
Abstract
Evaluation of patient perceptions of quality and adequacy of care is a critical component of continuous improvement in chronic disease care. The purpose of this study was to ascertain how patients with non-communicable diseases (NCDs) assess their routine care in primary care centres in Saudi Arabia and to identify areas for improvement. This cross-sectional study used the PACIC questionnaire to assess the quality of care received by these patients in primary care centres in Saudi Arabia. Data collection took place between May 2019 and July 2019. The questionnaire was self-completed anonymously by 315 patients with NCD attending primary health care centres in Riyadh, Saudi Arabia. The results showed that the average overall PACIC score was 2.97 (SD = 0.65), the mean scores for the subscales ranged from 2.76 (SD = 0.78) for the subscale of goal settings/tailoring to 3.17 (SD = 0.78) for delivery system design/decision support. PACIC scores varied significantly with age, occupation, monthly income, type and duration of chronic illness and educational attainment. In conclusion, patients with NCDs prioritised improvements in organised care that; is comprehensive, focussed on their needs, helps them identify clear goals for their treatments and become more involved in their condition(s) management.
Keywords
Background
The growing prevalence of non-communicable chronic diseases (NCDs) is placing increased pressure on healthcare systems, particularly primary health care. Worldwide, diabetes, respiratory disease, cardiovascular diseases and cancer account for over 80% of all deaths from NCDs. 1 In Saudi Arabia, NCDs are responsible for 73% of all deaths. 2 Many patients with NCDs do not receive treatment that meets their needs, even in well-managed integrated delivery systems. Consequently, as evidence exists that proactive, structured, and patient-centred approaches improve health outcomes for patients with NCDs, health care reforms have focussed on system changes to deliver this. The chronic care model (CCM) is an evidence-based framework widely accepted for improving the care of patients with NCDs. 3 CCM was introduced to bridge the gap between evidence-based chronic disease care and actual care practices. 4 A central component of the CCM is the team-centred care approach, which is intended to improve the processes and outcomes of NCD care by facilitating effective interactions between proactive primary care practice teams and informed patients.3,5,6
The CCM identifies a set of 6 clinical practice elements designed to deliver high-quality care to patients with NCDs: decision support, delivery system design, provision of clinical information systems, self-management support, the use of community resources and improved health care organisation. Interventions that involve one or more of the key elements of the CCM have been shown to positively impact care processes and clinical outcomes in patients with NCDs.7-9 CCM-concordant care is regarded as a reliable indication of quality. 10 As CCM is patient-centred, it is critical to include patients’ perspectives on the quality of the provided care. Hence, Glasgow et al 11 developed the patient assessment of chronic illness care (PACIC) questionnaire for the assessment of patients’ perspectives on the alignment of primary care with the CCM measurement of care. PACIC was selected for this study because it allows for a standardised assessment of the patient’s perspective on the current quality of health care services, which is essential in the evaluation of chronic care management.12-14 The PACIC questionnaire has been validated and used in the Saudi context.15,16
The PACIC can be used by health care organisations to support overall quality improvement efforts and track delivery of self-management support for patients.17-19 The key elements of the CCM have been included in NCD management programmes in different healthcare organisations in different countries, such as Australia, Canada, England and the United States. 20 In Saudi Arabia, the implementation of CCM in the routine care of patients with NCDs at primary health care centres is not well researched. Thus, the purpose of this study was to ascertain how patients with NCDs assess their routine chronic care received in primary care centres in Saudi Arabia and determine changes needed to the Saudi healthcare system to improve the quality of care for patients with NCDs.
Material and Methods
Study settings and design
This cross-sectional study used the PACIC questionnaire to assess the quality of care received by patient with NCD in primary care centres in Riyadh, Saudi Arabia. Data collection took place between May 2019 and July 2019 with the questionnaire completed anonymously by 315 patients with patients with NCDs attending primary health care centres on study days.
Sample size
For an estimated patient population of 20 000 the sample size for estimates of PACIC scores with a 5% margin of error at 95% confidence level, was 377 (calculated using Raosoft calculator) 21 simplified as a target of 400. The sample size achieved was 315 due to incomplete questionnaires giving an effective response rate of 79%. This sample size is similar to that used to develop and validate the PACIC instrument. 11
Research instrument
PACIC was selected because it allows for a standardised assessment of the patient’s perspective on the current quality of health care services. In addition, the questionnaire included socio-demographic variables of age, sex, income, occupation and level of educational attainment as they are known to influence health outcomes and important determinant of access to healthcare services. The PACIC questions group into the 5-factorial domains that assess the extent to which patients report receiving care that is consistent with the CCM as proposed by Glasgow et al. 11 The achievement level of each of these items is rated by the patients on a 5-point scale: 1 = almost never, 2 = generally not, 3 = sometimes, 4 = most of the time, and 5 = almost always. A high score indicates a high level of patient involvement.
