
Abstract
Evidence of variation in maternity health service practices has increased the government’s interest in quantifying and advancing the quality of institutional delivery care in the developing world, including Ethiopia. Therefore, we conducted a systematic review and meta-analysis to update and provide more representative data on women’s satisfaction with skilled delivery care and the associated factors in Ethiopia. This systematic review and meta-analysis followed the Preferred Reporting Items 2015 guideline. We searched PubMed/Medline, SCOPUS, Embase, Web of Science, and Google Scholar electronic databases for all 36 included studies. The pooled prevalence of women’s satisfaction with skilled delivery care and the associated factors were estimated using a random-effects model. Subgroup analysis and meta-regression were performed to identify the source of heterogeneity. Furthermore, publication bias was checked using eggers and funnel plots. All statistical analyses were performed using STATA version 14.0 software. The pooled prevalence of women’s satisfaction with skilled delivery care was 67.31 with 95% confidence interval (60.18–74.44). Wanted pregnancy (adjusted odds ratio = 2.86, 95% confidence interval: (2.24–3.64)), having a plan to deliver at a health facility (adjusted odds ratio = 2.09, 95% confidence interval: (1.42–3.09)), access to ambulance service (adjusted odds ratio = 1.52, 95% confidence interval: (1.00–2.31)), waiting time < 15 min (adjusted odds ratio = 3.66, 95% confidence interval: (2.51–5.33)), privacy assured (adjusted odds ratio = 3.94, 95% confidence interval: (2.23–6.94)), short duration of labour < 12 hr (adjusted odds ratio = 2.55, 95% confidence interval: (1.58–4.12)), proper labour pain management (adjusted odds ratio = 3.01, 95% confidence interval: (1.46–6.22)), and normal newborn outcome (adjusted odds ratio = 3.94, 95% confidence interval: (2.17–7.15)) were associated with women’s satisfaction. Almost two-thirds of women were satisfied with skilled delivery care. In comparison, the remaining one-third were not satisfied with the care. The quality of intrapartum care, unwanted pregnancy, lack of ambulance services, prolonged duration of labour, poor labour pain management, and complicated newborn outcome were factors affecting women’s satisfaction with skilled delivery care in Ethiopia. Therefore, strategies need to be developed to increase the satisfaction level by considering the abovementioned factors during routine delivery care.
Cover letter
Women’s satisfaction with skilled delivery care is critical for reducing maternal mortality and morbidity by avoiding negative experiences with the health care system to enhance subsequent maternal health services utilization. Providing satisfying delivery care for women has immediate and long-term effects on their health. It reduces the losses of women due to reasons related to pregnancy and childbirth, thus avoiding great social and personal tragedies of maternal death and morbidity. Therefore, this study aimed to estimate women’s satisfaction level with skilled delivery care and the associated factors in Ethiopia.
The findings of the study were reported using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2015 guideline. A random-effect model was used to estimate the pooled level of women’s satisfaction with delivery care. Eggers test and funnel plots were used to check publication bias. Subgroup analysis and meta-regression were performed to identify the source of heterogeneity.
The pooled women’s satisfaction level with skilled delivery care in Ethiopia was 67.31%. Factors associated with women’s satisfaction with skilled delivery care were wanted pregnancy, planned delivery at a health facility, ambulance service, privacy, short waiting time and duration of labour, proper management of labour pain, and healthy newborn outcomes. Therefore, addressing these factors is pertinent to increase women’s satisfaction with skilled delivery care, as maternal satisfaction had immediate and long-term effects on their health and subsequent use of maternal health services to reduce maternal morbidity and mortality.
