
Abstract
This study aimed to assess maternal satisfaction and associated factors with delivery care services uptake among mothers who gave birth at public health centers. An institution-based cross-sectional study was conducted in the Yeka Sub-City in Addis Ababa, Ethiopia. A systematic sampling technique was used to select mothers. Bivariable and multivariable analysis was done to identify associated variables. The overall mothers’ satisfaction with delivery care services uptake was 63%. The median age of the participants was 28 years. In multivariable analysis privacy measures taken at delivery care services uptake, mothers’ education level, occupational status of mothers, and family income level of mothers were associated with mothers’ satisfaction in delivery care services. Mother’s income levels of 1501 to 5000 birr were satisfied with the service (AOR = 2.49; 95% CI: 1.3, 4.76). However, mothers whose income below1500 birr were dissatisfied. In conclusion, a mother’s educational level, occupational status, and family income affect mothers’ satisfaction with delivery care services uptake in public health centers, in the Yeka Sub-City. Evaluating health care services uptake from the client’s point of view and targeting to identify problems is very necessary.
Background
Maternal satisfaction with delivery care services is an important predictor for health care services uptake, particularly it has an influential and curial role on pregnant women’s expectation of health facilities. Globally, more than 830 women died within a day with cases related to pregnancy and childbirth problems. 1 Of these, 99% of the deaths occur in developing countries, particularly in sub-Saharan Africa nations. For instance, about 216 maternal deaths per 100 000 live births occurred in 2015. Out of these deaths more than half occurred in Africa. 2 In Ethiopia, maternal mortality is one of the most crucial problems of the country. The maternal mortalities rate of Ethiopia was 416 from 100 000 live birth and its neonatal mortality rate was 27 from 1000 newborns in 2016. 3 In fact, in Ethiopia, maternal mortality has been reduced substantially from 1067 to 416 per 100 000 births in 2000 and 2016, respectively.3,4 In addition, in Ethiopia, the skilled birth attendant coverage rate increased from 60% in 2014/2015 to 72.7% in 2015/2016.3,4
Maternal satisfaction with delivery care services has an immediate and long-term impact on health care services uptake. Furthermore, to decrease delivery-related mortality and improve maternal satisfaction with delivery care services uptake birth attendants must maintain and handle carefully every women’s labor. Because, the delivery experience of mothers has a special feeling on health facilities services and set-up.5,6 Offering a quality delivery care service increases health care service uptake. As literature indicate that the level of maternal satisfaction on delivery care services is very essential for health care services uptake by mothers. When mothers use delivery services there would be a decline in maternal morbidity and mortality.6-12 Furthermore, a comfortable physical environment, respectful care service, psychological support, and good administration set-up, cleanliness of health facilities (delivery room, hand washroom, toilet, and shower room) are important predictors and determinant factors for maternal satisfaction with delivery services. 13 Moreover, availability of essential equipment (blood pressure monitor and thermometers), laboratory services, drugs, accessibility of toilet, availability of maternal waiting room, religion, culture, and distance of health facility are very necessary factors for delivering service uptake and satisfaction.7,14-16 Therefore, the main aim of this study was to assess maternal satisfaction with delivery care services and its associated factors among mothers who gave birth at public health centers in the Yeka Sub-City, Addis Ababa, Ethiopia.
Methods
Study setting, design, and period
An institutional-based cross-sectional study was conducted at public health centers in the Yeka Sub-City from December 9, 2019 to July 8, 2020. Yeka Sub-City is located in Addis Ababa, the capital city of Ethiopia. The sub-city has 85.98 km2 areas, which is divided into 14 administrative woredas and it has a total estimated population of 465 505 in 2019. Of these, 52% were females. 17 In the Yeka Sub-City, there are 15 public health centers. As reported by the Yeka Sub-City health office 17 the expected delivery was 10 846 newborns in 2018/2019. According to the Ethiopian health tire system, each public health center is expected to provide health care services for 25 000 people. 18 However, it is believed that each health center in urban areas provides health care services for about 40 000 to 50 000 people. In addition, each public health centers provide preventive and basic curative services. Furthermore, the health centers had various units, such as delivery ward/unit, antenatal care (ANC) and postnatal follow up clinic, family planning clinic, adult outpatient department, under 5-year children clinic, youth service unit, emergency clinic, outpatient department, tuberculosis clinic, antiretroviral treatment (ART) center/clinic, HIV/AIDS screening service unit, injection and wound caring unit, vaccination unit, laboratory services, pharmacy, etc. Besides, each health center has 5 beds for inpatient services. About 85 to 142 mothers give birth monthly in each health center and around 1275 to 2130 babies are born monthly in the entire health centers. 17 In each health center, the delivery care services are managed by trained midwives. The midwives are capable to manage spontaneous vaginal deliveries and sometimes perform instrumental deliveries, for instance, forceps delivery. Mothers who had complicated labor and expected to be delivered by Cesarean section were referred to a nearby hospital. The health professionals working at the health centers are degree holders (BSc. degree) midwives, nurses, health officers, laboratory technologists, pharmacists, and diploma holder nurses, midwives, laboratory technicians, and pharmacy technicians. Sometimes, some public health centers have emergency surgeons and anesthetists.