The inclusion criteria were patients with one or more diagnoses of a chronic disease and at least 1 visit to the primary healthcare centre within the 6 months prior to data collection. The exclusion criteria included an insufficient ability to participate in a survey (eg, not being able to read or write, blindness, deafness) and inability to give consent. All participants needed to sign an informed consent form prior to filling out the questionnaire.
Data management and analysis
Data were processed using the Statistical Package for the Social Sciences (SPSS) Version 26.0. Multivariate analysis was done to determine the association between the total score and subsection score with the respective socio-demographic and service-related characteristics. An independent samples t-test was applied for the variables with 2 categories, while a one-way ANOVA was used for the variables with multiple categories. Statistical significance (alpha) was set at .05 for all comparisons.
Ethical considerations
This study was approved by the ethics committee of the Ministry of Health, Saudi Arabia (IRB log no: 2019-0028 E dated 02/04/2019).
Results
The final sample consisted of 315 patients with NCDs. The socio-demographic characteristics of the sample are given in Table 1. In brief, the mean age of the patients was 56 years, ranging from 29 to 85; 49.8% were male and 50.2% were female, with more than half (52.4%) belonging to the 50 to 64 age group. Graduate level education was reported by over a third (37.1%), and 44.4% reported having been diagnosed with an NCD for less than 5 years. Among the study sample, 75.6% reported having only 1 NCD, while 24.4% had more than 1 NCD. Diabetes was the most common NCD, reported by 43% of the study population, followed by hypertension in 21.4% patients. Almost 50% of the diabetes patients also had hypertension. The presence of NCDs among the patients is given in Table 1.
Sociodemographic and medical characteristics of the 315 respondents.

Table 2 presents the descriptive statistics for the 20 PACIC items. The average overall PACIC score was 2.97 (SD = 0.65), with individual items ranging from 2.19 (SD = 0.83) for item 17, ‘Encouraged to go to a specific group or class to help me cope with my chronic illness’, to 3.78 (SD = 0.90) for item 12, ‘Sure that my doctor or nurse thought about my values and my traditions when they recommended treatments to me’.
Mean scores for PACIC items a in a study population with NCDs (315).
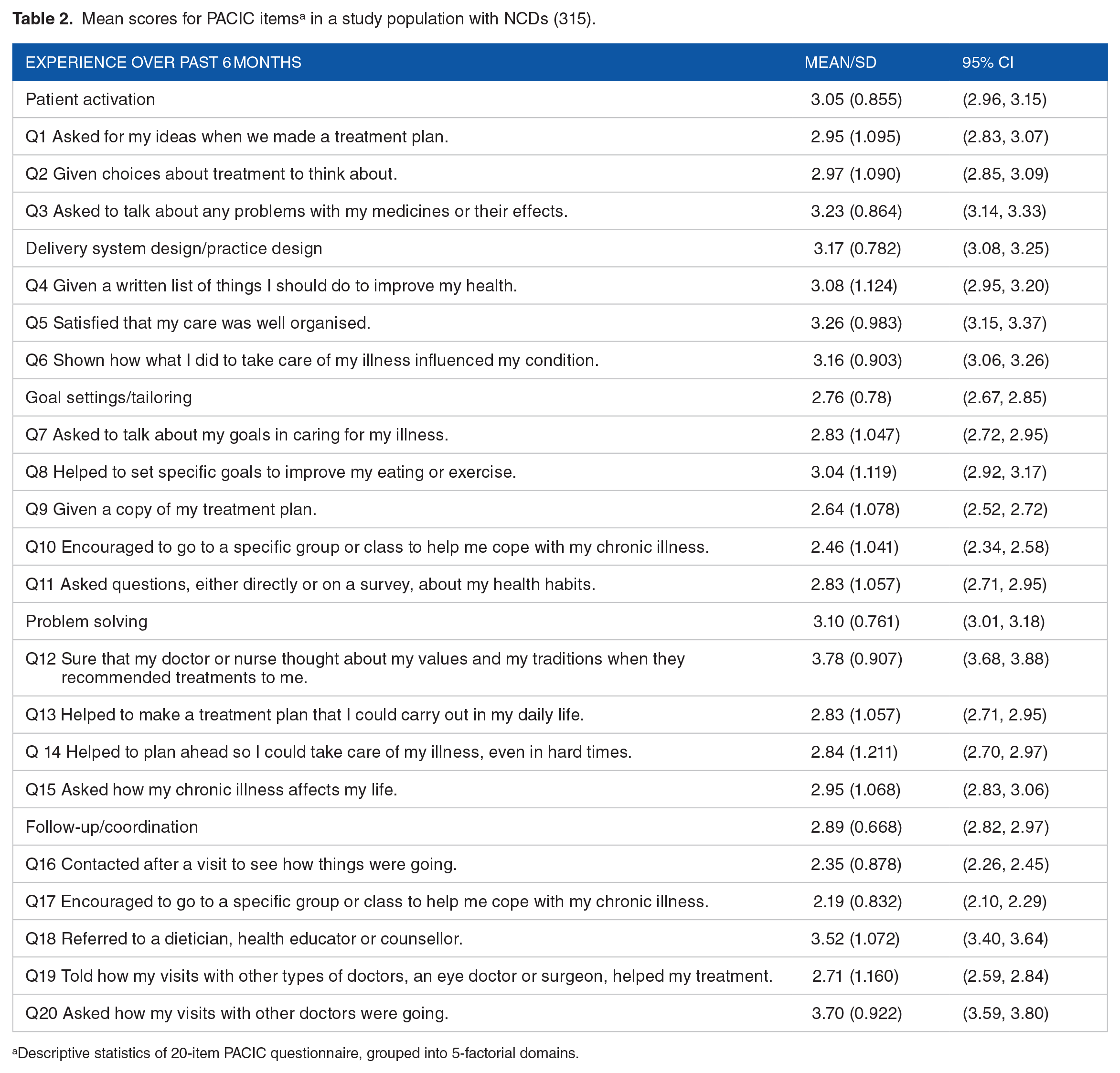
Descriptive statistics of 20-item PACIC questionnaire, grouped into 5-factorial domains.
