the study population and the hospital setting. Additionally, they might be less satisfied if they do not receive services that are comparable to the information they received previously or fall below their expectations.
Quantitatively, participants with improved treatment outcomes were 2.28 times more likely to be satisfied. Qualitative analysis of results showed that participants who felt their health status improved much since admission praised and thanked the staff of the ward, whereas participants who reported their health status was not improved much were dissatisfied with the service they got and complained about regular follow-up visits. These findings are in agreement with the study in Germany 9 and Pakistan, 43 which found a positive association between treatment outcome and satisfaction. Perhaps this might be because as the health condition of the patient improves, the patient becomes more pleased and satisfied with the service offered. Moreover, as well as recommending regular visits to patients in their wards, the qualitative phase findings highlighted the importance of contacting patients about their health status regularly.
Statistically, patients who used the hospital meal service had 49.00% lesser odds of being satisfied compared to those who did not use this service. Further, the qualitative result revealed that consumers of the hospital meal service voiced their dissatisfaction with hospital health service delivery. They expressed their concern with the quality of the hospital meal service as poor, expensive, and not considered patients’ needs. Moreover, participants who did not use hospital meals expressed satisfaction with inpatient services, however, they emphasized hygienic concerns regarding the ward and toilet rooms. This finding was similar to the result of the study done by Dall’ Oglio et al. 45 Additionally, the qualitative findings highlight the significance of providing patient-focused and quality food and working to ensure hygiene in a hospital environment to improve patient satisfaction.
Quantitatively, patients with an admission duration of 1 to 3 days were 1.98 times more likely to be satisfied than their reference group. The qualitative result also revealed that patients who stayed for more than 7 days were dissatisfied with the service. This finding was in agreement with the study done in Mekelle, Ethiopia. 15 The possible explanation for this finding might be related to the fact that as hospital stays are prolonged, expenses for medications, bed, food, and other essential needs increases. Due to this, patients might face financial problems and are thus likely to be dissatisfied. On the contrary, the finding was inconsistent with the study in Addis Ababa 44 and Indonesia, 18 which reported an increased likelihood of satisfaction as the duration of hospitalization increased. This discrepancy could be due to differences in the study population and sampling technique. For instance, the study in Indonesia was done on a small number of patients and used stratified simple random sampling.
Strengths and Limitations
The mixed method approach used for this study will provide valuable information to healthcare managers and other stakeholders to get deep insight into factors affecting adult patient satisfaction with inpatient services. Moreover, since the participants of this study were chosen in the hospital setting during discharge, the probability of recall bias could be minimized.
Since data collection was done in the hospital, the participants might have provided the information supporting the hospital staff due to frustration which could result in social desirability bias. However, we thought that this could not have a significant impact as necessary explanations were given and the data collection and record process were held in a quiet room. Fatigue associated with their illness and hospitalization could also influence participants’ responses. Moreover, variations in patients’ hospital stays might have an impact on patients’ satisfaction with inpatient services. But, since the quantitative data were collected from a relatively adequate sample of the patients and the in-depth interviews were stopped after data were saturated, the results are unlikely to be affected by this feature. In addition, since the study was conducted in a single hospital, the generalizability and/or transferability of the findings might be limited to the study setting.
Conclusions
The overall satisfaction with inpatient services in this study was relatively low. Rural residence, educational status, treatment outcome, use of hospital meal service, and duration of admission were significantly associated with patient satisfaction. Therefore, health professionals should make an appropriate diagnosis of illness, provide proper and timely treatment and care, and do regular follow-up visits to improve treatment outcomes and duration of hospitalization. Besides, the hospital administration should improve the quality of meal service and minimize its cost.
Footnotes
Acknowledgements
The authors would like to thank Mekelle University, study participants, and data collectors for their contributions to the success of this work.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request. All co-authors gave full responsibility to the corresponding author to share and discuss with editors and reviewers.
Ethical Approval and Consent to Participate
This study was approved by Mekelle University, College of Health Sciences, Institutional Review Board dated January 21, 2020, and numbered ERC1573/2020. An official letter was also received from the administration of AMGH and written informed consent was obtained from the participants. Confidentiality of the information was maintained throughout the study.