
Abstract
Introduction:
Healthcare workers (HCWs) are at the frontline of COVID-19 control and prevention but also are high-risk groups for COVID-19 infection. The low level of knowledge and negative attitudes toward COVID-19 among HCWs can lead to inappropriate responding, wrong diagnoses, and poor practices for prevention. This research aims to examine the knowledge, attitudes, and practices regarding COVID-19 prevention and factors influencing the practices among HCWs in Daklak province, Vietnam.
Method:
A cross-sectional study was conducted among 963 HCWs working at district health centers and commune health stations through an online survey.
Results:
Overall, HCWs have good knowledge (91.3%), a positive attitude (71.5%), and appropriate practice (83.1%) regarding COVID-19 prevention. There was 89.6% of HCWs facing difficulties in practicing preventive measures such as felt difficult to change their habits (56.4%), insufficient personal protective equipment (PPE) (40.0%), and inconvenience to practice preventive measures (14.4%). The factors associated with implementing good practices are age group, residence, and knowledge about COVID-19.
Recommendation:
The Daklak Department of Health should provide additional training programs and guidelines about COVID-19 prevention and PPE for HCWs. More studies on risk and protective factors, and assessment about KAP regarding COVID-19 prevention at the post of the pandemic are needed.
Background
Novel Corona Virus Disease (COVID-19) rapidly has been transmitted around the world and has become a global pandemic, after the first cases reported in Wuhan, China in the last of December 2019. The World Health Organization (WHO) 1 announced COVID-19 as a global health pandemic on 11th March 2020. After 1 year of transmission, on 30th December 2020, the COVID-19 pandemic has affected 215 countries and territories around the world, resulted in more than 48 million cases and more than 1.8 million deaths. 2 The number of affected people is still daily increasing in many nations and new variants of the SARS-CoV-2, the virus which causes COVID-19, have been complexly mutating. 3 The COVID-19 pandemic becomes one of the biggest health, social, and financial crises ever before. The emergence and spread of COVID-19 cause fear, anxiety among the community. 4 Lacking knowledge, misinformation, and rumors have led to blame, stigma, discrimination, and inappropriate preventive behaviors. 5 To control the COVID-19 outbreak effectively, good knowledge, positive attitudes, and appropriate behaviors of COVID-19 prevention will be effective measures.
Healthcare workers (HCWs) at all levels are at the frontline defense against the COVID-19 pandemic. They have been facing serious occupational health risks when involving in caring for COVID-19 patients and testing suspected cases, especially during an early stage of the pandemic. They are at a high risk of COVID-19 infection because they are not only frequently exposed to infected individuals with inadequate isolation facilities and insufficient personal protective equipment but also work under high load within long hours, fatigue, and distress. 6 HCWs only represent <2% to 3% of the population worldwide, however, up to 14% of COVID-19 infections are among HCWs, even in some nations, 35% of cases are HCWs. 7 Controlling and Preventing COVID-19 transmission in health facilities becomes the priority because the pandemic will be out of control if HCWs also become patients. Knowledge of the epidemiological dynamics and transmission pathways can influence the attitudes and practices of HCWs. Insufficient knowledge and inadequate practices of HCWs can result in delayed diagnosis, incorrect treatment, and increase the risk of disease transmission in other patients, HCWs, and visitors. 7 Also, the knowledge, attitudes, and practices of COVID-19 prevention and treatment of HCWs also affect the behaviors of patients, visitors, and the general community.