Introduction
Globally, more than 500,000 women die every year from complications of pregnancy and childbirth. 1 Reducing maternal mortality and morbidity is a global problem, especially in developing countries like Ethiopia, 2 mainly attributed to poor maternity quality of care. 1 However, the availability of maternal health services does not guarantee the utilization and optimal outcomes for women. 3 Although healthcare coverage has dramatically improved in recent decades, institutional delivery remains persistently low, and maternal mortality remains high. 4 Despite efforts by Ethiopian governments to promote health institution-based delivery services, 85% of births have occurred at home. 5
Maternal satisfaction with skilled childbirth care is the most frequently reported indicator for assessing the quality of obstetric services. 6 Women’s satisfaction with delivery care is a multidimensional concept with the following aspects: availability of human resources, medicine, and supplies; perceived provider competency and emotional support; and physical environment of the delivery ward, quality of care, and the health status of the mother and the newborn.7–10
Satisfaction with skilled delivery care in childbirth is essential for women to develop return behaviour and use maternal health services. 11 Satisfying delivery care has a direct and long-term impact on women’s health. It reduces maternal deaths, thus avoiding major social and personal tragedies by improving the subsequent utilization of maternal health services. 12 In contrast, disrespect and abuse of women during childbirth are decisive factors to skilled delivery care utilization, especially in low- and middle-income countries. 13 According to a study conducted in the west and south Ethiopia, around 74.8% and 98.9% of women experienced disrespect and abuse during childbirth at health facilities and received non-respectful care, respectively.4,13 Client dissatisfaction at a public health facility causes parturient women to decrease the utilization of maternal health services. 8
Improving maternal satisfaction during delivery is essential to support the efforts of reducing maternal mortality. 1 As a result, the World Health Organization recommends monitoring and evaluating maternal satisfaction to improve the quality and efficiency of skilled delivery care. 3
In Ethiopia, different studies have been conducted to determine the prevalence of maternal satisfaction and associated factors. The prevalence of maternal satisfaction ranges from 18% 11 to 95%, 14 which shows a great variation across different geographical areas and periods. Regarding the associated factors, several factors such as maternal age,12,15–19 residence place,14,19–22 educational status,1,12,14,16,17,23–27 Ante-Natal Care (ANC) utilization,6,12,14,15,18,21,24,26 status of pregnancy,12,14,18,25,28,29 maternal outcome,25,28,30,31 presence of waiting area,18,22,28,32 presence of a clean toilet,12,18,22,27,33 having a plan to delivery at health facility,1,3,12,17,22,26,34,35 waiting time to be seen by obstetric caregivers(OCGs),1,12,14,19,23–26,28,29 labour pain management,26,27,32,36,37 respectful delivery care,22,27,31,32,34,38 means of transportation,14,25,27,32 opportunity to talk,27,38 newborn outcome,1,26,29,31 privacy during examinations,1,12,16,28–30,34,35 mode of delivery,1,3,19,25,29,32,36 payment for the services,23,36 and duration of labour3,6,16,29 were frequently and consistently reported as significant factors affecting woman satisfaction with skilled delivery care. In addition, many factors such as gravidity, delivery time, overall cleanness of health facility, competency of health caregivers, sex of birth attendant, newborn care, well-coming gate, health facility stay time after delivery, previous place of delivery, and availability of drugs have been reported in Ethiopia with wide discrepancy.1,3,6,8,11,12,14–42 Aside from the variability in women’s satisfaction with delivery services and associated factors, the nationally representative pooled data on maternal satisfaction with labour and delivery services in Ethiopia was not representative of all regions. Furthermore, the existing pooled data on the area was limited to a few studies. 43 Therefore, this systematic review and meta-analysis aimed to provide more current and representative national data on women’s satisfaction with skilled delivery care and the associated factors. The results of this study will be beneficial in adapting and implementing methods to meet SDG 3.1 that calls for global maternal mortality to reduce to less than 70 per 100,000 live births. Furthermore, identifying and addressing the factors influencing mothers’ satisfaction with their facility-based childbirth experience is the best strategy to improve delivery in health facilities in future pregnancies. 44
Method
Study design and search strategy
This systematic review and meta-analysis aimed to estimate the pooled satisfaction of women with skilled delivery care and the associated factors in Ethiopia. This systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Review and Meta-Analyses 2015 guideline. 45 We systematically searched international databases like PubMed/Medline, SCOPUS, Embase, and Web of Science to identify published articles. Moreover, we searched google scholar to identify published studies and grey literature. All published and grey studies until 10 February 2021 were retrieved for critical appraisal and assessed for inclusion in this review. The following search terms used using AND and OR Boolean operators to retrieve articles: (Women OR mothers OR maternal, OR clients) AND Satisfaction AND labour AND delivery AND ( ‘maternal satisfaction’ OR ‘women satisfaction’ OR ‘mothers satisfaction’) AND ( ‘Delivery service’ OR ‘Delivery care’ OR ‘labour and delivery care’ OR ( ‘labour and delivery service’ OR ‘childbirth services’ OR ‘delivery care services’ OR ‘intrapartum services’) AND ( ‘skilled delivery services’ OR ‘institutional delivery services’) AND ( ‘associated factors’ OR ‘predictors’) AND Ethiopia. The CoCoPop (Condition, Context, and Population) search strategy was used (Table 1).