Source and study population
The source population was all mothers who gave birth in the public health center in Yeka Sub-City, Addis Ababa, Ethiopia. Mothers who gave birth (sampled) in the selected study public health centers were included in the study. Post-natal mothers “who were mentally or critically ill during the study period were not included in the study.”
Sample size determination and sampling procedure
The sample size of this study was calculated using single population proportion formula by taking the level of maternal satisfaction at St. Paul’s Millennium Hospital (19%), in Addis Ababa to obtain the sample size at 95% certainty and a margin error of 4% and a non-response rate of 10%. The final sample size was 406. Out of 15 health centers in Yeka Sub-City, 5 public health centers were selected by using the lottery method. Then, the sample size was distributed proportionally to the selected health centers based on their number of expected deliveries. Finally, we use the systematic sampling method to obtain the required sample size.
Variables of the study
Mother’s satisfaction on delivery care service uptake was a dependent variable. The independent variables were socio-demographic characteristics, such as age, marital status, education level, income size, cleanliness of health facility, waiting for time to be seen by a health care provider, sex of service providers, maternal outcome (if mother with complication or not), obstetric history (Time of admission and wanted status of pregnancy), and cost of service and neonatal outcome (Live birth, Stillbirth, and Neonatal death).
Operational definition
The overall mother’s satisfaction was expressed as a state of being satisfied with health care service uptake in the dimension of quality-of-care service (process, outcome, and physical environment). Satisfied was measured when mothers scored 75% and above from the items of mother’s satisfaction questionnaire were categorized under “satisfied” and unsatisfied was classified when mothers scored below 75% from the items of mother’s satisfaction questionnaire, were categorized under “unsatisfied.”
Data collection tool
Data was collected using a close-ended structured questionnaire, which contains dichotomy and a 5 scale Likert scale (Very satisfied = 1, satisfied = 2, neutral = 3, dissatisfied = 4, and very dissatisfied = 5). The questionnaire has 3 parts, the first part contains socio-demographic characteristics of delivering mothers, the second part contains the obstetric history of delivering mothers and the third part contain respondents’ satisfaction on health facility process, service offered by birth attendants, cleanliness of health facility, availability of resources necessary for delivery service and birth attendants.
The questioner was primarily developed in English and then translated to the local language (Amharic) and again to English to check its consistency.
Data collection procedure
Data were collected from mothers by exit interview in the selected health centers at the time of discharge from the post-natal unit. One day of training for 5 unemployed midwife data collectors and 1 public health officer supervisor was conducted. The training was on data collecting tools, time of data collection, study participant rights, informed consent, techniques of interviewing mothers, and reorganization of the collected data. To respect the mothers’ confidentiality interview was conducted individually in a separate room. The information obtained from the study participants was kept in a locked cabinet to keep confidentiality.
Data quality assurance
To assure the data quality high emphasis was given to designing data collection instruments. Before starting the actual survey, the questionnaire was pre-tested at a nearby health center. Before data collection, a pretest was done on 20 mothers who gave birth at Mychew health center in Gullele sub-city, Addis Ababa, Ethiopia, on December 6, 2019. The pretest aimed to check its ability to capture the required data. The health centers which was used for the pre-test did not include in the study. Training was given properly for 5 data collectors. Supervision was conducted by 1 trained supervisor and the principal investigator. The collected data was checked for its completeness on daily basis to ensure the accuracy of the data. The collected data were reviewed carefully and checked for its completeness before entry into software (EPI-Info). Incomplete data were discarded. The data were entered into Epi-Info and then transferred into SPSS by the principal investigator.
Data analysis
Data were checked for completeness and coded and entered to Epi-info version 7 and exported to SPSS (Statistical Package for Social Science) version 23 for analysis. Data entry was done by the principal investigator. During data entry and analysis mother’s responses of “very satisfied” and “satisfied” were categorized as “satisfied” and the response of “neutral,” “dissatisfied” and “very dissatisfied” were categorized as “dissatisfied.” Descriptive statistics were calculated and the overall level of maternal satisfaction was determined by classifying mothers who scored 75% and above under “satisfied” and those who scored below 75% under “dissatisfied”
To identify the association of different independent variables with the outcome variable, cross-tabulations, and bivariable analysis was carried out. In addition, multivariable analysis was conducted to identify the most important predictors of maternal satisfaction. The odd ratio with 95% confidence interval and P-value less than .05 were used to determine factors independently associated with maternal satisfaction. The findings were presented in the form of text, tables, and figures.