Summary scores for the 5 domains ranged from 2.76 (SD = 0.78) for the domain of goal settings/tailoring to 3.17 (SD = 0.78) for delivery system design/decision support (Table 3). The lowest scores were for the goal settings/tailoring domain (2.76, SD = 0.78) and the follow-up/co-ordination domain (2.89, SD = 0.67).
Score distributions of the PACIC. a

Each PACIC item is scored on a 5-point Likert scale that ranges from 1 (‘almost never’) to 5 (‘almost always’), with higher scores indicating better patient-perceived quality of chronic illness care.
These analyses are based on n = 315 patients.
The relationship of the total score and domain scores with socio-demographic and service-related characteristics are shown in Table 4. The patient activation domain was significantly associated with age (P < .003), occupation (P < .018), monthly income (P < .013), type of chronic illness (P < .001) and duration of disease (P < .006). The delivery system design domain was influenced by age (P < .010), level of education (P < .002), type of chronic illness (P < .001) and duration of disease (P < .007). The goal settings/tailoring and problem-solving domains were only significantly associated with the type of chronic illness (P < .001) while the follow-up/coordination domain was significantly associated with occupation (P < .024) and type of chronic illness (P < .001). The presence of diabetes was associated with a total higher PACIC score, and patients aged 35 to 49 years were associated with higher PACIC scores.
PACIC scores according to population characteristics.

Abbreviations: ANOVA, analysis of variance; PACIC-20, Patient Assisted Chronic Illness Care; SD, standard deviation.
Data are presented as mean (SD).
Independent t test.
ANOVA.
*P less than .05 (2-tailed) is considered as statistically significant.
Discussion
Quality improvement of care requires good measurements to track changes in the standards of care and to assess the success of interventions. 22 International comparisons and benchmarking provide opportunities for health systems to learn from one another in terms of the strengths and limitations of their approaches to NCDs but requires comparable measures. Patients’ reports of care received and their perception of the quality of that care is recognised as a key element of monitoring quality of care. In this study, we utilised the PACIC scale, a standardised method for measuring patients’ perceptions, to better understand the quality of treatment for patients with NCDs attending PHC in Saudi Arabia. PACIC has been used with patient surveys in multiple different health systems23-26 and has been shown to correlate with non-patient reported based measures of quality of chronic disease care. Higher scores on PACIC and its sub-domains indicate higher patient satisfaction with their care.
