
Abstract
Introduction:
Primary care plays an integral role in modern healthcare systems. More so in a country that is currently undergoing a reform of its health system. Their remains barriers that hinder patients from seeking medical assistance from primary physicians. This study aims to examine the overall satisfaction of patients toward Primary Healthcare Centers (PHCs) in Saudi Arabia, as well as its association with potential barriers from a sample of patients who presented at the emergency department (ED) for non-urgent cases.
Methods:
This cross-sectional study sampled 403 patients from King Fahd Hospital of the University. A piloted questionnaire was utilized that included questions on sociodemographics, satisfaction of PHCs, as well as organizational, socioeconomic, access, and patient-doctor relationship barriers using a Likert-scale item response. Chi-squared and Fisher’s Exact tests were used to compare categorical variables, and multivariable logistic regression was used to assess the association between overall satisfaction and all factors and barriers.
Results:
The sample consisted of 48.1% males and 51.9% females. Only 5.2% of the patients were hospitalized. Of the total sample, 28.3% reported being always satisfied with PHC services. The most reported barriers were organizational barriers and socioeconomic barriers. The regression analysis found that being a female, highly educated, have high organizational, and patient-doctor relationship were independent predictors for low overall satisfaction with PHCs.
Conclusion:
Findings from this study should allow healthcare planners and policy makers to reduce the impact of these barriers by finding solutions that would target them. This may include strictly implementing policies such as proper implementing of triaging in EDs as well as promoting services that are being provided free of charge at these centers.
Introduction
Primary care is fundamental in all modern healthcare systems. Its importance arises from the fact that it provides a comprehensive patient-centered approach to patients, in addition to coordinating care across diverse specialties with ensuring good follow-up of patients. As a result, maintaining high-quality primary care based on patients’ needs and expectations is the pathway for strong primary care with high patient satisfaction. 1
Patient satisfaction is an established component commonly used in measuring healthcare services worldwide and is considered an indicator for healthcare quality. 2 A satisfied patient is likely to develop a good relationship with the healthcare system, thereby enhancing patient compliance, continuity of care and eventually a better overall health outcome. 3 Hence, a low satisfaction of Primary Healthcare Centers (PHCs) is problematic in its own, but it could also lead patients with non-urgent and primary conditions to seek medical assistance from Emergency Departments (EDs) rather than PHCs. 4
Several studies have examined patients’ satisfaction of PHCs in Saudi Arabia and have reported varying figures.5-7 In Majmaah, it was reported to be 82% of their total sample, 6 whilst 20% in Abha. 7 Although, these studies have only conducted frequencies and bivariate analyses and have very small sample sizes. A further study examined satisfaction in terms of 3 questions relating to the tidiness of the center, instruments at the center working properly and whether patients thought the services could be improved which were reported as 77%, 37%, and 72.5% respectively. 5
With regards to barriers preventing patients from attending PHCs, a study by Alfaqeeh et al 8 examined the factors that were affecting the access to PHCs in both urban and rural parts of the capital city of Riyadh, and found that factors pertaining to poor communication, distance of the PHC and waiting hours were the most reported. Other factors reported in other studies included cleanliness of the centers, lack of availability of preventive services, and difficulty booking appointments. 9
Saudi Arabia is in the middle of a health reform, where the focus has shifted to better allocation of resources and budgeting to PHCs to relieve the pressure off secondary and tertiary care hospitals. 10 Regrettably, it seems that Saudis only seek healthcare services when sick, which may increase their likelihood to attend EDs due to perceived seriousness of their condition. This is especially unfortunate in Saudi Arabia where health services are given free of charge. Such behaviours thwart the governmental efforts in both health promotion and prevention. 11 Therefore, this study aims at examining the overall satisfaction of PHCs as well as the barriers against attending PHCs among a sample of ED non-urgent patients in Khobar, Saudi Arabia.
Methods
Study Design and Settings
This cross-sectional study was conducted at the ED of King Fahd Hospital of the University which is one of the facilities of Imam Abdulrahman Bin Faisal University (IAU) in the Eastern province of Saudi Arabia in 2019. The study included patients aged between 18 and 60 years old and who were present at the ED between 8:00 and 15:00 which are the exact working hours of PHCs in the country. Patients with trauma and urgent care and those who had arrived at the ED through ambulatory services were excluded. Ethical approval was obtained from the Institutional Review Board committee of IAU.
Sample Size and Sampling Techniques
The minimum required sample was computed to be 384. This was assuming a 50% satisfaction rate of patients toward PHCs with a precision of 5% and at an alpha level of 0.05. A systematic sampling technique was used to select the participants, who were approached by 4 research assistants.