Ethical consideration
Ethical clearance was obtained from the Ethical review committee of Addis Continental Institute of Public Health, (Ref. No. ACIPH-MPH/004//12, Dated 4 December 2019). Support letter was obtained from the Addis Ababa Health Bureau and Yeka Sub-City Health Office. Then the selected mothers were informed about the purpose of the study, the importance of their participation, their right to withdraw at any time. Data was collected after getting informed consent from mothers. Information obtained from each respondent was kept confidential.
Results
Socio-demographic characteristics
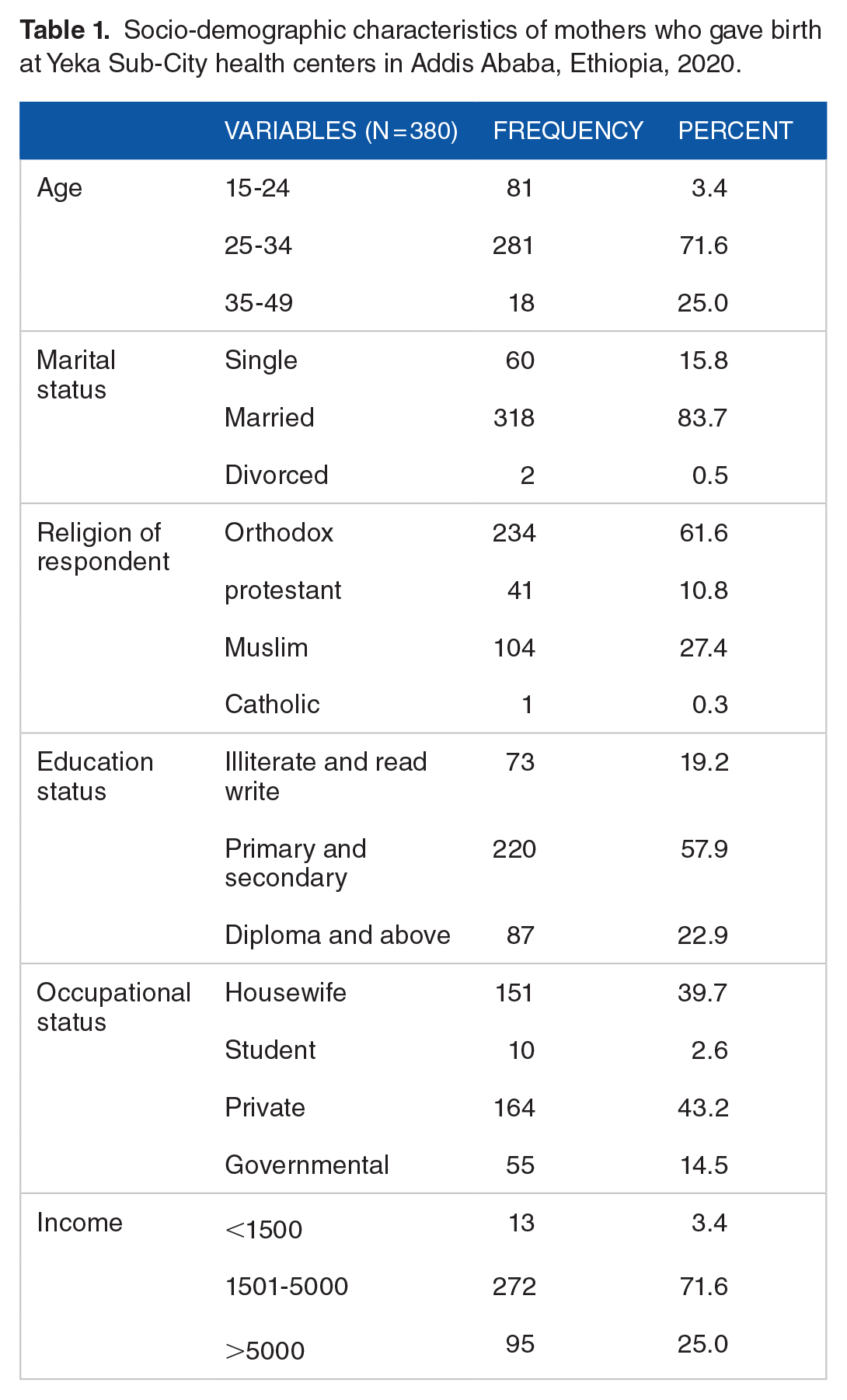
A sample of 406 mothers was selected for the study. Of these, 26 mothers discontinued the study. A total of 380 mothers participated in this study, making a response rate of 94%. The median age of the participants was 28 years. The mean monthly incomes of respondents were 4381 (±1841 standard deviation (SD)) birr. More than three fourth (73.9%) of the participants were found within the age group of 25 to 34 years. About 62% of the study participants were Orthodox in religion. The majority (83.7%) of the mothers were married, and 43.2% had their own private business. About 57.9% of the respondents were completed primary and secondary school (Table 1).