Logic grid and example of database search to assess women’s satisfaction and the associated factors with skilled delivery care in Ethiopia.

Condition: Women’s satisfaction towards skilled delivery care, and the associated factors like ANC visit, waiting time to be seen by health caregivers, privacy during examinations, planned delivery visit, newborn outcome, maternal outcome, payment for the services, means of transportation, and so on. Population: All women who gave birth in Ethiopia. Context: This review was conducted among all women who gave birth at health institutions of Ethiopia.
Inclusion criteria and exclusion criteria
All community or health institution-based published and grey studies reporting women’s satisfaction with skilled delivery care or the associated factors in the English language until 10 February 2021 are included in this review. However, articles without full access and did not report the outcome of the interest were excluded. Initially, articles were assessed independently for inclusion through a title and abstract. Then, studies that passed the title and abstract review were also screened using the full text. In case of duplicated data, the full-text published article was retained.
Outcome of interest
The primary outcome of this study was women’s satisfaction with skilled delivery care and the associated factors in Ethiopia. Women’s satisfaction with institutional delivery care affects the choice of birthplace selection. It is vital to identify the gap between actual childbirth care and expected health care outcomes to reduce maternal mortality and improve the quality of delivery care.
Quality assessment and data extraction
The risk of bias included studies assessed using the Hoy risk of bias tool. 46 The three reviewers (Y.B., M.D., and K.A.B.) independently assessed and extracted the articles for overall study quality and inclusion in the review using a standardized data extraction format. The data extraction format included primary author, year of study, the study region, study design, sample size, level of woman satisfaction, and odds ratio of factors affecting maternal satisfaction on delivery care. Any disagreement between the reviewers was resolved through discussion and involving reviewers H.A., H.T., and H.M.
Data analysis
Data were extracted in Microsoft Excel and exported to STATA version 14.0 software for further analysis. The heterogeneity among studies was assessed using the I2 test statistic. 47 A random-effects model was used to estimate the pooled prevalence of satisfaction with skilled delivery care. We used funnel plot 48 and Egger et al.’s 49 test to check for publication bias. In addition, we performed meta-regression and subgroup analysis to identify the source of heterogeneity. The effect of the selected predictor variables was analyzed using meta-analysis. The findings of this meta-analysis were presented using forest plot and odds ratio (OR) with its 95% confidence interval (CI).
Results
Article selection
Of the 552 articles retrieved, 536 were published and 14 were grey literature. 14 Of these, 104 duplicated records and 409 articles were excluded through screening of the titles and abstracts. The remaining 39 studies were assessed for eligibility based on the inclusion and exclusion criteria. In addition, 2 studies were excluded from the total of 39 because the whole document could not be accessed,50,51 and the remaining one was excluded because it does not report the outcome of interest. 52 Finally, 36 studies were included in this systematic review and meta-analysis (Figure 1).

A flow chart of the 36 included studies in the systematic review and meta-analysis on women’s satisfaction towards skilled delivery care and the associated factors in Ethiopia.