Data Collection Tool
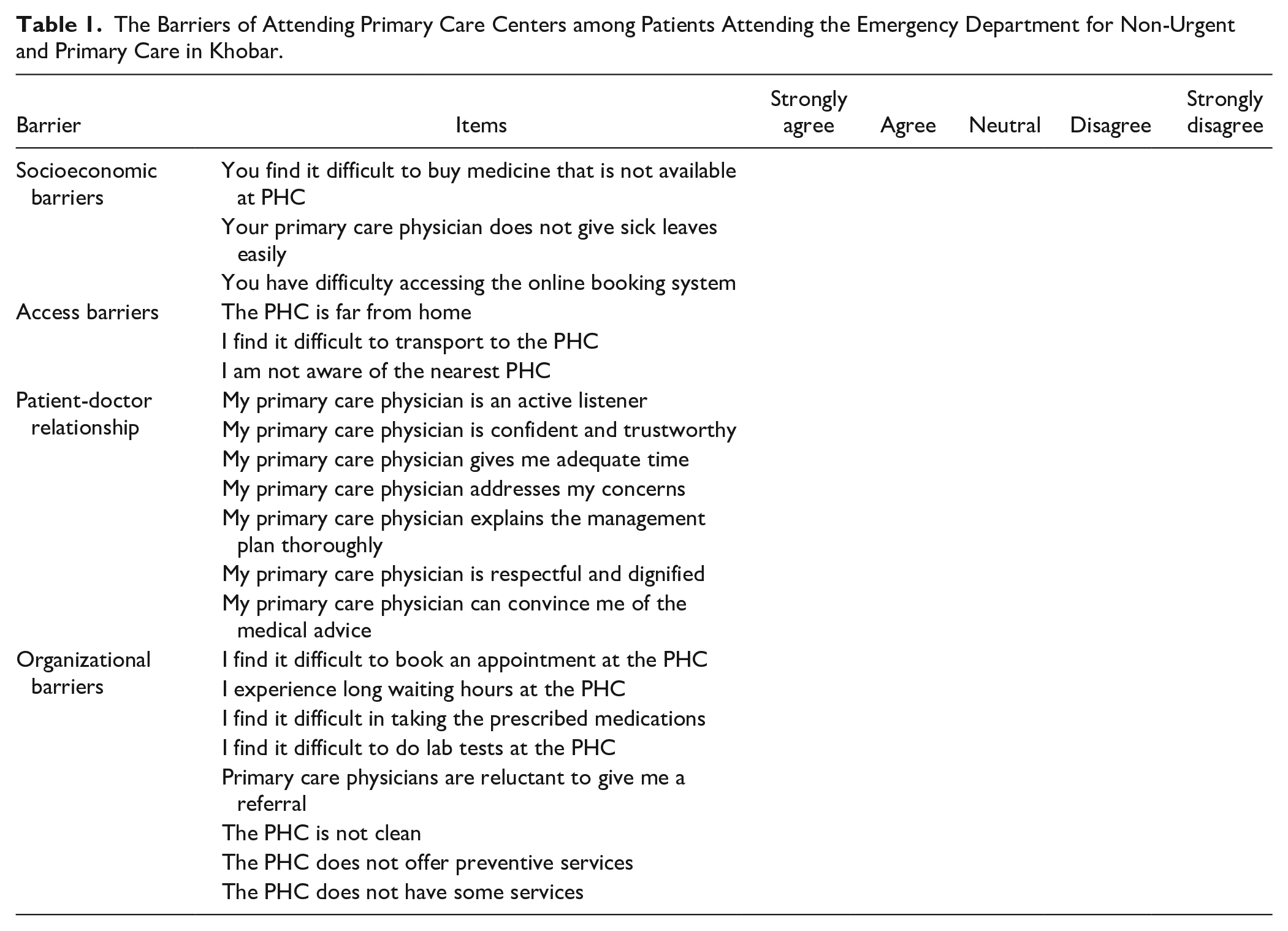
A questionnaire was developed after an extensive search of the literature. A cover letter that described the purpose of the research was attached to the questionnaire as well as the voluntary nature of participation. It consisted of 2 major sections. The first was the sociodemographic variables such as sex, age, nationality, educational status, household monthly income, marital status, and the number of family members. Patients were also asked directly to state how likely or unlikely they were satisfied with the respective PHC on a 5-point Likert-scale. The second was a series of questions relating to 4 barriers namely, socioeconomic, access, patient-doctor relationship, and organizational barriers (Table 1). A pilot study was done to ensure clarity and internal consistency. A Cronbach’s alpha value of 0.8 was obtained indicating good reliability of the questionnaire.