Socio-demographic characteristics of mothers who gave birth at Yeka Sub-City health centers in Addis Ababa, Ethiopia, 2020.
Obstetrics characteristics of the respondents
Of the respondents more than half (61%) were primiparous. About 95% of the respondents gave birth through spontaneous vaginal delivery and almost all (96.6%) had ANC follow-up. The majority (92.4%) of the respondents replied that their current pregnancy was wanted. More than half (63.2%) of the study participants responded that privacy measures were not taken by birth attendants during delivery. About 67.6% of respondents reported that female birth attendants were assisted them during labor (Table 2).
Obstetrics characteristics of mothers who gave birth at Yeka Sub-City health centers in Addis Ababa, Ethiopia, 2020.

Maternal satisfaction with delivery services
Overall mothers’ satisfactions with delivery service were 63% (Figure 1) with a mean of 0. About 63 and standard deviation of 0.484 and the 95% confidence interval for the low and upper limit were 58.2 and 67.6, respectively.

Percent of mothers’ satisfaction with delivery services in public health centers at Yeka Sub-City, Addis Ababa, Ethiopia, 2020 (n = 380).
Response of mothers for selected delivery services
Mother’s satisfaction with the cleanliness of the delivery room was 69.5% and satisfaction related to availability, accessibility, and cleanliness of toilet was 58.4%. In this study, the satisfaction level of mothers with the privacy of delivery care processes was 73.9%. Satisfaction with the availability and cleanliness of the waiting room/area was 81.3%. Concerning comfort at the entrance to the health center, about 365 (96.05%) and 15 (3.95%) of mothers were satisfied and dissatisfied, respectively. The mean and standard deviation of comfort at the entrance were 4.02 and 0.377, respectively. In connection with the availability of drugs, 309 (81.3%) of mothers were satisfied, while 71 (19.7%) of mothers were dissatisfied. Regarding the cleanliness of rooms and beds, 313 (82.4%) of mothers were satisfied and 67 (17.6%) of mothers were dissatisfied. In addition, the mean and standard deviation of satisfaction and dissatisfaction with the cleanliness of rooms and beds were 3.88 and 0.499, respectively. Concerning the availability of laboratory service, 309 (81.3%) and 71 (18.7%) of mothers were satisfied and dissatisfied, respectively. The overall response of mothers for selected delivery services is presented in Table 3.
The proportion of mothers satisfied with delivery services who gave birth at Yeka Sub-City health centers in Addis Ababa, Ethiopia, 2020.

Factors associated with maternal satisfaction
In bivariable logistic regression, privacy measures taken at the delivery room, mothers’ education level, income, and admission time were associated with maternal satisfaction. In multivariable analysis privacy measures taken at the delivery room, mothers’ education level, occupational status of mothers, and family income level of mothers were associated with mothers’ satisfaction for the delivery services.
Mother’s income levels of 1501 to 5000 birr were satisfied with the service (AOR = 2.49; 95% CI: 1.3, 4.76). However, mothers whose income below1500 birr were less satisfied. Mothers whose privacy measures were not assured were less satisfied (AOR = 0.09; 95% CI: 0.05, 0.17) than those mothers whose privacy was assured. Participants whose occupation status was housewife were satisfied with the service offered by the health centers (3.18; 95% CI: 1.07, 9.50). Mothers who were governmental employees were less satisfied with the service provided by health facilities.
Participants who were illiterate and read and write were less satisfied with the delivery service (AOR = 0.2; 0.06-0.61). Mothers who were diploma and above in educational status were satisfied with the service (Table 4).
Factors associated with mother’s satisfaction with delivery services in Yeka Sub-City public health centers in Addis Ababa, Ethiopia, 2020.

Abbreviations: AOR, adjusted odds ratio; COR, crude odds ratio.
P < .005.