The current study showed that patients with NCDs in Saudi PHC had a generally positive perception of their quality of care. The study found that patients aged 35 to 49 years were associated with higher PACIC scores, in line with findings from similar research in which younger patients had higher PACIC scores. 27 Also, in this study, diabetic patients were associated with higher PACIC scores, which is consistent with a study from the Netherlands that found patients with diabetes report higher PACIC scores with higher presence of structured chronic care. 28 This may be attributed to the more frequent involvement of patients with diabetes in organised programmes and with specific types of chronic care, such as case management. In organised programmes, care is provided in episodes or settings that focus on a single disease. While these programmes might allow for the focussed, efficient provision of care, comprehensive care for NCDs patients is more complex. The current study also found that 43% of patients suffered from diabetes, consistent with other Saudi studies. 29 Almost 50% of diabetes patients also had hypertension, consistent with the increased risk of vascular complications that decreased the patient’s quality of life in other studies.30,31
This study shows that, based on patients’ reports, the elements of effective chronic disease care are being implemented in primary care practices in Saudi Arabia. While some key elements, such as delivery system design/decision support (eg, ‘Satisfied that my care was well organised’), appear to be well implemented in routine care, patients report that other elements, such as helping the patient to set specific goals and arranging follow-ups, are less satisfactory. The mean overall PACIC score in this study was 2.97 (SD = 0.65, range 1-5) which implies that CCM-concordant care was not consistently received and patients are receiving a moderate number of services and activities. This is similar to the findings reported in Glasgow’s original PACIC validation study 11 and other studies of patients with one or more chronic illnesses.32,33 Although this score is lower than the mean scores in some US studies (3.1 in Glasgow et al 34 ; 3.2 in Jackson et al 35 ; 3.22 in Noël et al 36 ), it was higher than the mean score reported from studies in Finland (2.32 (SD = 0.84)) in Simonsen et al, 37 Germany 2.4 in Petersen et al, 38 Malaysia 2.6 in Nordin et al 39 and Egypt 2.7 in Salama and Soltan. 40 The variation in PACIC scores in different studies may be the result of differences in the samples of patients and healthcare systems. 41 The healthcare systems of these countries are not identical, and each has its own policies, delivery system and financing models which affect health system performance in terms of access to care and patients’ experiences with health care including patients with NCDs who often attend clinics with varying degrees of complexity. Furthermore, health outcomes are impacted by a broad range of social factors, economic circumstances, cultural aspects and ethnic variations which also vary among these countries.
The overall PACIC score (2.97 (SD = 0.65)) in this study appears higher than in 2 previous studies conducted in Saudi Arabi in 2015 (1.99 (SD = 1.49)) and in 2018 (2.52 (SD = 0.74)).15,42 This may represent improvements in care because these earlier studies were conducted prior to the recent efforts of the Saudi MOH to reduce the impact of chronic diseases through the implementation of a national strategy 43 that included the establishment of an electronic health records (EHR) system in all primary healthcare centres (PHCs) in 2019. 44 The availability of EHR systems was found to positively influence patients’ encounters in their PHC.
The finding that mean domain scores were lowest for goal setting/tailoring and highest for the delivery system design/decision support are consistent with results found in primary health care research conducted in some European countries, including Austria, Finland, Germany, the Netherlands, Switzerland, the United Kingdom 23 and Canada. 12 The lower PACIC domain score for ‘goal-setting’ and ‘follow-up/coordination’ in this study are consistent with a study in Malaysia. 39 These 2 domains, as well as the problem-solving domain, form the foundation of contemporary chronic care, which is always present in specialised quality improvement activities. 11 Goal settings is useful for personalising care and adapting it to a patient’s values and resources, as well as allowing patients to set attainable goals for their conditions and create concrete action plans for achieving these goals. Also, an important part of CCM is ensuring that patients receive the appropriate follow-up care with their primary care providers to monitor their health status and changes therapy where indicated. Although there have been significant efforts to improve the quality of care in primary health care in Saudi Arabia, the study results indicate there is substantial room for further improvements to increase patients’ perceptions of the quality of follow-up and coordination and goal setting/tailoring, including increasing referrals to other specialities, actively making phone calls, and providing home visits for patients with NCDs. Focussing on improving the aspects of care relating to these low score domains will allow healthcare teams to be more effective at fulfilling the patient’s needs and enhancing the patient’s satisfaction. 45 The findings of one study showed that home visits for patients with NCDs by healthcare professionals resulted in improved perceptions of follow-up and coordination. 46