The Barriers of Attending Primary Care Centers among Patients Attending the Emergency Department for Non-Urgent and Primary Care in Khobar.
Statistical Analysis
After checking for completeness and consistency, data were analyzed using IBM SPSS for Windows, version 26. 12 Categorical variables, presented as percentages and frequency distributions, were compared using the chi-squared or Fisher’s exact tests. Figures were used to illustrate the responses of participants regarding the barriers to visit PHCs. In questions based on a Likert-type scale, the responses were combined into 2, so that responses of “always” or “sometimes” were coded as “yes”. The total and all barrier subscale scores were calculated as a percentage of “yes” responses after reverse coding of negatively framed questions. A high barrier score was defined as a value above the mean score. Multivariable binary logistic regression analysis was conducted to identify the independent predictors of the overall satisfaction with visiting PHCs. Candidate variables were selected based on medical literature and bivariate analyses. Odds ratio (OR) with 95% confidence interval (CI) were estimated using the full model fit and were reported in comparison with the designated reference group. The goodness-of-fit of the model was evaluated using the Omnibus and Hosmer-Lemeshow tests. The significance level was defined as α = .05.
Results
Characteristics of Participants
The survey was completed by 403 patients, including 48.1% men and 51.9% women, visiting the ED. Overall, 46.9% participants were below the age of 30 years. The majority of participants were Saudi citizens. Nearly half were married, and 43.9% had a college education. In total, 24.1% of participants had family members less than 4, compared to 27% with family members of more than 7. Regarding monthly income38.5% earned below 5000 SR whilst 11.7% earned more than 15 000 SR. Only 5.2% were admitted to the hospital following their visit to the ED (Table 2).
Characteristics of Patients Attending the Emergency Department for Non-Urgent and Primary Care in Khobar.
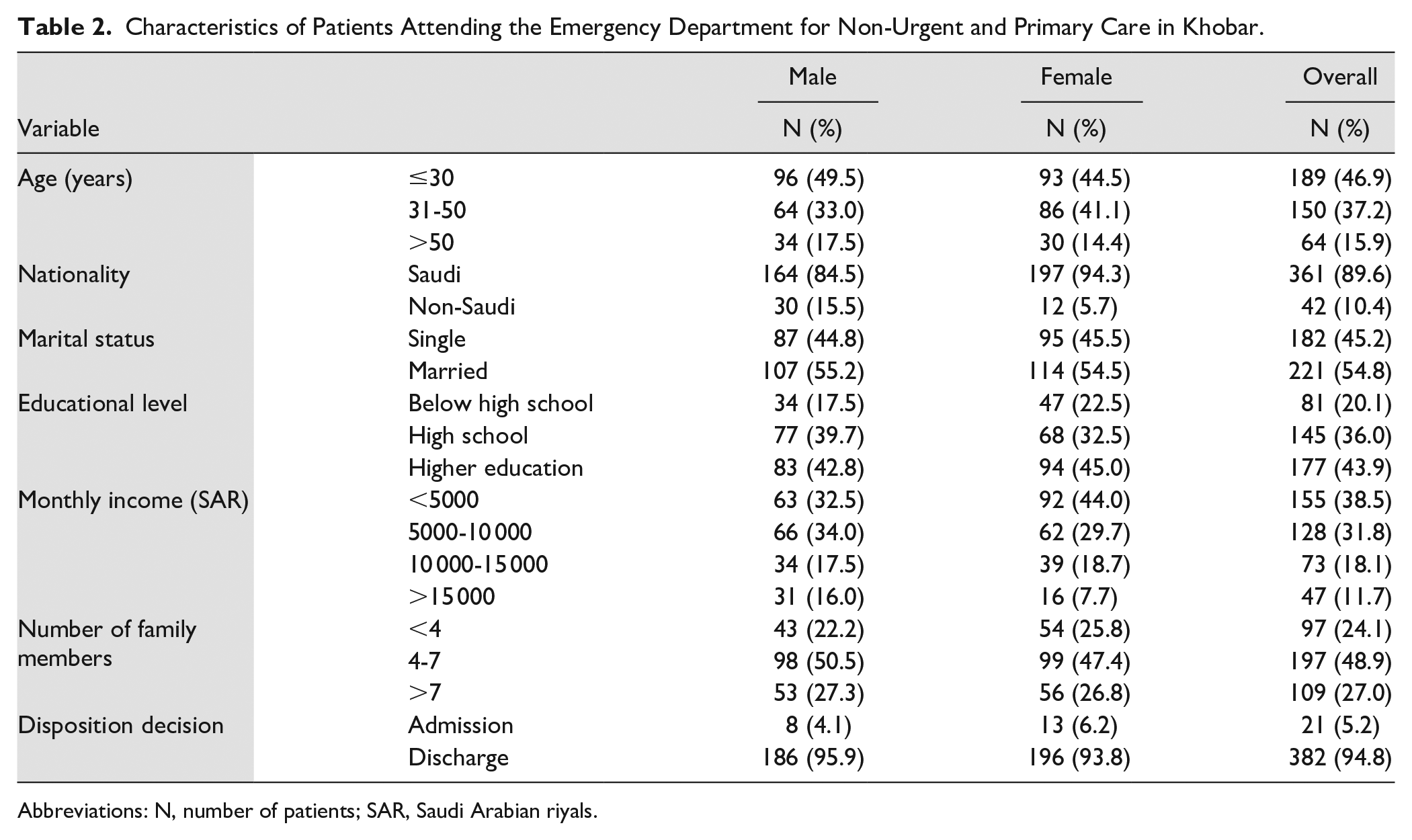
Abbreviations: N, number of patients; SAR, Saudi Arabian riyals.