Vietnam is one of the first countries in the world to detect COVID-19 cases outside of China. The first 2 patients (both traveled from Wuhan, China) reported in Vietnam was on 23 January, only 1 month after the first cases detected in China. By the end of 2020, the number of COVID-19 patients in Vietnam was 1456 cases with 35 deaths recorded. 8 In which, 14 doctors and medical staff in national hospitals have been infected. 9 The number of infected cases and deaths in Vietnam is relatively low compared to other countries in the world and the region although Vietnam is at a high-risk for disease transmission. Vietnam is a developing country with limited resources, a high population density (population over 97 million people with a density of 294 people/km2), and a disadvantaged health-care system. 10 Also, Vietnam was ranked as one of the top tourist destinations in Southeast Asia, with international arrivals reached over 15 million and domestic travels over 80 million each year (Dinh et al., 2019). 11
Amidst the current pandemic, the Vietnamese Ministry of Health has implemented training (online and face-to-face) and issued guidelines to raise knowledge and awareness for HCWs regarding the prevention and control of COVID-19. 12 Vietnam has conducted some studies about the level of awareness of COVID-19 among the general population, 13 university students, 14 and HCWs in a district hospital. 15 However, there is scarce information about COVID-19 understanding and risk perception among health staff at other levels. Therefore, more studies about facts of knowledge, attitude, and practice are needed to identify risky behaviors among HCWs. Given the importance of the issue, this study aims to describe the KAP toward COVID-19 of HCWs at district and commune levels during the early stage of the COVID-19 pandemic in Vietnam. The study’s findings will give suggestions to training, guidelines, and regulations to protect HCWs, to improve their capacity toward COVID-19 prevention, and to avoid occupational exposure during the COVID-19 pandemic as well as other disease outbreaks.
Methods
Data
This is a cross-sectional study design. The study sample was calculated using the 1-proportion sample size formula with a sample size was 692 people. Participants were selected using non-probability, self-nominated sampling. HCWs in this study include doctors, pharmacists, nurses, and other health staff working at district health centers and commune health stations in Daklak province, one of the highland provinces of Vietnam.
The questionnaire was posted on the HCWs’ network in Daklak province and to invite them to participate in the study. The online survey was conducted from April 2 to 9, 2020. The questionnaire included 3 main groups of KAP questions regarding COVID-19 prevention, which were based on guidelines of the Vietnam Ministry of Health, and some barriers of practices. The questionnaire was completed by 988 people, in which 25 records that had no sufficient information were excluded, leaving answers from 963 respondents (97.5% of the total respondents) for analyses.
Measures
The level of COVID-19 knowledge was assessed through eleven questions, including symptoms of the disease, key transmission routes, high-risk groups, the possibility of transmission of asymptomatic cases, treatment, and preventive measures. Each correct choice equates to 1 point, and higher scores mean higher levels of knowledge. There was a maximum of 23 points of knowledge. Participants had ⩾80% of correct choice (⩾18.4 scores) had a high level of knowledge, and those with less than 18.4 scores had a low level of knowledge. There were 8 questions related to the attitudes on COVID-19 prevention, equivalent to a maximum of 8 scores. Respondents who achieved equal to or higher than 6.4 scores (⩾80% of the total score) were classified as having a positive attitude while those who had lower scores than this cut-off point had a negative attitude. There was a total of 6 practical measures to help prevent COVID-19. HCWs who implemented all 6 measures were classified as sufficient practice. In contrast, those who did not apply at least 1 measure were classified as insufficient practice.
Analysis strategy
Both descriptive and inferential statistics were performed, and all independent variables were described under the main outcomes by calculating frequencies and percentages. A comparison of KAP according to demographic characteristics was performed (ANOVA test).
Binary logistic regression analyses were used to identify factors associated with practices (enter method). The dependent variable is the level of practice (2 values: 1-did all 6 measures, and 0-did less <6 measures); Variables were entered into the logistic regression model including: age group (⩾40; <40), sex (male, female), marital status (married, unmarried/other); ethnic (Kinh, other); education (undergraduate/graduate, lower), residence (urban, rural); occupation (5 occupational groups); working place (district, commune); knowledge level (high, low); perception of susceptibility of Covid-19 (yes; no); fear (yes; no); barriers of practice (yes; no). Data were analyzed using SPSS software (version 24). The statistical significance level was set at P < .05 (2-sided).
Results
Two-third of the respondents (669) were under 40 years old (69.5%); 67.7% were females and 32.3% males; 84% were married; 80.4% were Kinh ethnic people; 37.4% of HCWs were doctors and assistant doctors, 35.3% were nurses and midwives, and the remaining 27.3% were pharmacists, technicians, and administrative officers. One-half of HCWs worked in district health center (49.2%), while 50.8% worked at commune health stations. The demographic characteristics of respondents are shown in Table 1.