While comparing and contrasting the research on the subject, it should be noted that there are 2 main versions of the PACIC scale. In our research, the PACIC scale is rated from ‘almost never’ to ‘almost always’, as in the original research, 34 and the other main version extends from ‘never’ to ‘always’. Finally, the delivery system design subscale obtained the highest mean score, indicating that patients believe that the healthcare system effectively supports them, despite the low mean scores in other subscales. Several studies have addressed the satisfaction of patients with NCDs with their treatment with the ultimate goal of improving the quality of delivered care.30,47
It is important to understand the socioeconomic factors that impact a patient’s assessment of care when evaluating findings based on the PACIC. A Cochrane review 48 reported that studies of strategies to improve health outcomes in patients with co-morbidities in primary care frequently failed to adequately consider the impact of socio-economic factors. This study found a statistical significance association between PACIC scores and the socio-demographic and economic characteristics of age, occupation, monthly income, type of chronic illness, duration of disease and education. AlMomen et al 42 also found PACIC scores to be associated with level of education in patients in Saudi Arabia. It is likely that people with higher education attainment have a better understanding of the care they received as well being more able to discuss their care with physicians. Individuals with a higher education achievement are more likely to have higher health literacy better equipping them to make appropriate health choices and to acquire, comprehend and evaluate health information that will help enhance and maintain their health. 49 It is noteworthy that almost half (48.2%) of the sample in the current study had attained post high school qualifications.
The current study’s findings of an association between PACIC scores and the age of the patient are consistent with those of the developers of the PACIC. 11 The finding of no significant association between PACIC scores and gender is consistent with the findings of some studies13,50 but not with a Canadian study 51 where PACIC scores were higher for males than females. These differences may be accounted for by differences in other socioeconomic variables among the studies but may also be attributable to differences in care quality or patients’ expectations in different healthcare systems. The fact that a patient’s characteristics impact how they rate their care raises the question of whether this represents different expectations or variations in the treatment delivered to various types of patients. Future studies on health care quality should collect data on patient rating of care received in parallel with data on care provided.
Strengths and Limitations
There is limited research on patients’ perception of chronic disease care for patients with NCDs in primary healthcare clinics in Saudi Arabia. The consideration of all chronic disease patients who receive treatment and follow up at primary healthcare clinics able to complete the questionnaire was a major strength. The method is a cross-sectional study design, so causality assumptions is a limitation when interpreting the findings. The study was limited to clinics in Riyadh and may not represent the experience of patients across Saudi Arabia.
Recommendations
This study indicates a number of areas to improve the treatment and management of patients with NCDs. Improving patient goal setting and follow-up and coordination of care are critical as they allow patients to set attainable goals for their conditions and create action plans for achieving their goals. Also, improvements in the quality of chronic disease care, particularly with a stronger emphasis on patient engagement in their care, are likely to result in improved health outcomes and better value for the Saudi health system from PHC. Future studies assessing the care of patients with NCDs should incorporate measurements of aspects of practice-level organisation and the care recorded or observed as provided to individual patients.
Conclusions
The findings of this study provide practical insights into areas for improvement in the Saudi primary health care management for patients with NCDs based on their perceptions of the care they receive rated on the PACIC standardised scale. While overall scores on the PACIC scale indicated a quality of chronic disease care comparable with many other health systems, lower scores on some domains point to areas for improvement. In particular, the ratings point to the need for additional efforts to improve patient goal setting and follow-up and coordination of care. Improvements in quality of chronic disease care, particularly with greater focus on patient engagement in their care, are likely to result in improved health outcomes and better value for the Saudi health system from PHC. Future studies evaluating NCD patient care should incorporate measurement of aspects of practice-level organisation and the care recorded or observed as provided to individual patients.
Research Ethics and Patient Consent
Ethical approval was obtained on 2019-04-02 from the ethics committee of the Ministry of Health, Saudi Arabia (IRB log no: 2019-0028 E). Ethical principles were maintained throughout the research. All methods were performed in accordance with the relevant guidelines and regulations of the Helsinki declaration. Written informed consent was obtained from patients for their anonymised, pooled and analysized information to be published in this article.
Footnotes
Author Contributions
All authors contributed to initiating the conception and design of the study. AH conducted the data, analysed the data, and drafted the initial manuscript. AW guided analysis, critically revised the manuscript and approved the final manuscript.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author [AH], upon reasonable request.