Satisfaction with PHCs
In total, 28.3% of participants reported that they are always satisfied with their visits to the PHCs. In addition, only 18.8% reported that they always visit PHCs to seek medical advice. Female participants had less often overall satisfaction with their visits to PHCs than their male counterparts (23.0% vs 34.0%, P = .01). Age was significantly associated with the overall satisfaction with PHCs. For example, participants aged less than 30 years were least satisfied (24.3%) compared to those aged 31 to 50 years (27.3%), and those above the age of 50 years (47.6%) (P = .02) (Table 3).
Factors Associated with Overall Satisfaction with the Primary Health Centers among Patients Attending the Emergency Department for Non-Urgent Care in Khobar.

Abbreviations: N, number of patients; PHC: primary healthcare centers; SAR, Saudi Arabian riyal.
P values are in bold if statistically significant.
Barriers to Visit PHCs
The overall barrier score to visiting PHCs was 36.8%. The organizational factors constitute the major barrier (54.8%) followed by socioeconomic factors (47.7%). The patient-doctor relationship factors, however, were the least factors to be a barrier (10.5%) (Figure 1).

Distribution of barriers for patients to visit primary healthcare centers.
Regarding the organizational factors, long waiting hours was a leading barrier. For example, 83.4% of participants agreed or strongly agreed that they had to wait for a long time before seeing the primary healthcare physician. Similarly, 67.8% of participants reported having the same issue with the time for receiving laboratory results. Difficulty