Demographic characteristics of the study respondents (n = 963).

Three main sources of COVID-19 information that HCWs accessed were Ministry of Health’s website, TV, and the Internet, with the rates were 97.7, 97.5, and 96.7, respectively. Other sources of information such as radio, newspapers, and relative/friends/colleagues also were frequently used with more than 80%. 83.8% of HCWs showed that the amount of provided COVID-19 information was about right, and 12.6% of those thought that it was too much. The remaining participants showed that it was too little or did not know (see Table 2).
The sources of COVID-19 information.

Knowledge, attitudes, and practices about the COVID-19.
The findings show that the average knowledge score of 963 participants was 20.39 with 91.3% (879 HCWs) had a high knowledge score (Table 3). There were significant differences of the mean score of knowledge between groups of sex, education, and occupation. Specifically, female health workers, HCWs with under/graduate level, and respondents who were doctors or technicians had better knowledge of COVID-19 than comparison groups (P < .05).
Knowledge score of COVID-19 by demographic variables (n = 963).

Attitudes
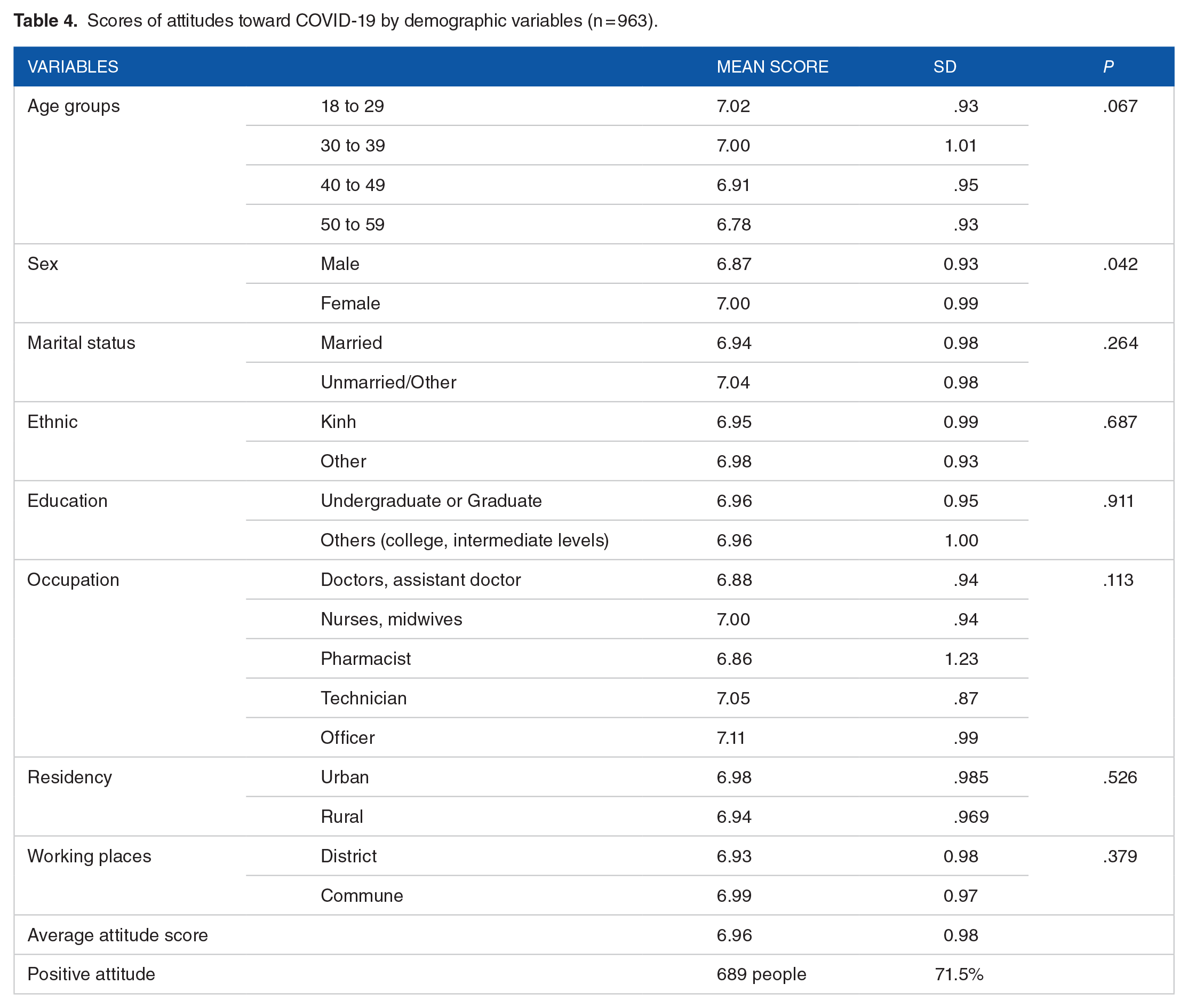
The total score of attitudes ranged from 0 to 8 with an average attitude score was 6.96. 71.5% of HCWs showed positive attitudes, and 28.5% of HCWs had negative attitudes about COVID-19 prevention (see Table 4). There was no significant difference related to attitudes within the age groups, education, occupation, residence, and working place. The only significant difference was found for gender. The attitude score of female staff was higher than their male counterparts (P = .042).
Scores of attitudes toward COVID-19 by demographic variables (n = 963).
Practices
Most of the HCWs (83.1%) carried out all 6 measures for preventing the COVID-19 while the remaining 16.9% of respondents had insufficient practice (Table 5). It means that 1 out of every 6 HCWs was not fully practicing COVID-19 preventive measures. Up to 89.6% of participants reported that they had barriers in practicing preventive measures. Specifically, among 863 HCWs who had difficulties to implementing measures, more than a half (56.4%) felt difficult to change their daily habits, 40% of them did not have enough personal protective equipment such as face masks (N95), gloves, face shields, gowns, and sanitizer. Other barriers were reported including inconvenience to practice these measures (14.4%), feeling uncomfortable (3%), and feeling unnecessary (1.7%).