Characteristics of the included studies
This study includes a total of 36 cross-sectional studies with 16,875 participants to estimate the pooled prevalence of women’s satisfaction with skilled delivery care and the associated factors. All the included studies were cross-sectional. From these, three were mixed,32,34,35 while one was a comparative cross-sectional. 41 More than 90% 33 were health institution-based studies. The study included a maximum sample size of 1483 women in the Oromia region 20 and a minimum sample size of 197 women at the University of Gondar Referral Hospital. 41 More than half of studies were conduc-ted in Amhara region3,15,19,21,24,27,28,31,40–42 and Oromia region.1,12,17,18,20,29,30,32,34,37 Seven of the studies were from Southern Nations, Nationalities, and Peoples Representative (SNNPR) region,6,8,14,16,23,35,36 and 5 in Addis Ababa.11,25,33,38,53 The remaining three studies were from Harar, 26 Tigray, 22 and Afar region. 54 The studies conducted in the SNNPR region 14 and Addis Ababa, 11 respectively, reported the highest, 95%, and the lowest, 19%, level of women’s satisfaction. Studies conducted after 2015 revealed the highest, 95%, 14 and lowest level, 19%, 11 of satisfaction among women. The study conducted in Oromia reported the lowest (92.60%), 18 and a 100% response rate was reported among studies in the Oromia, SNNPR, and Amhara region. More than three-quarters of the studies were conducted after 2015 (Table 2).
Characteristics of the 36 included studies in the meta-analysis, Ethiopia.

HC: Health Centre; Co.: Community; BH&HC: Both Hospital and Health Centre; SNNPR: Southern Nations, Nationalities, and Peoples Representative.
Women satisfaction with skilled delivery care
This systematic review and meta-analysis revealed that the pooled prevalence of woman satisfaction with skilled delivery care was 67.31 with 95% CI of (60.18–74.44) with significant heterogeneity between studies (I2 = 99.3, p = 0.001) (Figure 2). Therefore, subgroup analysis was conducted to identify the sources of heterogeneity by using study regions, year of study, and sample size.

Forest plot showed the pooled prevalence of women satisfaction with 95 % confidence intervals.
Subgroup analysis
In the subgroup analysis, the highest (76.30) and lowest (61.13) satisfaction levels were reported from the SNNPR and Amhara region, respectively. The highest (72.35) satisfaction level was also found in studies conducted in ⩽ 2015 years of study with a 95 % CI of (56.82–87.88) (Table 3).
Subgroup analysis of the pooled prevalence of women’s satisfaction, 95% CI, and heterogeneity estimate with a p value.

Other regions*: Tigray, Harar, and Afar. CI: confidence interval; SNNPR: Southern Nations, Nationalities, and Peoples Representative.
Sensitivity analysis
A sensitivity analysis was performed to determine whether or not individual studies influenced the pooled prevalence estimates. The sensitivity analysis result revealed that none of the studies influenced the overall pooled prevalence in a random-effects model (Figure 3).