to buy medications from outside pharmacies due to their unavailability in PHCs was the most frequent socioeconomic barrier, reported by over half of the participants (53.8%) and77% reported that they are not aware of their nearest PHC (Figure 2).
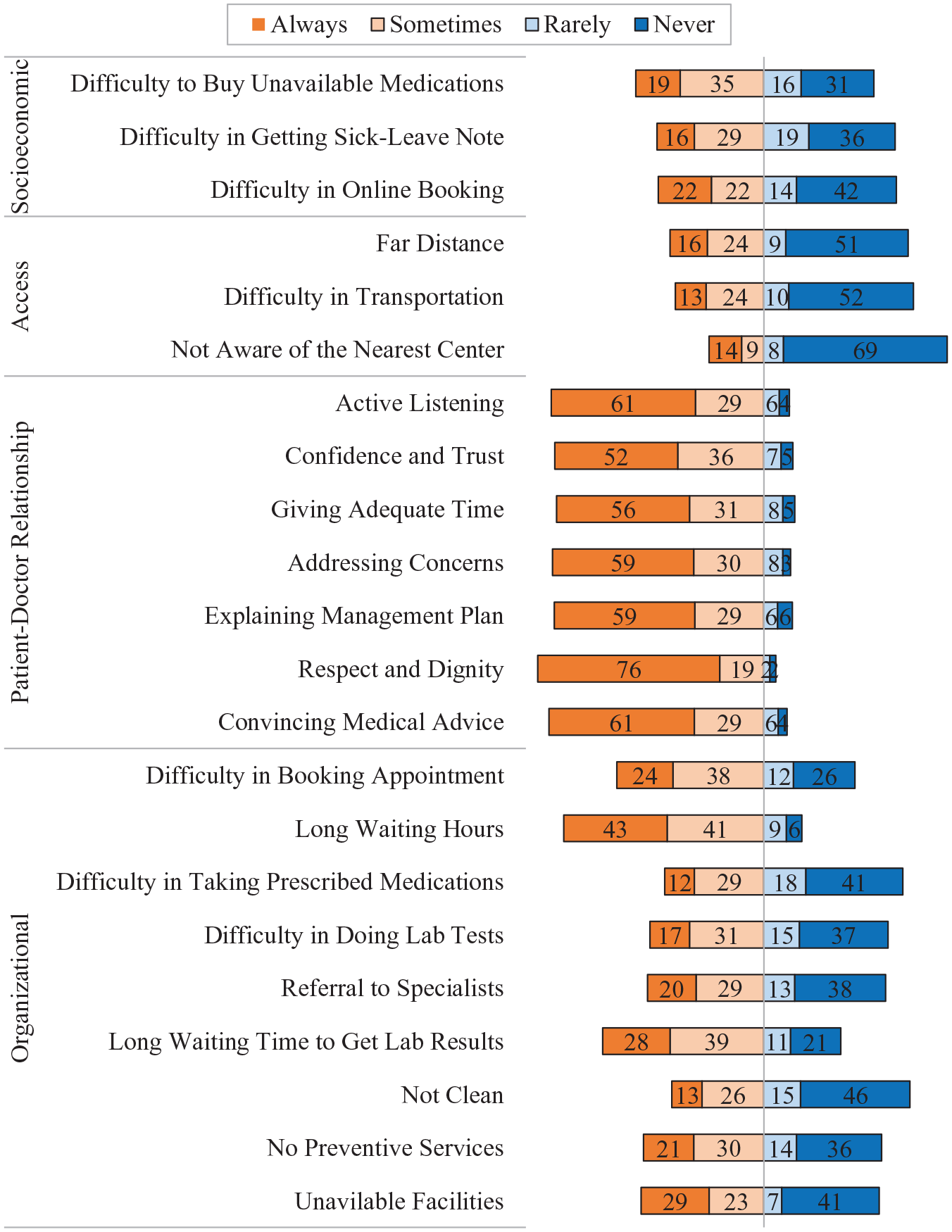
Patients responses on barriers against primary healthcare centers.
Gender and nationality were found to be the only factors that were associated with the high overall barrier score (P < 0.05), where the high score was found among 53.6% of the women compared to 34.5% of the men, and 46.3% of the Saudi’s compared to 28.6% of Non-Saudi’s (Table 4).
Factors Associated with Barriers Toward Primary Health Centers among Patients Attending the Emergency Department for Non-Urgent Care in Khobar.
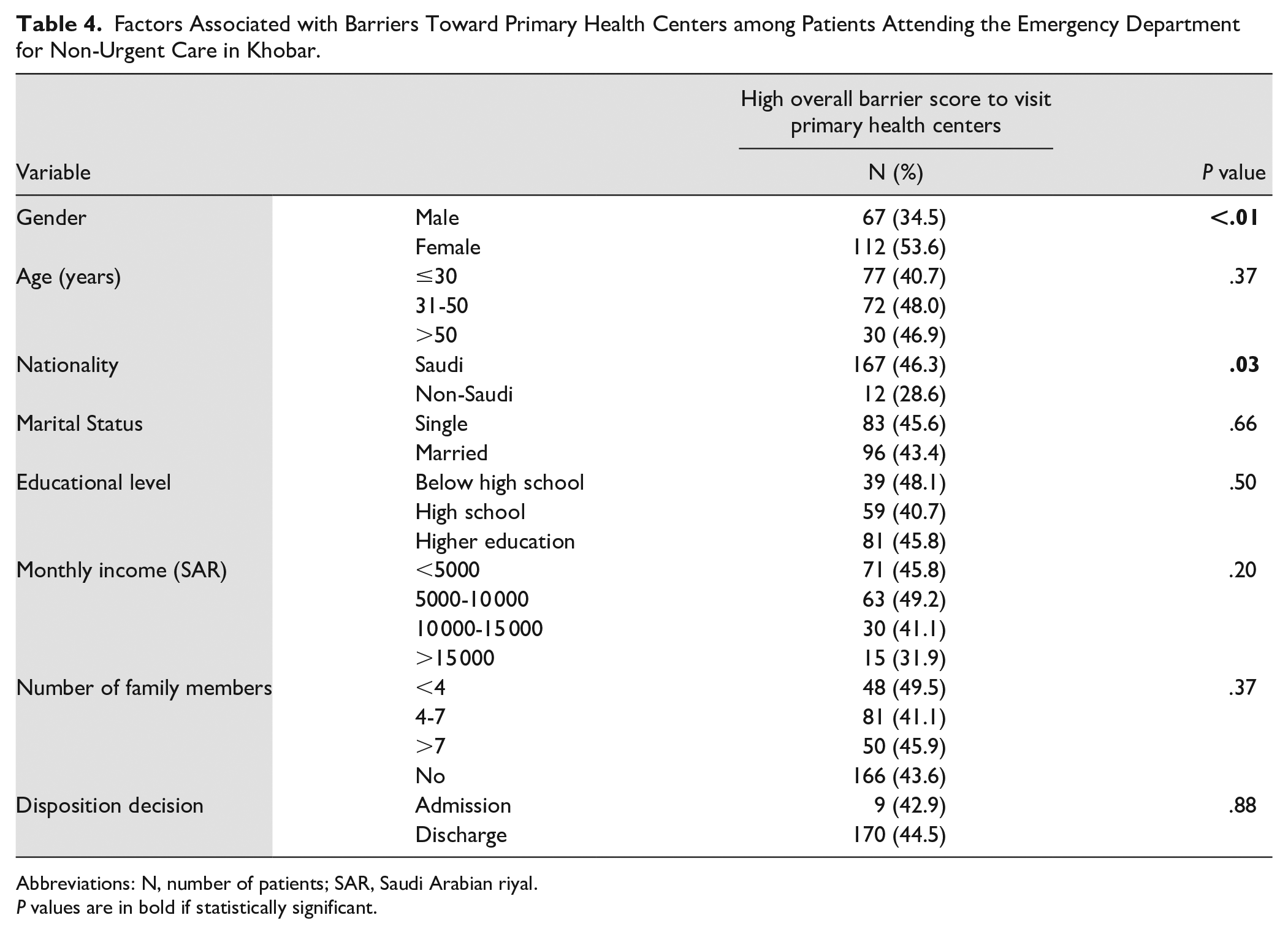
Abbreviations: N, number of patients; SAR, Saudi Arabian riyal.
P values are in bold if statistically significant.
Barrier Scores and Overall Satisfaction with PHCs
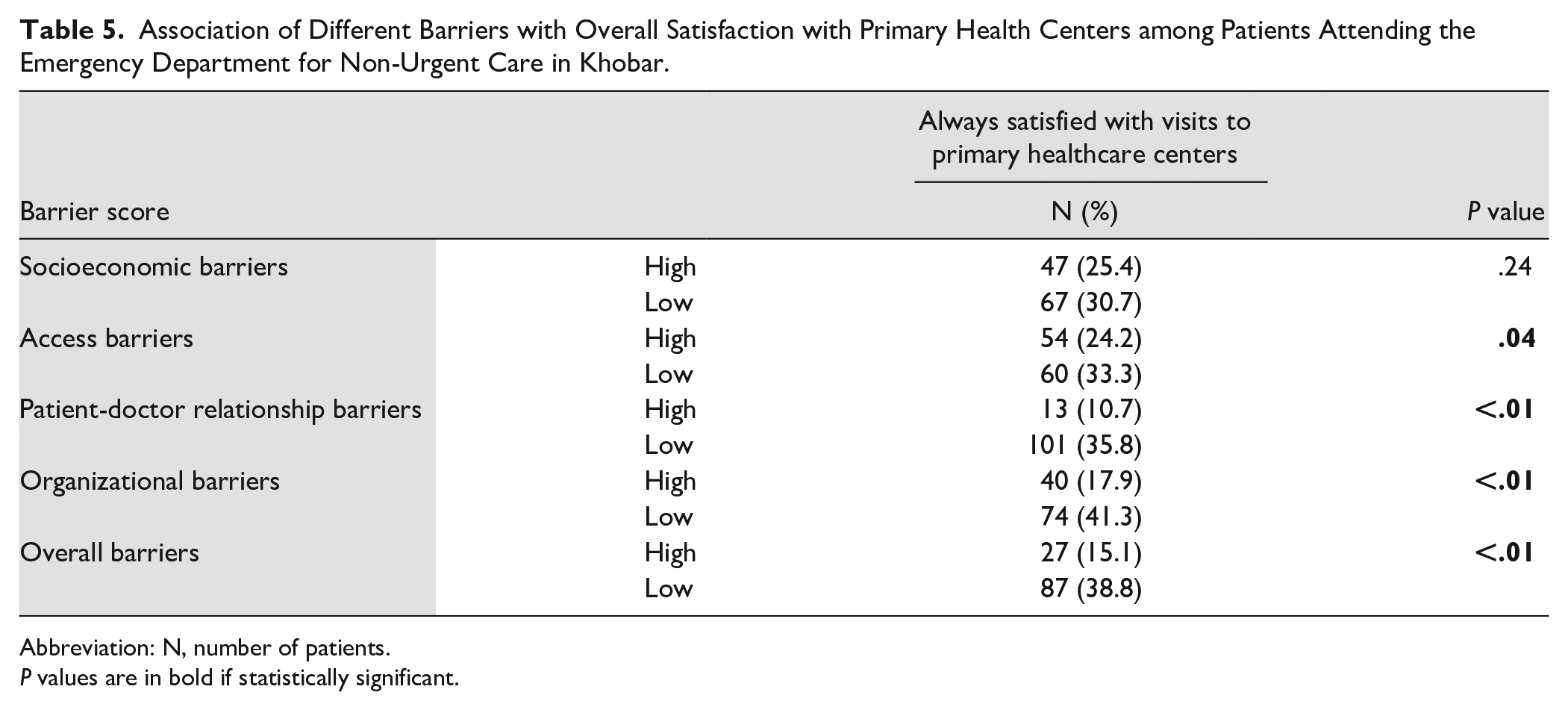
The overall barrier score was significantly associated with the satisfaction of the PHCs. For instance, participants who had a low overall barrier score had higher overall satisfaction than those who had a high barrier score (38.8% vs 15.1%, P < 0.01) (Table 5).
Association of Different Barriers with Overall Satisfaction with Primary Health Centers among Patients Attending the Emergency Department for Non-Urgent Care in Khobar.
Abbreviation: N, number of patients.
P values are in bold if statistically significant.
Multivariable Analysis of Factors Associated with Satisfaction with PHCs