Practices of participants to prevent COVID-19 and barriers of practices (n = 963).

Factors Influence to Practice of People
The output of the logic regression model just shows that the predicted percent of the model is 83.2%. Age groups, residence, and knowledge level were significantly associated with doing all 6 measures of Covid-19 prevention (Table 6). Groups of senior HCWs (aged 40 and higher), staffs who live in rural areas, and those who had good knowledge of COVID prevention were more likely to practice all 6 measures of prevention rather than comparison groups. HCWs met barriers of COVID-19 prevention were more likely to practice insufficient measures of prevention but the association was not significant clearly (OR = 0.5, P = .056).
Associated factors of practice level (n = 963).

Discussion
The study evaluated the knowledge, attitude, and practice regarding COVID-19 of 963 HCWs working at district health centers and commune health stations in Daklak province, Vietnam. In general, participants had good levels of knowledge, positive attitudes, and appropriate practices toward COVID-19 control and prevention. The results revealed that 91.3% of HCWs had a high level of knowledge about COVID-19, 71.5% of HCWs had a positive attitude toward the prevention and control of COVID-19 and 83.1% carried sufficiently protective measures. These outcomes were higher compared to those reported in a study among HCWs in the Amhara region, Ethiopia, 16 but were similar to the results of a study in China 17 and another study in Pakistan. 18 Comparing to previous studies in Vietnam, the study findings were in agreement with the results of studies among HCWs in Hochiminh city 15 and the Vietnamese general population 13 that reported high levels of knowledge and practices regarding COVID-19. The reasons could because of successes in risk communication for COVID-19 prevention and control in Vietnam. 19 This contributed to increasing the knowledge and practices of the community and HCWs in particular.