Result of sensitivity analysis of the included 36 studies.
Publication bias
Egger’s test, with a p value of (p = 0.001), and asymmetry of funnel plot showed the presence of publication bias. To adjust this publication bias, the trim and fill analysis was done (Figure 4).
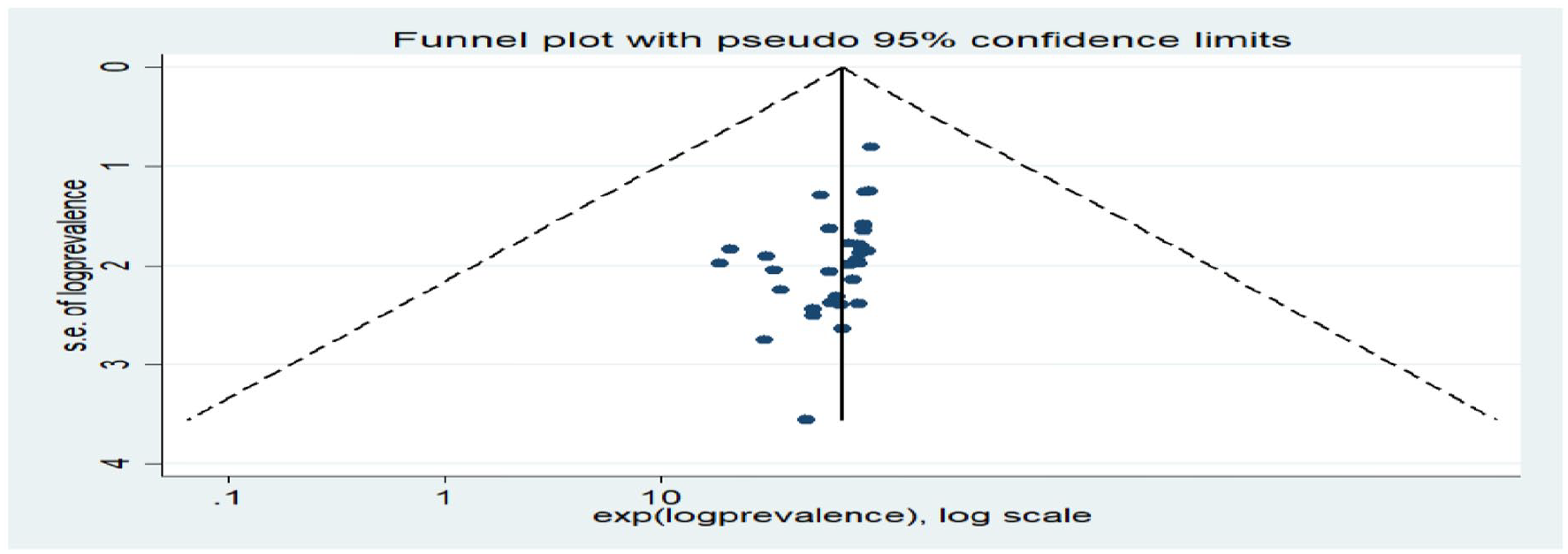
Funnel plot the test of publication bias.
Meta-regression
Meta-regression was performed to identify the source of heterogeneity using study/publication year and sample size as a covariate. However, the result showed that sample size and publication/study year were not significant to be considered, as the source heterogeneity (Table 4).
Meta-regression analysis of factors affecting between-study heterogeneity.

Factors associated with maternal satisfaction on skilled delivery care
This meta-analysis identified different factors associated with women’s satisfaction in delivery care in Ethiopia. Significantly associated factors were wanted pregnancy, planned delivery at a health facility, access to ambulance service, proper labour pain management, the short waiting time to be seen by OCGs, assuring privacy during examination, short duration of labour, and good newborn outcome. In addition, this meta-analysis revealed that the wanted pregnancy was associated with the satisfaction of women with skilled delivery care (adjusted odds ratio (AOR) = 2.86, 95% CI: (2.24–3.64)).
Women who planned to give birth at a health facility were 2.09 times more likely to be satisfied with skilled delivery care than those who did not (AOR = 2.09, 95% CI: (1.42–3.09)). In this meta-analysis, a positive association was observed between getting an ambulance service to arrive at a health facility and women’s satisfaction in skilled delivery care (AOR = 1.52, 95% CI: (1.00–2.31)).
This meta-analysis and systematic review revealed that the odds of women being satisfied by skilled delivery care were 3.66 more likely in those women who waited for ⩽ 15 min than women who waited for > 15 min to be seen by the OCGs (AOR = 3.66, 95% CI: (2.51–5.33)). It also revealed that women whose privacy was respected were 3.94 times more likely to be satisfied than those who did not privacy was not respected (AOR = 3.94, 95% CI: (2.23–6.94)).
In addition, women with a labour duration of < 12 hr were 2.55 times more likely satisfied with skilled delivery care compared to those women whose labour persist for more than 12 hr (AOR = 2.55, 95% CI: (1.58–4.12)). This meta-analysis stated that women whose labour pain was managed were 3.01 times more likely to be satisfied than women whose labour pain was not managed (AOR = 3.01, 95% CI: (1.46–6.22). Finally, good newborn outcome was positively associated with women’s satisfaction with skilled delivery care (AOR = 3.94, 95% CI: (2.17–7.15); Table 5).
The adjusted odds ratio between women’s satisfaction with skilled delivery care and the associated factors in Ethiopia, 2021.