Discussion
The present study discussed important information about maternal satisfaction with delivery care services and its associated factors among mothers who gave birth at public health centers in the Yeka Sub-City, Addis Ababa, Ethiopia.
In this study, the overall satisfaction level of mothers with delivery services was 63%. Privacy measures at the delivery room, educational status of women, occupation status, and monthly income were factors associated with mother’s satisfaction with delivery services.
The findings of the present study were closer to the study conducted in referral hospitals in the Northwest part of Ethiopia (61.9%). 16 However, the present study was lower than those studies conducted at Felege Hiwot Referral Hospital, Ethiopia (74.9%), 19 in public health facilities in Gamo Gofa, Ethiopia (79.1%), 20 Public health facilities in Debre Markos (81.7%), 21 Mekelle, Ethiopia (79.7%). 22 This difference may be due to variations in the cleanliness of health facilities/delivery rooms/beds, the privacy of delivery care process and support, cast of services, respect by birth attendants, verbal encouragement and explanation of procedures by birth attendants, time spent to be seen by birth attendants, comfort of the waiting room, availability of clean toilet/rest-room, availability of bathroom, quality of services provided, and expectation of mothers.
However, this study’s findings were higher than those studies conducted in St Paul’s Millennium Medical College, Ethiopia (19%) 15 and Gandhi Memorial Hospital, Ethiopia (21%). 23 This difference might be unlike other health facilities there were a high number of client flow in referral and specialized and teaching hospitals. The other probable reason may be the set-up of higher medical institutions not be convenient for mothers due to the complexity of many available services and their costs.
Mothers whose privacy was not assured were less likely to be satisfied than those mothers whose privacy was assured. Another study, conducted in a public hospital in Mekelle town, Ethiopia, and in public health facilities of Omo Nada District, Jimma Zone, Ethiopia suggested that women expressed discomfort and diminishing satisfaction levels if privacy was not kept.22,24 This may be due to mothers being sensitive to privacy around services provided by birth attendants and environmental factors of health facilities.
In this study, mothers whose occupation status was housewife were more likely to be satisfied compared to mothers who were governmental employees. This finding was in line with a study conducted in Nepal. 25 This could be due to housewives being more ready for childbirth. In addition, such findings could be because mothers who have jobs feel economically comfortable and happier to enjoy childbirth.
Furthermore, the present study indicated that family income levels of respondents were significantly associated with maternal satisfaction with delivery services. Furthermore, in this study, mother’s income levels of 1501 to 5000 birr were 3 times more likely to be satisfied than mothers’ income less than 1500 birr. This might be due to the provider’s attitude to providing mother friendly service to each mother equally and might be due to availability of comprehensive service at the health centers, as well as this could be due to public health facilities service has been improved and clients difference in terms of socio-demographic status.
Moreover, this study showed an association between educational status and service satisfaction. This finding is in line with a study conducted in Hawassa. Ethiopia 26 and Nepal, 25 which stated that those women with higher education level (college or above) were more likely to be satisfied with the childbirth experience than women with an education of high school or less.
In addition, the present study revealed that mothers who had no formal education/illiterate were less likely to be satisfied with delivery services. In contrast, studies conducted in Hawassa, Ethiopia 26 and Nepal 25 stated that non-formal education and illiterate were more likely to be satisfied with delivery services. This might be due to the client’s expectations about availability and quality service at health centers and hospitals. This could also be due to differences in the socio-economic characteristics of study populations.
Conclusion
The overall satisfaction of mothers with delivery care service in the Yeka Sub-City public health centers was moderate. The income level of women’s educational status and occupation of participants were the predictors for women’s satisfaction with delivery services. Thus, there is a need to assess privacy measures taken in health facilities to assure women’s privacy and satisfaction with services offered by the birth attendants.
Footnotes
Acknowledgements
We would like to thanks Addis Continental Institute of Public Health for supporting us. Our deep gratitude goes to Yeka Sub City Health Office for support this study. We would like to thank the participants of this study.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study obtained fund from Addis Continental Institute of Public Health for data collection only. The authors declare that they have not received funds for the publication of this manuscript.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Conceived the idea: DE. Designed the methodology: DE, WW. Conducted the study: DE, WW, MT. Data analysis: DE, WW, MT. Interpreted data: DE, WW, MT. Wrote draft manuscript: DE. Wrote the final manuscript: DE, WW, MT. Review and edit: MT. Read and approved the final manuscript and agreed for submission: DE, WW, MT.
Ethical Approval and Consent to Participate
The study was reviewed and approved by Institutional Review Board of Addis Continental Institute of Public Health. Data were collected after written consent obtained from the study participants.
Availability of Data
The data supporting the findings of this study are available within the manuscript.