The findings also illustrated that the discrepancies in knowledge, attitudes, and practices were significantly different across sub-groups of HCWs. For instance, the level of knowledge of male HCWs was significantly higher than their female counterpart, while the mean score of positive attitudes among males was lower than females. Regarding factors affecting practices, age, residency, and knowledge level had significantly associated with doing all 6 measures of COVID-19 prevention. These findings were quite similar to a recent study by Van Nhu et al, 13 which reported that marital status, gender, age group, knowledge, and fear significantly influenced the practicing of COVID-19 prevention among the general community.
The study findings also showed that more than 97% of the HCWs received COVID-19 information from television and the Ministry of Health websites as a primary source. This indicates that updated and transparent information about the COVID-19 pandemic on official channels had positive implications for improving knowledge for HCWs. However, there were 96.7% and 83.7% of HCWs often received the COVID-19 information from the Internet and family/friends, respectively. It is noted that a lot of information on the Internet and word-of-mouth communications are less authentic sources for information, that may be inaccurate, unverified, and can misguide. It could be a reason that up to 12.6% of HCWs thought that the information about the COVID-19 was too much, and 16.9% of HCWs have not applied sufficient preventive measures. Therefore, HCWs should be warned against fake news and should consult reliable sources such as WHO, US CDC, and Ministry of Health. The Ministry of Health should provide comprehensive training programs and guidelines about COVID-19 for HCWs.
It is noted that besides knowledge, attitudes, and practices, many other factors may influence the risk of COVID-19 infection. For example, the frequency of hazard exposure, the availability of material support, the level of work stress. Therefore, more research on risk and protective factors for COVID-19 is needed. Furthermore, this study was conducted in the early stage of the pandemic (April 2020), thus the levels of knowledge, attitudes, and practices toward COVID-19 prevention may change over time. It is necessary to have a reassessment about KAP among HCWs to compare the differences between early and post of the pandemic.
Limitations
The research has some limitations that need to be mentioned. This was an online cross-sectional study conducted during the pandemic. Therefore, a high percentage of HCWs may be too busy to participate. Also, the research was undertaken rapidly to provide an understanding of the COVID-19 in Vietnam, therefore it may not describe changes in knowledge and practices within the pandemic progresses. Also, information conducted in the study base on the self-report of participants that was influenced by the participants’ honesty and recall ability. Additionally, the limitation related to the online survey such as unable to calculate a response denominator. Despite these limitations, the study results provided useful information about the knowledge, attitudes, and practices of HCWs about COVID-19.
Conclusion
The study indicates that at the early stage of the COVID-19 pandemic, HCWs at the district and commune levels in Daklak province, Vietnam had good KAP regarding COVID-19 prevention. This was one of the results of the Vietnamese government’s efforts in COVID-19 control and prevention, as well as risk communication in the early stage of the pandemic. Also, good KAP of HCWs contributed to success in COVID-19 response in Vietnam. Additional guidelines and health education programs for HCWs and the general community are necessary to implement and maintain safe practices. In addition to providing adequate personal protective equipment for HCWs, in-depth studies on risk and protection factors, as well as comparisons of KAP during and after the pandemic, are needed.
Footnotes
Acknowledgements
The authors thank all the participants involved in this study for their time to share their knowledge and experiences toward COVID-19 prevention. The authors express special thanks to the directors of the Daklak Provincial Health Department and the CDC for their supports in organizing data collection.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
HVN, TQT, TTTH and TNQL designed the study. HVN, TQT and HHP organized data collection; TQT, HVN and HHP conducted the data analyses. TTTH and TNQL drafted the manuscript. All the authors made critical revisions and agreed on the final version of the manuscript. TQT, TNQL and TTTH reviewed the final manuscript and approved it for submission, which was done by TTTH.
Ethical Approval and Consent to Participate
This study was approved by the Institutional Review Board of the Hanoi University of Public Health under Decision No. 129/2020/YTCC-HD3 dated the 1st April 2020. The study information about objectives, selection criteria, personal information privacy, data protection, advantages, and potential harm were provided to participants before conducting the survey. Each participant was assigned a study number, no private data was collected, and all collected data was coded.
Data Accessibility Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.