Multivariable binary logistic regression analysis was performed to identify the factors associated with satisfaction with visits to the PHCs. The model revealed that those with a high-school educational level only were more likely to be satisfied with the PHCs than participants who had a higher educational level (OR = 1.77; 95% CI: 1.02-3.06). Furthermore, having a high organizational (OR = 0.42; 95% CI: 0.25-0.70) or patient-doctor relationship barrier scores (OR = 0.28; 95% CI: 0.15-0.54) were found to be independent predictors of having a lower satisfaction with PHCs (Table 6).
Multivariable Regression Analysis of Factors Associated with Overall Satisfaction with Visits to Primary Healthcare Centers among Patients Attending the Emergency Department for Non-Urgent Care in Khobar.

Abbreviations: CI, confidence interval; OR, odds ratio.
P values are in bold if statistically significant.
Discussion
The current study assessed patients’ satisfaction and their barriers to visit PHCs among a sample that visited an emergency setting in the Eastern province of Saudi Arabia.
While almost a quarter of the patients in this study reported being always satisfied with PHC visits, only 18.8% of the sample always visit PHCs to seek medical advice. This indicates that most patients were unlikely to be fully satisfied with the PHCs. 1 In Turkey, the mean patients’ satisfaction with family physician offices was reported to be 68.1%. 13 In Lebanon, it was reported that 60.23% and 36.43% of patients were satisfied and very satisfied, respectively, with the services provided in PHCs. 14 Different study settings and methodologies could explain the differences between the findings from the current study and other international and Saudi studies which revealed that patients’ satisfaction with PHCs was ranging from 75% and above. 1
A systematic review of 109 studies, published between 1980 and 2014, to discover patient satisfaction determinants, showed that the associations between patients’ characteristics and satisfaction were contradictory between studies, and directions and strengths of associations were inconsistent. 15 Age in this study was significantly associated with satisfaction of PHC visits where, the lower the age group, the less satisfied a patient is. This ultimately leads younger patients to seek primary and non-urgent care from EDs rather than PHCs. Similar findings were reported in Iran in which a patient’s age was negatively correlated with the number of ED visits. 16 Contradictory to this finding, Hemadeh et al 14 found no association between patient’s age and their satisfaction with PHC services in Lebanon. The association found in the current study may be attributed to the fact that the lower the age group, the more likely they are to not be aware of services provided by PHCs, and accordingly their expectations might not be met at a PHC.
Hemadeh et al 14 reported lower odds of satisfaction with PHC services in Lebanon among males compared to females. However, females in this study were less often satisfied with PHCs than their male counterparts. Females may have higher expectations of PHC services than men because of their responsibilities toward their children and families and consequently a better understanding of their health needs.