Discussion
Although global efforts to decrease maternal mortality have been increased, maternal satisfaction and its associated factors also need to be addressed by a developing country. 10 This study reported that the pooled prevalence of Ethiopian women’s satisfaction in delivery services was 67.31%, with a 95% CI of (60.18–74.44). This finding is in line with a meta-analysis in low-income countries. 43 This result is also in line with studies conducted in India (68.7%) 55 and Pakistan (61%). 56 But this finding was higher than a study done in Jordan 17.8%, 57 Xiengkhuang province (38.6 %), 58 Nepal (56%), 59 Senegal (56%), 44 Kenya (54.5%), 60 Nairobi (56%), 61 Sudan (47.5%), 62 and Eritrea (20.8%). 63
On the other hand, this finding was lower than the studies conducted in India (79.2%), 55 Sweden (90%), 64 Serbia (81%), 65 Nepal (89.88%), 66 Saudi Arabia (89.5 %), 67 Mozambique (92.5%), 9 and Egypt (78.5%). 68 This might be due to the difference in the quality delivery service provided, women’s level of expectation and experiences, and a difference in socio-demographic characteristics of study participants. This may also be due to a difference in social and cultural factors that determine the perception of labouring women towards delivery care. A difference in the quality of services provided for labouring women across countries and type of health facilities contributed to this difference. Experience and prelabour expectations of women also determine maternal satisfaction with childbirth. 69
The subgroup analysis of this study revealed that the highest (76.30%) pooled prevalence was reported in the SNNPR region, followed by the Oromia region (69.26 %). This difference might be due to a difference in socio-demographic characteristics, expectations of women about childbirth quality of services, and differences in social and cultural norms of the women across the region.
Despite advancement and increased accessibility of maternal health services, the subgroup analysis based on year reported that maternal satisfaction was 72.35 % among studies conducted at or before 2015, greater than the later years with 66.09%. This discrepancy may be due to changing the perceptions and expectations about the quality of services by the labouring women who demand better quality childbirth care in a health facility over time. This might also be due to increased women’s awareness about the standard of delivery services increased maternal health services utilization. For instance, ANC utilization has increased from 28% in 2005 EDHS 70 to 74% in 2019 mini EDHS, 71 making women expect a better quality of delivery care. For women to be satisfied by the given delivery services, OCGs should consider the women’s expectations and provide consistent care. 66
In this meta-analysis, women who wanted their pregnancy were 2.60 times more likely to be satisfied than mothers who did not. A study conducted in Kenya supports this finding. 61 Thus, women’s dissatisfaction, worry, or ambivalence resulting from unwanted pregnancy was associated with reduced satisfaction, which might impair their perception of their birth experience and satisfaction. This meta-analysis revealed that women who planned to give birth at health institutions were 2.09 times more likely to be satisfied than those who did not. This might be due to having a plan to deliver at health facilities based on better knowledge about labour and delivery-related complications that contribute to a woman having more realistic expectations about the services than those who did not plan. Respectful and compassionate maternity care during the antenatal period may also increase women’s satisfaction during delivery. 43
Women who get ambulance service to arrive at health facility more likely to satisfy than women did not (AOR = 1.52). This result is supported by a study done in India. 72 This might be due to policies exempting women from direct payment for childbirth services results in women’s satisfaction. 73 Reduction in adverse pregnancy outcomes and access to skilled delivery care through emergency obstetric transportation contributes to an increased satisfaction rate of women. 74
This study revealed that women who waited for ⩽ 15 min were 3.66 times more likely to be satisfied with labour and delivery services than those who waited for > 15 min to be seen by the health caregivers. This finding is congruent with a study conducted in Bangladesh, 75 Bengal, 76 and Nepal. 59 This result was also consistent with a study in the Musandam region of Omanin which reported prolonged waiting time as a factor for dissatisfaction of clients with the services provided 77 and in Iran where 6.4% of women were disappointed by long waiting time until they have been seen by health caregivers. 78 This is due to reducing waiting times to be seen by health caregivers is mandatory for satisfying clients, 79 and longtime waiting creates a sense of ignoring among clients by health caregivers and health facility which may end up with dissatisfaction of clients. Moreover, longer waiting times can be associated with childbirth complications, such as stillbirth, death of a newborn, and maternal death, 80 and also impair the quality of services provided for women.
This review revealed that women whose privacy was assured were 3.94 times more likely to be satisfied than those whose privacy was not guaranteed. This finding was congruent with a review from developing countries. 81 Studies from Bangladesh, 75 India, 72 Ghana,73,82 and Uganda 83 also support this evidence. In addition, a survey in Eritrea revealed dissatisfaction towards service given was associated with a lack of adequate privacy measures during the examination. 63 This is because the obstetric caregiver process to perform physical examination affects women’s satisfaction level, 84 and privacy is an essential factor determining women’s satisfaction level with maternal care services. 10 Keeping privacy also was taken as respecting the women and their local culture and norms.
This meta-analysis found that the shorter duration of labour was associated with a higher rate of satisfaction among women (AOR = 2.55). This evidence is consistent with a study in Sweden. 85 The possible reason may be the negative effect of prolonged labour on birth outcomes and women’s experiences. 86 Mothers with prolonged labour are at risk of a negative birth experience. 87 This might also be because women with prolonged labour were more likely to be dissatisfied with repeated vaginal examinations and persistent labour pain.
A quasi-experimental study in Iraq supports this evidence. This meta-analysis found that women whose labour pain was managed were 3.01 times more likely to be satisfied than those whose women labour pain was not managed (AOR = 3.01). Women whose labour pain was managed was associated greater satisfaction with childbirth experience. 88 This finding is also in line with a study in Jordan, as inadequate labour pain relief was associated with low satisfaction. 57
Finally, according to this meta-analysis, women with good newborn outcomes were 3.94 times more likely to be satisfied than women with poor newborn outcomes. A study in Iraq supports this finding that women with healthy newborn outcomes were more satisfied. 81 This is because pregnant mothers want a normal baby, so if they deliver a baby without complications, the mother’s satisfaction will change, and they will become more satisfied. Having a healthy newborn can help to balance the negative experiences of childbirth.
Strength and limitation
This systematic review and meta-analysis attempted to include all regions and available evidence in Ethiopia to ensure the representativeness of the findings. The majority of the included studies were facility-based and cross-sectional, which may be considered a limitation. This review could be better interpreted if the limitations of the original studies were considered.
Conclusion
Although the Ethiopian government strives to increase skilled birth deliveries, only 67.31% of women were satisfied in institutional delivery care. This meta-analysis revealed that wanted pregnancy, having a plan to give delivery at a health facility, getting ambulance service, privacy, short waiting time and duration of labour, labour pain management, and healthy newborn outcome were factors associated with women’s satisfaction.
Therefore, responsible bodies should work to meet the expectations of labouring women by maintaining their privacy, reducing waiting time to be seen by health caregivers, and encouraging women to develop a birth plan to deliver at health institutions and avoid unwanted pregnancy to increase women’s satisfaction in the skilled delivery care. Also, measures should be taken to improve the quality of intrapartum care for a better newborn outcome, accessibility of ambulance services, and labour pain management.
Overall, this meta-analysis has the potential to be a very useful reference for planners of midwifery care in low-income countries to prevent preventable maternal and neonatal morbidity and mortality during childbirth and the postpartum period.
Supplemental Material
sj-doc-1-smo-10.1177_20503121211068249 – Supplemental material for A systematic review and meta-analysis of women’s satisfaction with skilled delivery care and the associated factors in Ethiopia
Supplemental material, sj-doc-1-smo-10.1177_20503121211068249 for A systematic review and meta-analysis of women’s satisfaction with skilled delivery care and the associated factors in Ethiopia by Keralem Anteneh Bishaw, Habtamu Temesgen, Haile Amha, Melaku Desta, Yibelu Bazezew, Temesgen Ayenew, Tewodros Eshete, Bekalu Bewket, Henok Mulugeta and Gebrehiwot Ayalew Tiruneh in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to thank all the authors included in this systematic review and meta-analysis.
Author contributions
KA, HT, TE, and HM were involved in the design, selection of study, statistical analysis, and developing the initial drafts of the article. KA, HA, MD, YB, and TA were involved in data extraction. All authors prepared and revised subsequent drafts. KA, HT, BB, and GA prepared the final draft of the article. Finally, all authors read and approved the final draft of the article.
Availability of data and material
All the datasets analyzed during this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.