Educational level was observed to be a predictor of overall satisfaction. Results from this study have shown that highly educated patients were less likely to be satisfied with PHC services, either due to higher expectations surrounding the quality of care or an increased awareness and becoming more knowledgeable regarding different treatment plans. Such associations were observed in other Saudi PHCs.6,7
Interestingly, neither the monthly income nor the number of family members were associated with the overall satisfaction score. A possible contributing factor to this may that PHC services in Saudi Arabia are delivered free of charge and are entirely covered by the government.
Only 5.2% of patients in this study were admitted. Although, this finding could be attributed to the availability of well-trained ED physicians who can manage cases efficiently in EDs rather than admitting the cases. It may also be explained by the fact that most patients who visited the ED had non-urgent cases manageable effectively in PHCs, which could reflect lower satisfaction reported in this study. Alyasin and Douglas 17 conducted a study among 350 patients who visited a large tertiary ED in Riyadh, Saudi Arabia, with non-urgent presentations and found that there was a significant difference between perceptions of patients and triage nurses regarding the urgency of the cases. Other factors they found that had also influenced visits to the ED were not having a regular healthcare worker, availability of care on the same day, accessibility, and convenience to medical care. Additionally, a systematic review of 26 studies from the US revealed that the average ED visits that were non-urgent was 37% (with a range of 8%-62%). Moreover, negative perceptions of patients about alternatives such as primary care settings play an important role in driving non-urgent visits to EDs. 18 Similar findings were reported in Turkey and Iran.13,16
This study reported that organizational barriers were the most common barriers toward visiting PHCs. Organizational barriers included cleanliness, lack of preventive services and difficulty in obtaining referrals. However, long waiting hours to both see the physician and obtain lab results were the most highly reported. Similar findings were observed both nationally and internationally.19,20 For example, in Riyadh—Saudi Arabia—79.9% of patients were dissatisfied with waiting time and 44% of patients felt neutral about the availability of requested lab results.21,22 Such issues may be exacerbated by the high demands of such services due to the increasing rates of chronic diseases in recent years. 23
Socioeconomic barriers were also found to be high. It included difficulty in purchasing medications due to their non-availability at the PHC. Such an issue has been reported—although scarcely—for chronic conditions such as diabetes. 9 A further reported socioeconomic related barrier was the difficulty in obtaining an appointment through the Mawid Service, which is an electronic central appointment system provided by the Ministry of Health. 24 Some patients may lack accessibility to such electronic services which renders it easier for them to seek medical help from an ED without utilizing the Mawid system.
Interestingly, this study found that the patient-doctor relationship at PHCs was the least reported barrier. Participants mostly agreed that physicians were active listeners, confident, trustworthy, address patients’ concerns, give adequate time, explain the management plan, and show respect and dignity. Other Saudi studies reported similar findings.1,5 Therefore, this factor is less likely to impact patients’ willingness to visit the EDs.
Both the organizational barriers and patient-doctor relationship barriers were also predictors of low overall satisfaction both before and after adjustment. Indeed, older studies have found that factors pertaining to these barriers have played a role in patients resisting to present to PHCs when appropriate. However, in recent years such views are changing noticeably which reflects the efforts the government is currently working on. A primary care reform strategy has been set which calls for the establishment of more PHCs to meet the growing needs of health services especially in rural areas where potential patients tend to travel and temporarily relocate to larger cities to seek medical help rather than attending primary and preventive centers closer to their homes. 10
Strengths and Limitations
A particular strength of this study is its setting, to the best of our knowledge, past Saudi based literature has sampled patients from PHCs, whereas this study sought patients actively attending EDs for non-urgent care. It also examined both the patients’ satisfaction of PHCs as well as the barriers preventing them from attending these centers, thereby addressing the 2 issues simultaneously rather than separately as has been the case in past literature. Nevertheless, the sample size may be considered small even though it did exceed the minimal sample required. Also, the samples came from 1 ED from 1 institution which may have affected the generalizability of the results.
Conclusions
This study focused on the barriers preventing patients attending the ED at a tertiary hospital from seeking non-urgent medical care from PHCs in the Eastern province of Saudi Arabia, as well as computed an overall satisfaction score of PHCs and studied the associations between both. The most reported barriers were found to be organizational barriers which included factors such as long waiting hours and cleanliness, as well as socioeconomic barriers such as having to purchase prescribed medications that would have otherwise been available for free. Organizational barriers were found to be independent predictors of low satisfaction scores in addition to being of a younger age, a female and high educational status. Findings from this study should allow healthcare planners and policy makers to reduce the impact of these barriers by strictly implementing policies such as proper implementing of triaging in ED where non-urgent and primary cases be guided to their appropriate PHC as well as working on the reported factors for improvement.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.